Unlock better THA: The technique of short stem for less invasiveness

Key Takeaway
We review everything you need to understand about Unlock better THA: The technique of short stem for less invasiveness. The technique of short conservative femoral prostheses in total hip arthroplasty encompasses various design philosophies. These include trapezoidal stems engaging the lateral cortex, femoral neck-sparing curved designs for triplanar stability, bulky stems utilizing the lateral trochanteric flare, and short tapered stems. These designs aim for bone preservation and optimized biomechanics.
Introduction and Epidemiology
Total hip arthroplasty (THA) is one of the most successful and cost-effective procedures in all of medicine. With well-designed prostheses, the vast majority of patients enjoy reliable clinical outcomes and good implant survivorship. Nevertheless, advances in technology and improved understanding of the biomechanical nuances of THA have driven manufacturers and surgeons alike to continually strive for better results. One area of longstanding focus has been the design of the femoral component. Unresolved issues such as stress-shielding, proximal-distal morphology mismatch, and tissue-sparing surgery have given rise to a generation of conservative femoral prostheses.
Standard length cementless femoral components generally abide by one or a combination of three main philosophies for shape and fixation. Anatomic prostheses are designed to match or so-called “fit-and-fill” the proximal femur. Using a combination of reaming and broaching, the host bone is prepared to accept the stem for not only a tight fit for initial stability, but also maximal fill of the metaphyseal endosteal space. Cylindrical, extensively-coated stems rely not on proximal fixation for initial stability, but rather distal fixation via a “scratch fit” between the prosthesis and a slightly under-reamed femoral canal. Tapered stems rely on proximal fixation, but in comparison to anatomic prostheses, they are wedge-shaped and do not completely fill the metaphyseal space. After compaction broaching of the proximal cancellous bone, the tapered stem allows for self-seating for axial stability and achieves rotational control by virtue of its rectangular cross-sectional shape in an ellipsoid canal.

Excluding true resurfacing implants, there are several different design philosophies for conservative femoral components. The Mayo Conservative Hip was developed in the 1980s and has a trapezoidal coronal shape. It engages the lateral femoral cortex in order to resist varus-valgus stress and aims to achieve multiple-point contact within the irregularly shaped proximal femoral cavity. Short, femoral neck-sparing curved designs, such as the Collum Femoris Preserving prosthesis, aim for triplanar stability by blocking rotational and varus-valgus movements with an intact cortical cylinder of neck. Short, bulky designs that do not spare the neck, such as the Proxima prosthesis, engage the lateral trochanteric flare in order to utilize the lateral femoral column to transmit weight-bearing loads. Finally, short tapered stems such as the TaperLoc Microplasty rely on the same philosophy as the tapered standard-length stems.


The epidemiology of THA has shifted dramatically over the past two decades. The procedure is increasingly performed on younger, more active patients who place higher biomechanical demands on their prostheses and who are likely to outlive their index implants. This demographic shift necessitates bone-conserving strategies to facilitate future revision surgeries. Short-stem THA addresses this by preserving metaphyseal and diaphyseal bone stock, optimizing proximal load transfer, and facilitating minimally invasive surgical approaches.



Surgical Anatomy and Biomechanics
Proximal Femoral Osteology and Trabecular Patterns
The success of short-stem THA is entirely predicated on the structural integrity of the proximal femur, specifically the metaphyseal bone. Unlike standard stems that bypass the metaphysis to gain diaphyseal fixation, short stems rely on the compressive trabecular system of the proximal femur. The primary compressive group extends from the medial cortex (calcar femorale) to the superior femoral head, while the primary tensile group arcs from the lateral cortex to the inferior femoral head. The intersection of these trabecular patterns forms the structural basis for metaphyseal fixation.

The calcar femorale, a dense vertical plate of bone originating from the posteromedial aspect of the femoral shaft and radiating proximally toward the greater trochanter, is the primary load-bearing structure for short stems. Preservation of the femoral neck and the calcar is paramount. A high neck osteotomy retains the strong cortical ring of the femoral neck, which provides immediate rotational stability and resists axial subsidence.

