Mastering TFCC Dorsal Ligament Reconstruction and Ulnar Impaction Management
Key Takeaway
The Scheker technique for dorsal ligament reconstruction of the triangular fibrocartilage complex (TFCC) restores distal radioulnar joint stability using a tendon graft. This comprehensive surgical guide details the biomechanics of ulnar impaction, precise osseous tunnel preparation in the radius and ulna, graft routing, and tensioning protocols. Indicated for chronic DRUJ instability, this procedure mitigates ulnocarpal abutment and prevents progressive arthritic degeneration when conservative management fails.
INTRODUCTION TO DISTAL RADIOULNAR JOINT INSTABILITY
The distal radioulnar joint (DRUJ) is a complex diarthrodial articulation that, in conjunction with the proximal radioulnar joint, facilitates forearm rotation. Stability of the DRUJ is primarily conferred by the triangular fibrocartilage complex (TFCC), specifically its dorsal and palmar radioulnar ligaments. Chronic instability of the DRUJ, often resulting from irreparable TFCC tears or severe distal radius malunions, leads to debilitating wrist pain, weakness, and progressive arthrosis.
When direct anatomic repair of the TFCC is not feasible due to tissue attrition or chronicity, ligamentous reconstruction becomes necessary. The Scheker technique for the reconstruction of the dorsal ligament of the TFCC provides a robust, biomechanically sound method to restore DRUJ kinematics using an autogenous tendon graft (typically the palmaris longus).
💡 Clinical Pearl: The Biomechanics of DRUJ Stability
The dorsal radioulnar ligament tightens during forearm pronation, while the palmar radioulnar ligament tightens during supination. Recognizing these dynamic tensioning patterns is critical for both accurate clinical diagnosis of instability and correct intraoperative tensioning of the reconstructed graft.
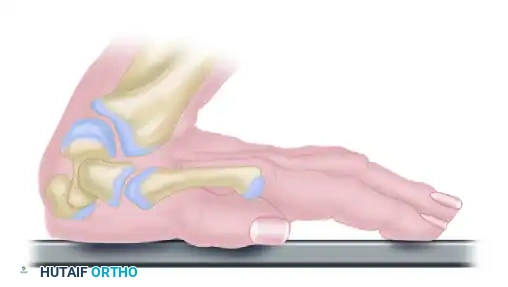
PATHOMECHANICS: ULNAR IMPACTION-ABUTMENT SYNDROME
Symptoms of ulnar-sided wrist pain aggravated by ulnar deviation and forearm rotation are frequently attributable to ulnocarpal impaction (abutment). This condition arises from excessive load transmission across the ulnar aspect of the wrist, leading to progressive degenerative changes.
Biomechanical Considerations of Ulnar Variance
In a normal wrist with neutral ulnar variance, approximately 80% of the axial load is transmitted through the radiocarpal joint, and 20% through the ulnocarpal joint. Alterations in ulnar variance drastically shift this load distribution:
* Positive Ulnar Variance (+2.5 mm): Increases ulnocarpal load transmission by 42%.
* Dorsal Tilt of the Distal Radius (45 degrees): Increases ulnocarpal load transmission by 65%.
Patients with acquired or developmental ulnar-positive variance are at high risk for developing degenerative tears of the TFCC, chondromalacia of the ulnar head, articular wear on the proximal poles of the lunate and triquetrum, and attenuation or rupture of the lunotriquetral (LT) interosseous ligament.
Etiology of Ulnar-Positive Variance
Positive ulnar variance may be a normal anatomical variant or secondary to:
* Developmental Abnormalities: Madelung deformity.
* Traumatic Acquired Variance: Shortening of the radius following a distal radius fracture (e.g., malunited Colles fracture).
* Longitudinal Instability: Radial head fracture-dislocation combined with interosseous membrane injury (Essex-Lopresti lesion).
* Pediatric Trauma: Premature physeal closure/growth arrest of the distal radius.
Differential Diagnosis: Ulnocarpal vs. Ulnostyloid Abutment
Accurate differentiation between ulnocarpal and ulnostyloid abutment dictates the surgical approach.
* Ulnocarpal Abutment: Patients experience exacerbation of pain with ulnar deviation combined with forearm pronation or in a neutral position.
* Ulnostyloid Abutment: Patients experience pain with ulnar deviation combined with forearm supination. An old, ununited ulnar styloid fracture is a frequent culprit.
⚠️ Surgical Warning: Diagnostic Pitfall
Routine, neutral-rotation radiographs may falsely demonstrate neutral ulnar variance. Dynamic changes contribute significantly to symptoms. A pronated grip view radiograph is mandatory; it often reveals an average increased ulnar-positive variance of 2.5 mm compared to resting films, unmasking dynamic ulnocarpal impaction.
