Open Repair of Class 1D TFCC Injuries: Comprehensive Surgical Guide
Key Takeaway
Class 1D triangular fibrocartilage complex (TFCC) injuries involve a traumatic avulsion of the articular disc from its radial attachment at the sigmoid notch. Open repair, utilizing the Cooney technique, restores distal radioulnar joint (DRUJ) stability through direct transosseous suture fixation. This guide details the step-by-step surgical approach, biomechanical principles, and postoperative rehabilitation protocols essential for achieving optimal functional outcomes in complex radioulnar instability.
INTRODUCTION TO CLASS 1D TFCC INJURIES
The triangular fibrocartilage complex (TFCC) is the primary stabilizing structure of the distal radioulnar joint (DRUJ) and the ulnocarpal articulation. According to the Palmer classification of TFCC lesions, Class 1 injuries are traumatic in etiology. Specifically, a Class 1D injury denotes a traumatic avulsion of the TFCC from its radial attachment at the distal margin of the sigmoid notch.
Unlike the more common Class 1B (ulnar avulsion) injuries, Class 1D lesions disrupt the critical tension-band mechanism of the radioulnar ligaments at their radial footprint. This results in profound DRUJ instability, altered load transmission across the ulnocarpal joint, and significant ulnar-sided wrist pain. While arthroscopic techniques have advanced, open repair remains the gold standard for massive, retracted Class 1D tears, particularly when associated with complex distal radius fractures or chronic DRUJ instability.
This comprehensive guide details the open repair technique pioneered by Cooney et al., providing orthopedic surgeons with an evidence-based, step-by-step approach to restoring radioulnar kinematics.
SURGICAL ANATOMY AND BIOMECHANICS
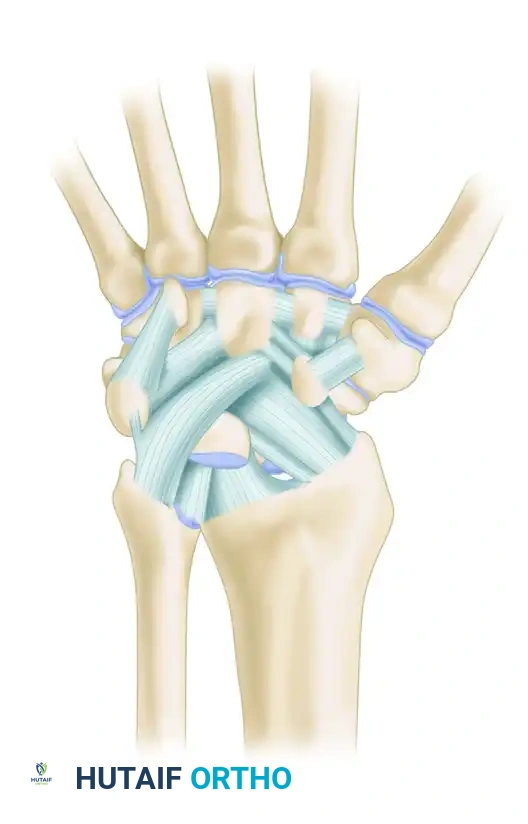
A profound understanding of DRUJ kinematics is requisite for successful surgical intervention. The TFCC is a complex, three-dimensional structure comprising the articular disc, the dorsal and palmar radioulnar ligaments, the meniscus homologue, the ulnocarpal ligaments (ulnolunate and ulnotriquetral), and the extensor carpi ulnaris (ECU) subsheath.
The Sigmoid Notch and Radioulnar Ligaments
The radial attachment of the TFCC spans the distal margin of the sigmoid notch. The dorsal and palmar radioulnar ligaments are the primary stabilizers of the DRUJ. During forearm rotation, these ligaments experience reciprocal tension:
* Pronation: The dorsal radioulnar ligament tightens, preventing dorsal subluxation of the ulna.
* Supination: The palmar radioulnar ligament tightens, preventing palmar subluxation of the ulna.
💡 Clinical Pearl: Biomechanical Implications of Class 1D Tears
A Class 1D avulsion detaches both the dorsal and palmar radioulnar ligaments from the radius. This global detachment destabilizes the DRUJ in both pronation and supination, necessitating a robust transosseous repair to restore the anatomical footprint and withstand the rotational torque of the forearm.
INDICATIONS AND PREOPERATIVE PLANNING
Indications for Open Repair
- Acute, traumatic Class 1D TFCC tears with gross clinical DRUJ instability.
- Failure of conservative management (immobilization) after 4 to 6 weeks.
- Concomitant displaced distal radius fractures requiring open reduction and internal fixation (ORIF), where the TFCC radial footprint is avulsed.
- Chronic DRUJ instability secondary to an unrecognized Class 1D lesion.
Preoperative Evaluation
Standard posteroanterior (PA), lateral, and oblique radiographs of the wrist are mandatory. The PA view must be evaluated for ulnar variance, as ulnar-positive variance significantly increases load transmission across the TFCC and may necessitate a concomitant ulnar shortening osteotomy.
