Mastering Interposition Arthroplasty for Traumatic Conditions of the Elbow
Key Takeaway
Discover the latest medical recommendations for Mastering Interposition Arthroplasty for Traumatic Conditions of the Elbow. Posttraumatic conditions of the elbow encompass various disorders stemming from prior trauma. These include posttraumatic arthritis, which involves articular surface degeneration; nonunion of the distal humerus; dysfunctional instability due to lost stable function; and chronic ligamentous instability (dislocation). Treatment is tailored to the specific pathology and patient needs.
Introduction and Epidemiology
Posttraumatic conditions of the elbow represent a broad and complex spectrum of disorders involving the ulnohumeral and radiocapitellar joints as a result of previous high-energy trauma or repetitive microtrauma. Treatment for these posttraumatic conditions is highly individualized, depending heavily on the precise characteristics of the pathology, the available bone stock, the integrity of the ligamentous constraints, and most importantly, the functional demands and age of the patient.
Primary pathology typically involves posttraumatic degeneration of the articular surface, leading to severe, recalcitrant posttraumatic arthritis. Secondary pathologies frequently complicate the clinical picture and can include profound soft tissue contracture, intra-articular loose bodies, heterotopic ossification, and impingement or irritation from retained orthopedic hardware.
Nonunion of the distal humerus is a particularly challenging subset of this pathology. It may involve all or a part of the articular surface and is frequently associated with marked fixed angular and rotatory deformity. When nonunion is combined with articular destruction, the reconstructive options become severely limited.

Dysfunctional instability of the elbow represents a special clinical situation where the essential fulcrum for stable elbow function is entirely lost. This is frequently associated with considerable bone loss from the distal humerus, proximal ulna, or both. In severe cases, the forearm may be completely dissociated from the brachium. Chronic ligamentous instability of the elbow can rapidly lead to articular degeneration, particularly in the elderly or osteopenic patient. Fixed contracture and displacement are characteristic of these chronic dislocations.

The epidemiology of posttraumatic elbow arthritis skews younger than primary osteoarthritis or rheumatoid arthritis. Patients are frequently males in their third to fifth decades of life, often employed in heavy manual labor. This demographic presents a unique reconstructive dilemma. Total elbow arthroplasty (TEA) is generally contraindicated in young, high-demand patients due to strict lifetime lifting restrictions (typically limited to 10 to 15 pounds) and a high rate of aseptic loosening and catastrophic mechanical failure. Interposition arthroplasty serves as a critical salvage procedure designed to relieve pain, restore a functional arc of motion, and preserve the patient's ability to perform heavy lifting and high-demand activities.
Surgical Anatomy and Biomechanics
A profound understanding of elbow osseous anatomy and kinematics is a prerequisite for performing interposition arthroplasty. The elbow is a highly constrained hinge joint, relying on both articular congruity and complex ligamentous structures for stability.
Osseous Articulations
The elbow comprises three distinct articulations. The ulnohumeral joint is the primary hinge, providing the majority of structural stability in the sagittal plane. The highly congruent relationship between the trochlear notch of the ulna and the trochlea of the distal humerus acts as the primary constraint to varus and valgus stress, particularly in extension. The radiocapitellar joint allows for forearm rotation while providing a secondary buttress against valgus stress and proximal migration of the radius. The proximal radioulnar joint facilitates pronation and supination.

