Mastering Microvascular End-to-Side Anastomosis and Vein Grafting
Key Takeaway
Microvascular end-to-side anastomosis and interpositional vein grafting are indispensable techniques in complex orthopaedic reconstruction, replantation, and free tissue transfer. These procedures ensure tension-free vascular repairs while preserving distal perfusion in critical recipient vessels. This comprehensive guide details the biomechanical principles, precise step-by-step surgical execution, and postoperative management required to achieve optimal patency rates and prevent catastrophic microvascular thrombosis.
Comprehensive Introduction and Patho-Epidemiology
Microvascular surgery represents the absolute pinnacle of reconstructive orthopaedics and traumatology, providing the technical foundation for complex limb salvage, major digit and extremity replantation, and composite free tissue transfer. The evolution of microsurgery from a highly experimental endeavor to a reliable, standard-of-care surgical discipline has fundamentally altered the management algorithms for severe musculoskeletal trauma, oncologic resections, and congenital deformities. While standard end-to-end anastomosis remains the workhorse technique for vessels of equal caliber and sufficient length, the complex realities of the traumatized extremity frequently preclude this straightforward approach. In high-energy trauma—such as Gustilo-Anderson Type IIIB and IIIC open fractures—the zone of injury often extends far beyond the visible wound, necessitating the resection of severely contused or avulsed vascular segments to reach healthy, uncompromised intima.
The patho-epidemiology of severe extremity trauma dictates that surgeons must be prepared to manage massive soft tissue deficits coupled with critical ischemia. Ischemia-reperfusion injury introduces a profound physiological insult, characterized by the generation of reactive oxygen species, endothelial dysfunction, and the potential for the "no-reflow" phenomenon. When vascular gaps exist, or when primary end-to-end repair would induce longitudinal tension, the surgeon must pivot to advanced reconstructive techniques. Microvascular end-to-side anastomosis and interpositional vein grafting are indispensable strategies in the microsurgeon's armamentarium, specifically designed to bypass extensive zones of injury, bridge significant anatomical gaps, and preserve critical distal perfusion in extremities with limited vascular runoff.
The decision to employ an end-to-side anastomosis is frequently driven by the anatomical and hemodynamic necessity of preserving a major recipient axis. For instance, in a traumatized lower extremity with only a single patent tibial vessel (e.g., a solitary posterior tibial artery), sacrificing that vessel for an end-to-end flap anastomosis risks catastrophic distal ischemia and limb loss if the anastomosis fails or if the flap's vascular resistance alters the distal hemodynamics. By utilizing an end-to-side configuration, the surgeon taps into the side of the source vessel, maintaining the critical axial flow to the foot while simultaneously perfusing the transplanted tissue. This technique demands an exceptional degree of technical precision, as the geometry of the arteriotomy and the subsequent suturing must perfectly accommodate the altered flow dynamics without inducing thrombogenic turbulence.
Similarly, interpositional vein grafting is the definitive solution for the fundamental microsurgical axiom: "Tension is the enemy of patency." When vessel ends cannot be approximated without tension, and skeletal shortening is either contraindicated (to preserve limb length and function) or insufficient, a vein graft must be harvested to bridge the defect. The pathophysiology of tension on a microvascular repair is well-documented; longitudinal strain narrows the vessel lumen, disrupts the delicate endothelial monolayer, and exposes highly thrombogenic subendothelial collagen and tissue factor, rapidly initiating the intrinsic coagulation cascade. Mastering these advanced techniques requires not only technical dexterity but a profound, granular understanding of vascular hemodynamics, endothelial biology, and the complex interplay of Virchow’s Triad within the microcirculation.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of vascular microanatomy and fluid biomechanics is the prerequisite for achieving high patency rates in complex microvascular reconstructions. The arterial and venous walls are composed of three distinct histological layers: the tunica intima, tunica media, and tunica adventitia. The tunica intima consists of a single layer of endothelial cells resting on a basal lamina. These endothelial cells are not merely a passive conduit; they are highly active endocrine organs that secrete nitric oxide (a potent vasodilator) and prostacyclin (an inhibitor of platelet aggregation), while maintaining a negatively charged glycocalyx that repels circulating platelets. Any mechanical disruption of this layer—whether through crush injury from forceps, thermal damage from cautery, or desiccation—instantly converts the vessel from an antithrombotic conduit to a highly thrombogenic surface.