Biomechanical Principles of Metaphyseal Fixation
Wolff’s Law dictates that bone remodels in response to the mechanical stresses placed upon it. Standard-length cementless stems, particularly extensively porous-coated cylindrical stems, achieve rigid diaphyseal fixation. This creates a stress-shielding effect in the proximal femur, leading to adaptive bone resorption, calcar round-off, and proximal osteopenia. Over time, this loss of proximal bone stock can complicate revision surgery.


Short stems are designed specifically to mitigate stress shielding. By engaging the metaphyseal bone and terminating proximal to the diaphyseal isthmus, they facilitate more physiological load transfer to the proximal femur. The load is transferred directly to the calcar and the lateral trochanteric flare. Finite element analyses demonstrate that short stems maintain significantly higher periprosthetic bone mineral density in Gruen zones 1 and 7 compared to standard stems.

Indications and Contraindications
The selection of a short stem requires meticulous patient evaluation. Not all femurs are amenable to metaphyseal fixation. The ideal candidate is a younger, active patient with excellent proximal bone stock (Dorr Type A or B femur). The morphology of the proximal femur must allow for adequate cortical contact and compaction of cancellous bone.


Conversely, severe osteoporosis (Dorr Type C femur) is a strict contraindication, as the thinned cortices and sparse trabecular bone cannot provide the necessary initial press-fit stability, leading to a high risk of subsidence and periprosthetic fracture. Proximal femoral deformities, such as severe coxa vara, coxa valga, or prior proximal femoral osteotomies, alter the normal intramedullary geometry and preclude the use of standard short-stem designs.

Patient Selection Criteria
| Clinical Parameter | Short Stem THA Indication | Standard Stem or Alternative |
|---|---|---|
| Bone Quality | Dorr Type A or B (Thick cortices, dense cancellous bone) | Dorr Type C (Osteoporotic, stovepipe canal) |
| Patient Age | Younger, active patients (Typically < 65 years) | Older patients, low demand |
| Femoral Morphology | Normal proximal geometry, intact greater trochanter | Severe dysplasia (Crowe III/IV), prior fracture/osteotomy |
| Diagnosis | Primary Osteoarthritis, Avascular Necrosis (early stage) | Inflammatory arthropathies with severe osteopenia, post-traumatic arthritis with deformity |
| Body Mass Index | Normal to moderately elevated | Morbid obesity (relative contraindication due to high torsional forces) |




Pre Operative Planning and Patient Positioning
Digital Templating and Sizing
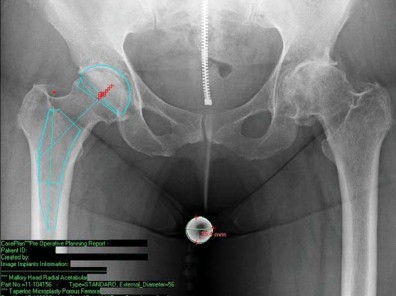
Pre-operative templating is critical in short-stem THA, as the sizing and positioning paradigms differ significantly from standard stems. Standard anteroposterior (AP) pelvis and cross-table lateral radiographs are mandatory. A magnification marker must be used to ensure accurate digital calibration.
When templating a short stem, the surgeon must focus on the metaphyseal fit rather than the diaphyseal fill. The level of the femoral neck osteotomy is the most critical variable. Short stems require a higher neck cut than standard stems to preserve the metaphyseal envelope. The template should demonstrate three-point fixation: medial calcar contact, lateral cortical engagement near the trochanteric flare, and anterior/posterior fill on the lateral radiograph.

Surgeons must also assess the restoration of femoral offset and leg length. Because short stems follow the native curvature of the medial calcar, they naturally recreate the patient's native offset. However, if the neck cut is too low, the stem will subside until it finds cortical engagement, inadvertently shortening the leg and decreasing offset.


Patient Positioning and Surgical Approach Compatibility
Short stems are highly compatible with minimally invasive surgical approaches, particularly the Direct Anterior Approach (DAA) and the minimally invasive anterolateral or posterior approaches. Because the stem is shorter, it requires less soft tissue clearance and less extreme femoral elevation or translation to introduce the broaches and the final implant into the femoral canal.


For the DAA, the patient is positioned supine on a standard or specialized orthopedic traction table. The anterior superior iliac spine (ASIS) and the greater trochanter are palpated and marked. Supine positioning allows for accurate intraoperative assessment of leg length and offset using fluoroscopy, which is particularly beneficial when titrating the fit of a short stem.