PREOPERATIVE EVALUATION AND IMAGING
Physical examination should include assessment of DRUJ stability (ballottement test) in neutral, full pronation, and full supination. Ulnocarpal pain is typically aggravated by passive ulnar deviation (ulnocarpal stress test). Furthermore, passive dorsal translation of the ulnar side of the carpus—performed by pushing dorsally against the palmar surface of the pisiform while stabilizing the distal ulna—often reproduces the patient's mechanical pain.
Radiographic Findings:
* Ulnar-positive variance (static or dynamic on pronated grip views).
* Subchondral cystic changes or sclerosis in the proximal ulnar aspect of the lunate and the radial aspect of the ulnar head.
* DRUJ osteoarthritis, characterized by joint space narrowing, subchondral sclerosis, and marginal osteophyte formation.
SURGICAL TECHNIQUE: RECONSTRUCTION OF THE DORSAL LIGAMENT OF THE TFCC (SCHEKER ET AL.)
1. Patient Positioning and Preparation
- Place the patient supine with the operative arm extended on a radiolucent hand table.
- Apply a proximal pneumatic tourniquet. Exsanguinate the limb and inflate the tourniquet to the standard upper extremity pressure (typically 250 mm Hg).
- Position the forearm in pronation to begin the dorsal exposure.
2. Incision and Deep Exposure
- Make an angled dorsal incision in the skin overlying the junction between the fourth (extensor digitorum communis) and fifth (extensor digiti minimi) extensor compartments.
- Carefully dissect through the subcutaneous tissues, protecting the dorsal sensory branches of the ulnar nerve (DSBUN).
- Open the deep antebrachial fascia between the extensor digitorum and the extensor carpi radialis brevis (ECRB) tendons, remaining proximal to the extensor retinaculum.
- Retract the musculotendinous units to expose the dorsoulnar aspect of the distal radius, just distal to the extensor pollicis brevis muscle belly.
3. Radial Capsulotomy
- Perform a precise, small capsulotomy between the fourth and fifth extensor compartments.
- Elevate the capsule to expose the dorsal corner of the sigmoid notch of the distal radius.
4. Preparation of the Radial Osseous Tunnels
- Tunnel 1 (a-a1): Using a heavy Kirschner wire (K-wire), drill a tunnel in the distal radius. Start precisely at the dorsal lip of the sigmoid notch. Direct the wire in a proximal, radial, and palmar direction into the medullary cavity.
- Tunnel 2 (b-a1): Create a second tunnel in the radial metaphysis. Start approximately 3 cm proximal and radial to the lip of the sigmoid notch. Direct the K-wire in a distal, radial, and palmar direction to intersect the first tunnel within the medullary cavity.
- Enlargement: This creates a V-shaped, angulated tunnel in the distal radius. Enlarge this continuous tunnel using a hand drill equipped with a 3.0-mm drill bit.
- Tunnels 3 & 4 (c & d): Drill two additional unicortical holes, measuring 3.0 to 3.5 mm in diameter, into the radial metaphysis. Space these holes at 1-cm intervals proximal to the initial construct.
- Connect these two proximal holes (c and d) within the medullary canal using a large tendon hook or curved curette. Smooth all bony edges to prevent graft abrasion during passage.
5. Preparation of the Ulnar Osseous Tunnels
- Shift the focus to the distal ulna. Approach the radial aspect of the distal ulna through the interval between the fifth and sixth (extensor carpi ulnaris - ECU) compartment muscles. Retract the soft tissues carefully.
- Open the DRUJ capsule at the level of the ulnar styloid, remaining just radial to the ECU tendon sheath.
- Tunnel 5 (e-f): Use a heavy K-wire to drill a tunnel starting from the ulnar fovea (the anatomic isometric origin of the TFCC). Direct the wire through the medulla to exit on the dorsoradial side of the ulnar cortex. Enlarge this tunnel with a 3.0-mm drill bit.
- Tunnels 6 & 7 (g & h): Drill two more holes, spaced 1 cm apart, along the distal ulnar diaphysis/metaphysis. Connect these holes to form a continuous tunnel within the ulnar medullary canal.
6. Graft Harvest and Passage
Harvest a palmaris longus tendon graft (or alternative, such as a strip of flexor carpi radialis or allograft, if the palmaris is absent) using standard minimally invasive tendon stripping techniques.