The tunica media, composed of circumferentially arranged smooth muscle cells and elastic fibers, is responsible for the vessel's vasomotor tone. In traumatized or mechanically irritated vessels, profound vasospasm can occur, mediated by the release of endothelin and the influx of intracellular calcium within the smooth muscle cells. The tunica adventitia is the outermost layer of connective tissue, containing the vasa vasorum and sympathetic nerve fibers. While the adventitia must be meticulously stripped from the immediate anastomotic site to prevent it from being dragged into the lumen (which would precipitate immediate thrombosis), over-stripping can devascularize the vessel wall, leading to late necrosis and pseudoaneurysm formation.
Hemodynamically, microvascular flow is governed by Poiseuille’s Law, which states that flow rate ($Q$) is directly proportional to the pressure gradient ($/Delta P$) and the fourth power of the vessel radius ($r^4$), and inversely proportional to fluid viscosity ($/eta$) and vessel length ($l$). The formula, $Q = /frac{/pi /Delta P r^4}{8 /eta l}$, underscores the absolute criticality of the vessel radius. Even a microscopic narrowing of the anastomotic lumen—whether due to tension, purse-stringing of sutures, or intimal hyperplasia—will result in an exponential decrease in blood flow. Furthermore, the transition from laminar to turbulent flow is predicted by the Reynolds number. In an end-to-side anastomosis, the angle of incidence between the donor and recipient vessels profoundly affects this turbulence. An oblique angle (45 to 60 degrees) is biomechanically superior, as it minimizes flow separation, reduces the boundary layer stagnation zones, and limits the shear stress on the posterior wall of the recipient vessel.
Conversely, an orthogonal (90-degree) anastomosis creates significant flow disturbances. The blood stream impacts the posterior wall of the recipient vessel at a perpendicular angle, creating a "water hammer" effect that increases localized shear stress. This abnormal shear stress can induce endothelial injury and stimulate smooth muscle cell proliferation, leading to long-term intimal hyperplasia and delayed graft failure. When utilizing vein grafts, the surgeon must also account for the biomechanics of venous valves. Veins contain delicate, bicuspid valves designed to ensure unidirectional flow toward the heart. When a vein is harvested for arterial reconstruction, it must be reversed end-for-end. If not reversed, the arterial pressure will instantly snap the valves shut, completely occluding flow and leading to immediate reconstructive failure.
Exhaustive Indications and Contraindications
The selection of the appropriate microvascular technique requires a nuanced evaluation of the patient's systemic physiology, the local zone of injury, and the specific anatomical constraints of the recipient site. End-to-side anastomoses and vein grafting are not universally applicable; they possess distinct indications and absolute contraindications that must be rigorously respected to ensure limb salvage and flap survival.
End-to-side anastomosis is unequivocally indicated when there is a severe size mismatch between the donor and recipient vessels (typically a ratio greater than 2:1 or 3:1), where an end-to-end repair would result in severe turbulent flow, bottlenecking, and inevitable thrombosis. It is also the absolute standard of care when reconstructing a traumatized extremity that relies on a single patent runoff vessel. For example, in a severe lower extremity crush injury where the anterior tibial and peroneal arteries are occluded, the posterior tibial artery becomes the sole source of perfusion to the foot. Transecting this vessel for an end-to-end flap anastomosis is contraindicated; an end-to-side anastomosis to the posterior tibial artery preserves the critical distal axial flow while successfully vascularizing the free tissue transfer.
Interpositional vein grafting is indicated whenever an end-to-end anastomosis cannot be achieved without longitudinal tension. This scenario frequently arises in high-energy trauma where extensive segmental vessel loss has occurred, or when the zone of injury dictates that the recipient vessels must be debrided aggressively back to healthy, unbruised intima. Vein grafts are also utilized in complex replantations (such as major limb or multi-digit amputations) where bone shortening is either anatomically impossible or functionally devastating. Furthermore, vein loops (arteriovenous loops) can be constructed in a primary stage to bring robust vascular inflow and outflow to a severely traumatized, vessel-depleted bed, allowing for a secondary free flap transfer once the patient has stabilized.