During interposition arthroplasty, the osseous anatomy is surgically altered to accommodate the interpositional graft. The trochlear notch is frequently widened, and the distal humerus is contoured. This intentional alteration inherently destabilizes the joint, making precise understanding of the ligamentous anatomy critical for subsequent reconstruction.
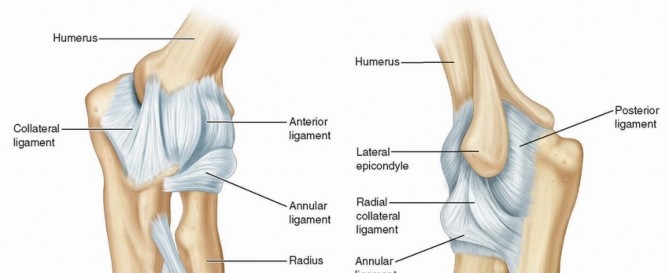
Ligamentous Constraints
The medial collateral ligament (MCL) complex and the lateral collateral ligament (LCL) complex are the primary soft-tissue stabilizers of the elbow.
The anterior bundle of the MCL is the primary restraint to valgus stress. It originates from the anteroinferior surface of the medial epicondyle and inserts on the sublime tubercle of the coronoid process.
The lateral ulnar collateral ligament (LUCL) is the primary restraint to posterolateral rotatory instability. It originates from the lateral epicondyle, blends with the annular ligament, and inserts on the supinator crest of the ulna.
Because interposition arthroplasty often requires extensive bony resection that compromises the epicondylar origins of these ligaments, concurrent reconstruction of the collateral ligaments is frequently mandated to restore the functional fulcrum of the elbow.
Kinematics and Axis of Rotation
The functional axis of rotation of the elbow passes through the center of the capitellum laterally and the anteroinferior aspect of the medial epicondyle medially. Identifying this precise isometric axis is critical during the application of a dynamic hinged external fixator, which is a mandatory adjunct in modern interposition arthroplasty techniques. Misalignment of the external fixator axis by even a few millimeters can lead to eccentric loading of the interpositional graft, rapid graft failure, and recurrent instability.
Indications and Contraindications
Interposition arthroplasty is a technically demanding salvage procedure with a narrow but critical set of indications. Patient selection is paramount for achieving a successful outcome. The ideal candidate is a young, active, high-demand patient with severe posttraumatic arthritis who is willing to accept a potentially lengthy rehabilitation process and understands that the procedure may eventually fail, requiring conversion to a total elbow arthroplasty later in life.

| Parameter | Operative Indications for Interposition Arthroplasty | Non-Operative Management or Alternative Procedures |
|---|---|---|
| Patient Age | Young to middle-aged (< 60 years) | Elderly (> 65 years) - Consider Total Elbow Arthroplasty |
| Functional Demand | High demand, heavy manual labor, lifting requirements > 15 lbs | Low demand, sedentary lifestyle |
| Pathology | Severe posttraumatic arthritis, articular destruction | Mild to moderate arthritis - Consider arthroscopic debridement |
| Bone Stock | Intact medial and lateral columns, reconstructable epicondyles | Severe bone loss, missing columns - Contraindication |
| Infection Status | Aseptic joint | Active or recent intra-articular infection - Absolute Contraindication |
| Neurologic Status | Intact motor control (biceps, brachialis, triceps) | Profound neuromuscular dysfunction, flail extremity |