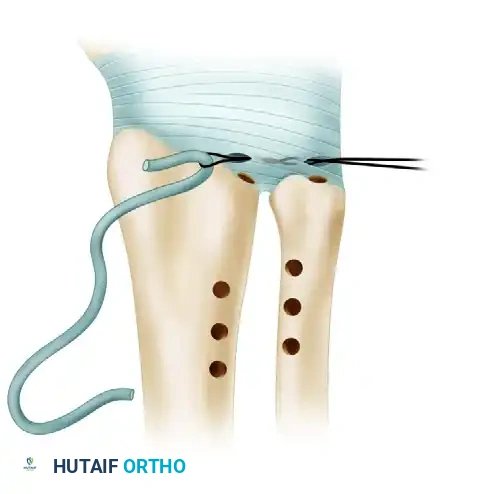
- Initial Passage: Use small, angulated mosquito forceps to pass a loop of 26-gauge wire (or a suture shuttle) into the radial capsulotomy, across the DRUJ, and out through the ulnar capsulotomy. Draw the tendon graft through the joint space using this wire loop.
Figure A: The tendon graft is drawn through the radial and ulnar capsulotomies, traversing the DRUJ.
- Routing the Ends: Using the wire loop technique, pull the radial end of the tendon graft into hole a (at the sigmoid notch) and out of hole b (proximal radius). Simultaneously, pull the ulnar end of the tendon graft into hole e (fovea) and out of hole f (dorsoradial ulna).
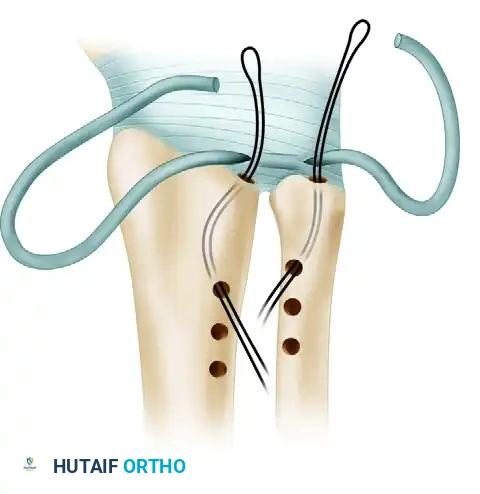
Figure B: The ends of the tendon graft are inserted into loops of wire emerging from the tunnels in the ulnar fovea and the dorsal lip of the sigmoid notch of the radius.
- Distal Ulnar Routing: Route the ulnar end of the tendon into the medulla of the ulna through hole g and out through hole h.

Figure C: The tendon graft is drawn through the two distal tunnels in the ulnar metaphysis.
7. Fixation and Tensioning
- Ulnar Fixation First: Suture the ulnar end of the tendon to itself using a heavy, non-absorbable 3-0 braided suture (e.g., Ticron or Ethibond).
- Crucial Step: The ulnar side must be attached first. When the hand is subsequently supinated to tension the graft, the ulnar tunnel rotates toward the volar aspect and disappears from the dorsal surgical field.
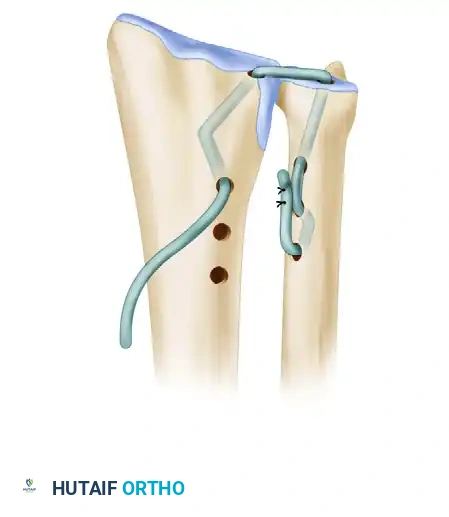
Figure D: The ulnar end of the tendon graft is threaded through the second tunnel and securely sutured to itself.
- Proximal Radial Routing: Using a similar wire-loop technique, pull the radial end of the tendon graft into hole c and out of hole d.

Figure E: The tendon graft is pulled between the middle and distal holes in the metaphysis of the radius to ensure that full tension can be applied between the fovea and the sigmoid notch.
- Tensioning: Place the forearm in full supination. Apply firm tension to the radial end of the tendon graft. While maintaining tension, assess the stability of the DRUJ by translating the ulna dorsally and volarly in both pronation and supination.
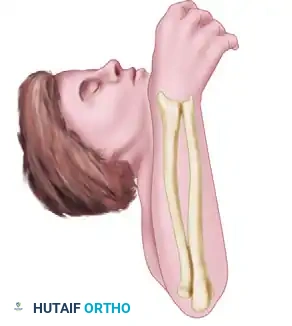
Figure F: With tension applied to the radial end of the tendon graft while the forearm is supinated, joint stability is rigorously tested through a full range of motion.