Contraindications for these advanced techniques are both systemic and local. Systemic contraindications include profound hemodynamic instability, uncorrectable coagulopathy, or severe systemic atherosclerosis that precludes the availability of healthy recipient vessels. Local contraindications for end-to-side anastomosis include a heavily calcified recipient artery that will shatter or dissect upon arteriotomy, or a recipient vessel that is deeply embedded in a heavily irradiated or infected bed. For vein grafting, the lack of suitable donor veins (due to prior harvesting, deep vein thrombosis, or severe superficial phlebitis) represents an absolute contraindication.
| Clinical Parameter | End-to-Side Anastomosis | Interpositional Vein Grafting |
|---|---|---|
| Primary Indications | Size mismatch > 2:1; Single-vessel runoff extremity; Preservation of distal axial flow. | Segmental vessel loss > 2cm; Inability to achieve tension-free end-to-end repair; Bypassing zone of injury. |
| Relative Indications | End-to-end technically difficult due to deep anatomical constraints; Flow-through flap designs. | Replantation requiring preservation of skeletal length; Creation of AV loops for staged reconstruction. |
| Absolute Contraindications | Heavily calcified/atherosclerotic recipient vessel wall; Severe recipient vessel vasospasm. | Lack of viable donor veins; Placement of graft through an actively infected, purulent wound bed. |
| Relative Contraindications | Lack of adequate microsurgical instrumentation for precise arteriotomy. | Significant size mismatch between vein graft and recipient/donor vessels without geometric compensation. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful microvascular reconstruction. The process begins with comprehensive vascular imaging. While clinical examination and handheld Doppler assessment are foundational, complex reconstructions often demand advanced imaging modalities such as Computed Tomography Angiography (CTA) or Magnetic Resonance Angiography (MRA). These studies allow the surgeon to map the entire vascular tree, identify the precise level of vascular injury, delineate the zone of trauma, and confirm the patency of distal runoff vessels. In cases of chronic ischemia or highly complex trauma, conventional digital subtraction angiography (DSA) may be required to dynamically assess flow rates and identify subtle collateral networks.
Templating involves mapping the planned free flap or replant against the recipient site to determine the exact required pedicle length and the optimal geometry for the anastomosis. The surgeon must anticipate whether an end-to-side configuration will be geometrically feasible or if a vein graft will be required to bridge the anatomical distance. Donor sites for vein grafts must be evaluated preoperatively. The great saphenous vein, lesser saphenous vein, cephalic vein, and basilic vein are standard conduits. In digital replantation, the superficial veins of the volar forearm or the dorsal venous arch of the foot provide excellent caliber matches. These veins should be mapped with a duplex ultrasound or marked clinically prior to the induction of anesthesia, as sympathetic blockade and volume shifts during surgery can make them difficult to identify later.
Patient optimization is critical and revolves around the physiological triad of microsurgery: normothermia, euvolemia, and optimal hemodynamics. The patient must be kept strictly normothermic (core temperature > 37°C) throughout the perioperative period. Hypothermia induces profound peripheral vasoconstriction, shunting blood away from the extremities and drastically reducing flow through the microvascular anastomosis. The operating room ambient temperature should be elevated (typically above 24°C / 75°F), and active warming measures (forced-air warming blankets, warmed intravenous fluids) must be employed. Hemodynamically, the patient should be maintained in a hyperdynamic state with aggressive intravenous hydration to optimize cardiac output and maintain a brisk capillary flow. The use of systemic vasopressors (e.g., norepinephrine, phenylephrine) is generally discouraged, as they induce splanchnic and peripheral vasoconstriction that can compromise flap perfusion; if blood pressure support is required, volume expansion is the preferred initial intervention.
Positioning and ergonomics are paramount for the microsurgeon. Microvascular anastomosis requires absolute stillness and the elimination of physiological tremor. The patient must be positioned securely on a stable operating table, and the extremity must be immobilized. The surgeon must be seated comfortably, with the back supported and both forearms resting solidly on the operating table or an arm board. The operating microscope must be positioned to allow a neutral cervical spine posture for the surgeon. High-quality optics with dual viewing heads, foot-pedal controls for zoom and focus, and a focal length that accommodates the required instruments are mandatory. The armamentarium should be laid out meticulously, including non-toothed jeweler's forceps (typically #3, #4, or #5), Castroviejo needle holders, micro-adventitial scissors, Acland microvascular approximator clips, and a selection of 8-0 to 10-0 monofilament nylon sutures with spatulated or taper-point micro-needles.