Absolute contraindications include active joint infection, inadequate bone stock to support the collateral ligaments (loss of the medial and lateral columns), and an inability or unwillingness to comply with strict postoperative rehabilitation protocols. Relative contraindications include profound preoperative stiffness that cannot be released, and severe chronic regional pain syndrome.
Pre Operative Planning and Patient Positioning
Patient History
The patient history is directed at gaining information about the initial injury, treatments undertaken, complications of treatment, presenting complaints, and patient expectations. Detailed investigation of the patient's symptoms should include questions regarding the degree of pain, presence of instability or stiffness, and mechanical symptoms of catching or locking.
Presence of radiating pain, especially in the ulnar nerve distribution, is solicited. Special attention is paid to night pain and pain at rest, as these suggest a possibility of sepsis. A history of drainage or any evidence of infection is especially critical to elicit, as latent infection is a primary cause of catastrophic failure in reconstructive elbow surgery.
Physical Examination
Physical examination of the elbow should follow a systematic approach. Inspection of the elbow is performed, looking especially for warmth and redness, and noting the presence and location of previous skin incisions or persistent wounds. The alignment of the extremity at rest is evaluated, and the physician must palpate for prominent hardware.
Localization of pain during active and passive motion is essential. Active range of motion (AROM) is assessed and compared to the opposite side. The degree of motion, smoothness of motion, and feel of the end point is established. Normal AROM varies but should be symmetric with the opposite unaffected side. Range of motion should be from near full extension (may have hyperextension) to 130 to 140 degrees of flexion. Normal forearm rotation is an arc of 170 degrees, with slightly more supination than pronation. Functional range of motion has been defined as a flexion-extension arc from 30 to 130 degrees and a pronation-supination arc from 50 degrees of pronation to 50 degrees of supination.
Passive range of motion (PROM) is then assessed and compared to the active motion arc to differentiate between capsular contracture and muscle weakness or guarding. Palpation of the elbow should systematically review all of the bony and soft tissue structures of the elbow.
The ulnar nerve needs to be carefully assessed. If previously surgically manipulated, its location should be identified if possible. Examine for the presence of a Tinel sign at the cubital tunnel and along the course of transposition. Motor function of the elbow should be rigorously assessed. In particular, the flexor (biceps and brachialis) and extensor (triceps) mechanisms must be evaluated for strength and continuity, as active dynamic stabilization is required postoperatively.
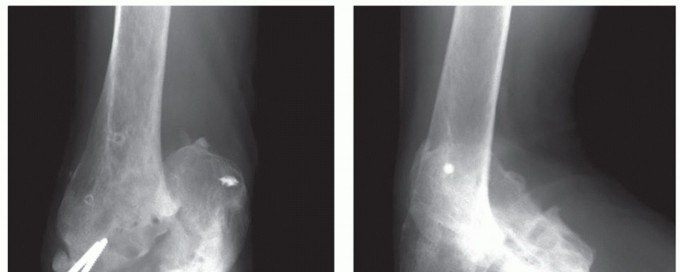
Imaging and Templating
Standard anteroposterior, lateral, and oblique radiographs of the elbow are obtained to assess joint space narrowing, osteophyte formation, heterotopic ossification, and the status of retained hardware.

Computed tomography (CT) with three-dimensional reconstructions is highly recommended. CT imaging provides critical detail regarding the precise location and volume of bone loss, the integrity of the medial and lateral columns, and the architecture of the greater sigmoid notch. This allows the surgeon to plan the degree of bony resection required to accommodate the interpositional graft.
Patient Positioning
The patient is typically placed in the lateral decubitus position or supine with the arm draped across the chest. The lateral decubitus position with the arm resting over a padded bolster allows for excellent visualization of the posterior compartment and facilitates the application of the hinged external fixator. A sterile tourniquet is applied high on the brachium to ensure a bloodless field during the initial dissection and bony preparation.

Detailed Surgical Approach and Technique
Surgical Exposure and Nerve Management
A universal posterior midline incision is utilized, typically incorporating or excising previous surgical scars. Full-thickness fasciocutaneous flaps are elevated medially and laterally. The first critical step is the identification, neurolysis, and protection of the ulnar nerve. The nerve is decompressed from the arcade of Struthers proximally to the deep flexor pronator aponeurosis distally. In the setting of extensive posttraumatic scarring, the nerve may be encased in dense fibrosis. An anterior subcutaneous transposition is routinely performed to protect the nerve during the extensive bony work and application of the external fixator.
Deep Dissection and Joint Preparation
Exposure of the ulnohumeral joint can be achieved via a triceps-reflecting approach (Bryan-Morrey), a triceps-splitting approach, or an olecranon osteotomy, depending on the need for articular exposure and the presence of preexisting hardware. The triceps-reflecting approach is generally preferred as it preserves the extensor mechanism continuity while allowing wide exposure of the distal humerus.

Once the joint is exposed, a thorough capsulectomy is performed. All heterotopic bone, loose bodies, and impinging osteophytes are excised. The articular surfaces of the distal humerus and proximal ulna are meticulously debrided. The goal is to create a congruent, smooth articulation that can accommodate the volume of the interpositional graft without overstuffing the joint.
The distal humerus is contoured using a high-speed burr to recreate the trochlear sulcus and capitellar convexity. The greater sigmoid notch of the ulna is deepened and widened. If the radial head is severely arthritic or blocks motion, a radial head excision or replacement may be performed concomitantly.