- Final Radial Fixation: Once optimal stability is confirmed without over-constraining the joint, tighten the radial end of the tendon while the forearm remains in supination, and suture the graft to itself using 3-0 non-absorbable suture.
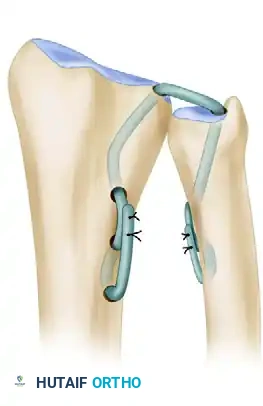
Figure G: On the radial side, the graft is sutured to itself with the forearm held in supination, completing the robust reconstruction of the dorsal ligament.
- Closure: Thoroughly irrigate the wound. Close the extensor retinaculum, subcutaneous tissue, and skin. Maintain the forearm in supination during wound closure to protect the newly tensioned dorsal ligament reconstruction.
POSTOPERATIVE CARE AND REHABILITATION
Strict adherence to the postoperative immobilization protocol is paramount to allow for biologic incorporation of the tendon graft within the osseous tunnels.
- Phase I (0 to 3 Weeks): The forearm is immobilized in a long-arm cast with the forearm in neutral rotation. This protects the graft from extreme tension while initial healing occurs.
- Phase II (3 to 6 Weeks): At 3 weeks, the initial cast and sutures are removed. A new long-arm cast (or rigid Munster-style orthosis) is applied with the forearm positioned in 20 to 30 degrees of pronation for an additional 3 weeks.
- Rationale: Immobilizing in slight pronation removes tension from the reconstructed dorsal ligament, preventing elongation of the healing graft.
- Phase III (6 to 10 Weeks): Immobilization is discontinued. The patient begins a supervised physical therapy program focusing on active range-of-motion (AROM) exercises for wrist flexion/extension and forearm pronation/supination. Lifting and forceful gripping are strictly prohibited.
- Phase IV (10+ Weeks): Passive range-of-motion (PROM) and progressive strengthening exercises are initiated. Full return to heavy manual labor or sports is typically delayed until 4 to 6 months postoperatively, contingent upon the restoration of dynamic stability and strength.
MANAGEMENT OF COEXISTING ULNAR IMPACTION AND DRUJ ARTHRITIS
Reconstruction of the TFCC addresses instability but does not reverse established osseous abutment or advanced osteoarthritis. Operative treatment for these conditions is indicated when conservative measures (activity modification, splinting, NSAIDs, corticosteroid injections) fail.
Surgical Options for Ulnocarpal Impaction
If DRUJ arthritis is absent, the goal is to decompress the ulnocarpal joint:
* Arthroscopic TFCC Debridement: Sufficient for patients with ulnar-neutral to slightly positive variance with central TFCC tears. However, pain will persist if significant ulnar-positive variance is left unaddressed.
* Ulnar Wafer Resection (Open or Arthroscopic): Involves resecting the distal 2-3 mm of the ulnar head (leaving the styloid and TFCC attachments intact). Ideal for mild positive variance (1-2 mm).
* Ulnar Shortening Osteotomy (USO): The gold standard for significant ulnar-positive variance, especially following radial shortening fractures. USO unloads the ulnocarpal joint and simultaneously tightens the ulnocarpal ligaments and TFCC, enhancing DRUJ stability. Modern dynamic compression plating techniques yield exceptionally high union rates.
Surgical Options for Ulnostyloid Impaction
- Styloidectomy: Excision of the ununited or hypertrophic ulnar styloid fragment. Care must be taken to preserve the foveal attachments of the TFCC to prevent iatrogenic DRUJ instability.
Surgical Options for Advanced DRUJ Arthritis
Arthritic changes in the DRUJ may result from primary osteoarthritis, post-traumatic incongruity, or inflammatory arthropathies (e.g., rheumatoid arthritis). When joint preservation is no longer viable, salvage procedures include:
* Excisional Arthroplasty (Darrach Procedure): Resection of the distal ulna. Generally reserved for low-demand or elderly rheumatoid patients due to the risk of painful ulnar stump instability.
* Modified Arthrodesis (Sauvé-Kapandji Procedure): Fusion of the DRUJ combined with a proximal pseudoarthrosis of the ulna to maintain forearm rotation. Excellent for high-demand patients with DRUJ arthritis.
* Implant Arthroplasty: Partial or total DRUJ replacement using constrained or semi-constrained prostheses.
* Salvage of the Failed Resection: For a painful, unstable distal ulnar stump following a Darrach procedure, options include soft-tissue tethering (e.g., tenodesis), extensive ulnar resection, or creation of a "one-bone" forearm (radioulnar fusion), which completely sacrifices forearm rotation for pain relief and stability.
===
You Might Also Like