Step-by-Step Surgical Approach and Fixation Technique
The execution of advanced microvascular techniques demands absolute concentration, flawless tissue handling, and strict adherence to a systematic sequence. The term "fixation" in this context refers to the precise, secure structural coaptation of the vascular elements—whether anchoring a flap pedicle to a major recipient axis or securing an interpositional vein graft—ensuring mechanical stability against arterial pressure while maintaining perfect intimal alignment.
The procedure begins with the exposure and preparation of the recipient vessel. Operating initially under surgical loupes (3.5x to 4.5x magnification) and subsequently transitioning to the operating microscope, the recipient artery or vein is carefully dissected from its surrounding fascial attachments. Proximal and distal control is achieved using double-sliding Acland microvascular clips. The adventitia, the highly thrombogenic outer layer, must be meticulously stripped from the planned anastomotic site over a distance of 5 to 8 millimeters. This is achieved by grasping the adventitia with jeweler's forceps, applying gentle traction, and sharply excising it with micro-scissors, ensuring the underlying tunica media is not scored or damaged.
For an end-to-side anastomosis, the creation of the arteriotomy (or venotomy) is the most critical step. Using a micro-scalpel or the sharp point of micro-scissors, a precise ellipse of the vessel wall is excised.
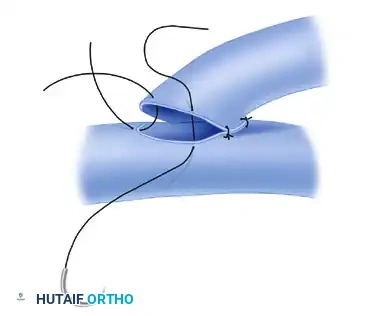
It is imperative that this defect is a true ellipse and not merely a longitudinal slit. A simple slit will pucker and gape irregularly under arterial pressure, distorting the geometry of the anastomosis and creating a highly thrombogenic nidus. The donor vessel is then prepared by cutting its end obliquely (typically at a 45 to 60-degree angle) to perfectly match the dimensions of the recipient arteriotomy. This oblique cut increases the cross-sectional area of the anastomosis, accommodating flow and minimizing turbulence.
The suturing sequence for an end-to-side anastomosis begins with the placement of the anchor sutures, universally referred to as the "heel" and "toe" stitches.

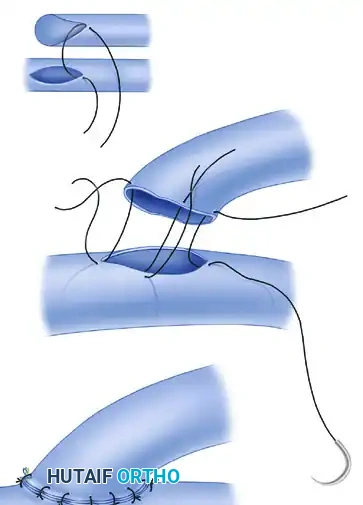
These two sutures are placed at the extreme apices of the elliptical opening. They are tied and the ends are deliberately left long to serve as traction stays. By applying gentle, opposing traction on these stay sutures, the anterior wall of the anastomosis is elevated and pulled taut, effectively separating it from the posterior wall. This geometric manipulation is crucial for preventing the most dreaded complication of this technique: inadvertent suturing of the posterior wall.
With the heel and toe sutures providing structural stability, the surgeon proceeds to suture the anterior wall.

Interrupted 8-0 or 9-0 nylon sutures are placed sequentially, ensuring full-thickness bites that perfectly coapt the delicate intimal surfaces. The needle must enter the vessel wall at a perfect 90-degree angle to minimize tissue trauma. Once the anterior wall is completed, the vessel is gently rotated (if anatomical mobility permits) or the microscope is angled to visualize the posterior wall. The posterior wall is then sutured with equal precision. The surgeon must constantly visualize the lumen, utilizing a micro-vessel dilator or continuous heparinized saline irrigation to ensure the back wall is not caught in the suture loop.
Upon completion of the suture line, the microvascular clips are released to verify flow and structural integrity.
The distal clip on the recipient vessel is released first to assess for retrograde flow and identify any major anastomotic leaks, followed by the release of the proximal clip to restore full arterial pressure. A successful anastomosis will demonstrate immediate, pulsatile expansion of the donor vessel. Minor needle-hole bleeding is common and should be managed with gentle, sustained pressure using a cottonoid pledget; additional sutures should only be placed for pulsatile, structural leaks, as every additional needle pass causes further endothelial trauma.