Detailed Surgical Approach and Technique
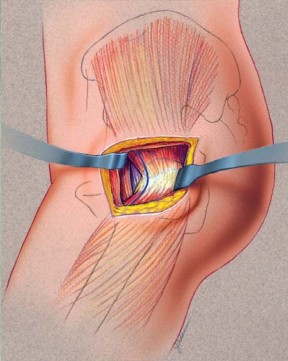
Soft Tissue Dissection and Internervous Planes
The Direct Anterior Approach utilizes the true internervous plane between the tensor fasciae latae (TFL, innervated by the superior gluteal nerve) and the sartorius (innervated by the femoral nerve). An oblique or longitudinal incision is made starting distal and lateral to the ASIS. The fascia over the TFL is incised, and blunt dissection is used to develop the interval.


Ligation of the ascending branches of the lateral femoral circumflex artery is performed to maintain hemostasis. The anterior hip capsule is exposed by elevating the rectus femoris and the iliopsoas. A standard anterior capsulotomy (often an H-type or T-type) is performed, preserving the capsule for later repair.


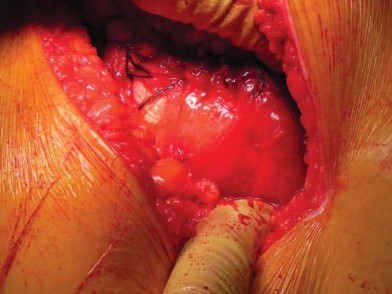
The Femoral Neck Osteotomy
The femoral neck osteotomy is the most critical step in short-stem THA. Unlike standard stems where the cut is often made at the base of the neck, short stems require a conservative, high neck cut. The cut is typically planned based on a measured distance above the lesser trochanter.

Using an oscillating saw, the osteotomy is made perpendicular to the long axis of the femoral neck. Retaining the lateral cortical ring of the neck provides a supportive buttress for the prosthesis, preventing varus collapse and rotational instability. If the cut is inadvertently made too low, the surgeon must be prepared to switch to a standard-length stem, as a short stem will lack the necessary metaphyseal support.

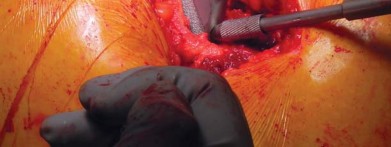
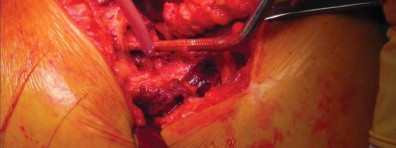
Femoral Preparation and Broaching
Following acetabular preparation and cup insertion, attention is turned to the femur. The femur is elevated and externally rotated. A box osteotome or a curved awl is used to enter the femoral canal, staying lateral to avoid varus positioning.

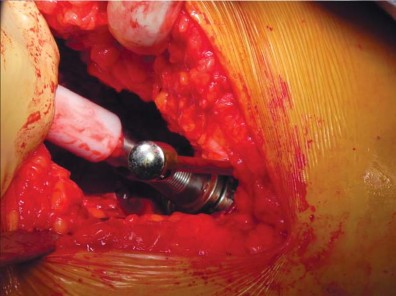
Broaching is performed using progressively larger compaction broaches. The philosophy of compaction broaching is to preserve the cancellous bone by compressing it against the endosteal cortex, creating a dense envelope of bone that enhances initial press-fit stability.



The surgeon must meticulously guide the broach along the medial calcar. Because short stems lack a diaphyseal pilot, there is a tendency for the broach to fall into varus. To counteract this, lateral pressure must be applied during broaching, ensuring the instrument engages the lateral trochanteric bone. The final broach should be rotationally and axially stable.