Graft Preparation and Interposition
The ideal interpositional material remains a subject of academic debate, but Achilles tendon allograft and autologous fascia lata are the most commonly utilized. Achilles tendon allograft provides robust, thick tissue that can withstand the significant compressive and shear forces of the ulnohumeral joint.

The graft is tailored to fit the contoured distal humerus. It is draped over the articular surface of the distal humerus, covering the trochlea and capitellum. The graft is secured using multiple suture anchors or transosseous drill holes placed along the anterior and posterior aspects of the distal humerus, ensuring the graft is tensioned smoothly over the articular surface without redundant folds that could cause mechanical catching.
Ligamentous Reconstruction
Because the radical debridement and bony contouring frequently compromise the origins of the MCL and LUCL, ligamentous reconstruction is often required to restore varus and valgus stability. If an Achilles tendon allograft with an attached calcaneal bone block is used, the tendinous portion can be split to reconstruct the collateral ligaments, while the central portion covers the articular surface. Alternatively, separate palmaris longus or plantaris autografts can be routed through isometric drill holes in the epicondyles and the proximal ulna/radius to reconstruct the MCL and LUCL.

Application of the Hinged External Fixator
The application of a dynamic hinged external fixator is arguably the most critical step in preventing early failure of the interposition arthroplasty. The fixator unloads the healing graft, maintains joint distraction, and provides strict sagittal plane stability while allowing early active range of motion.

A precise isometric axis must be established. A 2.0 mm Kirschner wire is driven from the center of the capitellum laterally to the anteroinferior medial epicondyle medially. The fixator hinge is centralized over this axis pin. Half-pins are then placed into the humeral diaphysis and the ulnar diaphysis. The fixator is locked, and the axis pin is removed. The joint is taken through a full range of motion to ensure concentric reduction throughout the arc without hinge binding or joint subluxation.
Complications and Management
Interposition arthroplasty is fraught with potential complications, given the severity of the underlying pathology and the technical complexity of the procedure. Meticulous surgical technique and rigorous postoperative management are required to mitigate these risks.
| Complication | Estimated Incidence | Etiology and Pathogenesis | Salvage and Management Strategies |
|---|---|---|---|
| Recurrent Instability | 10% - 25% | Failure to reconstruct collateral ligaments, malposition of external fixator axis, severe bone loss. | Revision ligamentous reconstruction, prolonged external fixation, eventual conversion to TEA. |
| Graft Resorption and Narrowing | 15% - 30% | Natural biologic degradation of allograft, excessive compressive loading. | Often tolerated if functional motion remains. Revision interposition or TEA if pain becomes debilitating. |
| Ulnar Neuropathy | 5% - 15% | Traction injury during exposure, compression from scar tissue, inadequate transposition. | Revision neurolysis, ensuring submuscular or secure subcutaneous transposition. |
| Deep Infection | 3% - 8% | Prolonged operative time, extensive dead space, external fixator pin tract infections tracking intra-articularly. | Aggressive surgical debridement, removal of graft/hardware, placement of antibiotic spacer, eventual TEA or arthrodesis. |
| Recurrent Stiffness | 20% - 40% | Inadequate postoperative rehabilitation, heterotopic ossification, capsular fibrosis. | Aggressive physical therapy, dynamic splinting, secondary arthroscopic or open contracture release. |

Pin tract infections from the external fixator are the most common minor complication and are generally managed successfully with local pin care and short courses of oral antibiotics. However, if a pin tract infection tracks into the joint, it becomes a limb-threatening emergency requiring immediate fixator removal and joint lavage.
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is as critical to the success of the procedure as the surgical execution. The rehabilitation is divided into distinct phases, heavily reliant on the presence of the hinged external fixator.
Clinical & Radiographic Imaging
You Might Also Like