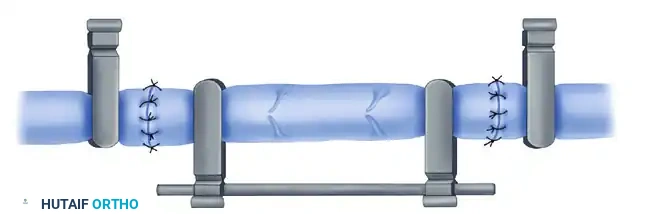
When an end-to-end or end-to-side anastomosis cannot bridge the gap without tension, a vein graft is required. The defect is first measured accurately with the limb in its anatomical, neutral resting position.

The appropriate donor vein is harvested using a strict "no-touch" technique, grasping only the periadventitial tissue. Small side branches must be managed meticulously; they should be ligated with micro-clips or tied with fine silk. If bipolar electrocautery is used, it must be applied well away from the main trunk of the vein, as lateral thermal spread will cause focal full-thickness necrosis of the vein wall, leading to inevitable graft blowout or thrombosis.
Crucially, the orientation of the harvested vein graft must be managed based on its intended function.
If the vein is being used to bridge an arterial defect, it must be reversed end-for-end to ensure the venous valves do not obstruct arterial flow. If used for venous reconstruction, it must remain in its native anatomical orientation. The graft is gently flushed with heparinized Ringer's solution to dilate the vessel, check for leaks, and clear micro-thrombi.
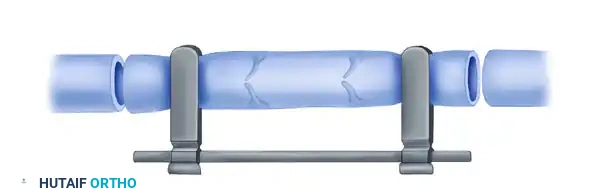
The anastomotic sequence for a vein graft is highly specific to prevent kinking and redundancy.
The proximal anastomosis is performed first using standard microvascular techniques. Once completed, the proximal vascular clamps are briefly released. This allows the arterial pressure to forcefully dilate the vein graft, revealing its true, pressurized length and confirming robust flow. The clamps are reapplied, and the graft is meticulously trimmed to the exact required length to reach the distal recipient vessel without any redundancy. Redundancy is catastrophic, as the pressurized graft will kink, creating severe turbulence and immediate thrombosis. The distal anastomosis is then completed, and flow is restored across the entire reconstructed segment.
Complications, Incidence Rates, and Salvage Management
Despite flawless surgical execution, microvascular reconstruction remains fraught with potential complications. The vast majority of microvascular failures occur within the first 48 to 72 hours postoperatively, corresponding to the peak period of endothelial reactivity, platelet aggregation, and edema formation. The primary complication is anastomotic thrombosis, which can occur on either the arterial or venous side of the reconstruction. Arterial thrombosis typically presents as a pale, cool flap or digit with absent capillary refill and loss of Doppler signals. Venous thrombosis, which is statistically more common due to the lower pressure and slower flow rates of the venous system, presents as a swollen, engorged, purple or blue flap with brisk but excessively dark capillary refill.
Vasospasm is another critical complication, characterized by a sudden, profound constriction of the vessel's smooth muscle layer. This can be triggered by mechanical irritation, hypothermia, hypovolemia, or the presence of fresh blood (which contains potent vasoconstrictors like serotonin and thromboxane A2) outside the vessel wall. Vasospasm dramatically reduces the vessel radius, exponentially decreasing flow according to Poiseuille’s Law, and can precipitate secondary thrombosis if not rapidly reversed. Late complications, occurring weeks to months postoperatively, include intimal hyperplasia (particularly at the site of an end-to-side anastomosis or a size-mismatched vein graft), pseudoaneurysm formation due to adventitial devascularization or unrecognized infection, and accelerated atherosclerosis within vein grafts exposed to arterial pressures.
Salvage management requires an aggressive, protocol-driven approach. "Time is tissue" in microvascular surgery. If thrombosis is suspected based on clinical examination or monitoring adjuncts, immediate return to the operating room for surgical re-exploration is mandatory. Non-operative management with systemic anticoagulants is universally ineffective for established microvascular thrombi and only delays definitive care. Upon re-exploration, the anastomosis must be taken down. The thrombus is evacuated, often utilizing a size