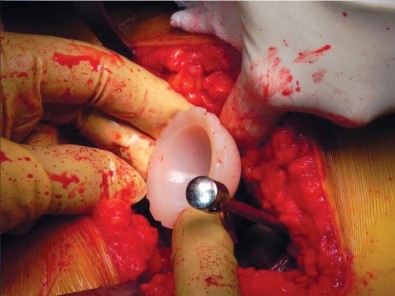
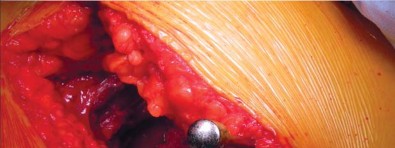
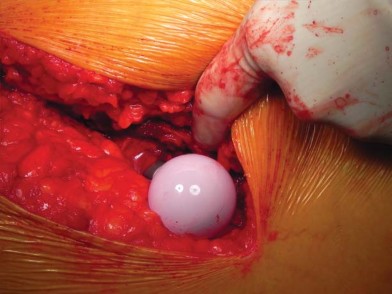
Implant Insertion and Reduction
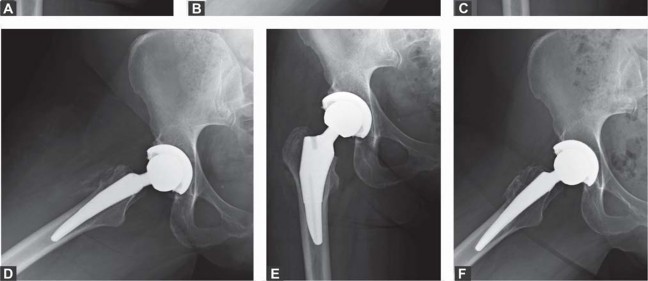
Once the appropriate broach size is determined, the trial neck and head are placed, and the hip is reduced. Leg length, offset, and stability in extremes of motion are assessed. Intraoperative fluoroscopy is highly recommended at this stage to confirm the correct seating and alignment of the trial components.


The trial is removed, and the final short stem is impacted into place. The stem should seat at the exact level of the final broach. Vigorous impaction is not required and can lead to calcar fractures; the stem should achieve a solid "ring" pitch when fully seated. The final head is impacted onto the trunnion, the hip is reduced, and the surgical site is closed in a layered fashion.


Complications and Management
While short-stem THA offers numerous biomechanical advantages, it is not without specific risks. The learning curve associated with metaphyseal preparation and the lack of diaphyseal guidance can lead to unique intraoperative and postoperative complications.

Intraoperative calcar fractures occur when the stem is oversized or when the broach is forced into a mismatched metaphyseal envelope. Varus malalignment is another common issue, occurring when the surgeon fails to lateralize the broach during preparation. While a slight varus position is often well-tolerated with modern tapered wedge short stems, severe varus can lead to early loosening and thigh pain.


Subsidence is defined as the axial migration of the stem within the femoral canal. Because short stems rely on cortical engagement in the metaphysis, a failure to achieve a tight press-fit can result in early subsidence. Most subsidence occurs within the first 6 weeks and stabilizes once secondary osseointegration occurs. However, progressive subsidence >5mm is a harbinger of aseptic loosening.

Summary of Complications and Salvage Strategies
| Complication | Estimated Incidence | Etiology | Management and Salvage Strategy |
|---|---|---|---|
| Intraoperative Calcar Fracture | 1.5% - 3.0% | Oversizing, aggressive impaction, poor bone quality | Prophylactic or therapeutic cerclage wiring. If unstable, bypass with a standard-length diaphyseal fitting stem. |
| Varus Malalignment | 3.0% - 8.0% | Failure to lateralize broach, medial starting point | Often observed if stable. If severe with poor bone contact, revise to standard stem intraoperatively. |
| Early Subsidence (>3mm) | 2.0% - 5.0% | Undersizing, osteoporotic bone, low neck cut | Protected weight-bearing. Serial radiographs. Revise if progressive or symptomatic after 3-6 months. |
| Aseptic Loosening | < 1.0% at 5 years | Failure of osseointegration, thermal necrosis during neck cut | Revision THA using a standard or revision diaphyseal stem. |
| Thigh Pain | < 2.0% | Distal toggle, modulus mismatch | Rule out infection/loosening. Usually resolves spontaneously within 1 year. |


Post Operative Rehabilitation Protocols
The postoperative rehabilitation following short-stem THA aligns with contemporary rapid recovery protocols. Because the procedure is often combined with muscle-sparing approaches and preserves proximal bone, patients typically experience less early postoperative pain and can mobilize rapidly.


You Might Also Like