Magnetic Resonance Imaging (MRI) or MR Arthrography is the imaging modality of choice to confirm the diagnosis, assess the integrity of the ECU subsheath, and evaluate the articular cartilage of the lunate and ulnar head.
PATIENT POSITIONING AND PREPARATION
- Anesthesia: The procedure is performed under regional anesthesia (brachial plexus block) or general anesthesia, depending on patient factors and anticipated surgical duration.
- Positioning: Place the patient in the supine position. Extend the affected extremity onto a radiolucent hand table.
- Tourniquet: Apply a well-padded pneumatic tourniquet to the proximal upper arm.
- Preparation: Following standard sterile skin preparation and draping, exsanguinate the limb using an Esmarch bandage and inflate the tourniquet to the appropriate pressure (typically 250 mm Hg or 100 mm Hg above systolic blood pressure).
SURGICAL TECHNIQUE: THE COONEY ET AL. APPROACH
The open repair of a Class 1D injury requires meticulous dissection to expose the DRUJ without compromising the overlying extensor compartments.
1. Incision and Superficial Dissection
- Make a straight, dorsoulnar skin incision centered over the DRUJ, coursing between the fourth (extensor digitorum communis) and fifth (extensor digiti minimi) extensor compartments.
- The incision should be sufficiently long—usually 8 to 10 cm—to gain unhindered access to both the DRUJ and the ulnocarpal joint.
- Carefully dissect through the subcutaneous tissues, identifying and protecting the dorsal sensory branches of the ulnar nerve (DSBUN).
2. Extensor Retinaculum Flap Creation
- Identify the extensor retinaculum. Open the retinaculum in a Z-shaped configuration.
- This specific geometry is critical; it preserves robust retinacular flaps that will be utilized later for either retinacular repair or augmentation of the TFCC reconstruction.
- Identify the extensor carpi ulnaris (ECU) tendon within the sixth compartment and retract it laterally (radially) to expose the underlying joint capsule.
3. Capsulotomy and Joint Exposure
- Perform a longitudinal incision through the radioulnar joint capsule. Begin proximal to the DRUJ and extend distally toward the dorsal radioulnar ligament.
- Turn the incision medially (ulnarward) along the proximal edge of the dorsal radioulnar ligament to create an L-shaped capsular flap.
- Beginning just distal to the dorsal radioulnar ligament, extend the capsular incision transversely. This maneuver exposes the ulnocarpal joint, the lunate fossa, the lunate, the triquetrum, the ulnar lunotriquetral ligament complex, and the TFCC itself.
4. Assessment and Preparation of the Radial Footprint
- Utilize small periosteal elevators and arthroscopic probes to meticulously determine the extent of the TFCC damage and confirm the Class 1D avulsion.
- Detach the dorsal radioulnar ligament from the dorsal surface of the distal radius to facilitate visualization.
- Reflect the periosteum from the distal radius, just proximal to the lunate fossa, to expose the dorsoulnar cortex of the distal radius.
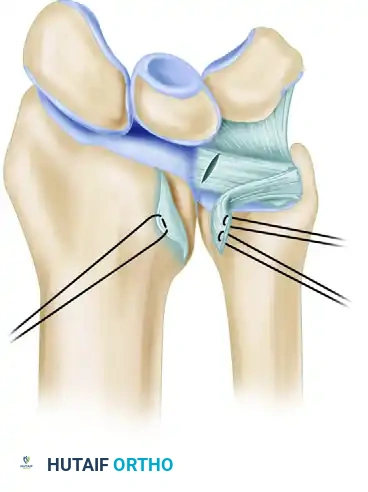
Figure A: Approach to the TFCC, demonstrating the reflection of the dorsal radioulnar ligament and periosteum over the lunate fossa to expose the radial footprint.
- Inspect the triangular fibrocartilage and the radiocarpal joint for any concomitant chondral injuries or loose bodies.
- Using a rongeur or a powered burr, aggressively débride the distal margin of the sigmoid notch and the torn margin of the TFCC down to bleeding subchondral bone. This decortication is vital to stimulate a robust healing response.
⚠️ Surgical Warning: Ulnar-Positive Variance
Insert a small lamina spreader between the radius and ulna to improve exposure of the sigmoid notch. If satisfactory exposure cannot be achieved, or if the patient exhibits a significant ulnar-positive variance, Cooney et al. strongly recommend performing a concomitant ulnar shortening osteotomy with rigid plate fixation. Failure to address ulnar positivity will result in excessive compressive forces on the repair, leading to inevitable failure.
5. Transosseous Drill Holes and Suture Passage
- Utilize a 1.2-mm Kirschner wire (or a drill bit of equivalent size) to create a line of four side-by-side drill holes through the distal radius.
- The trajectory of these holes must be precise: drill from the dorsal surface of the distal radius (dorsoradial) directing the wire palmar-ulnar, ensuring the drill point exits exactly at the distal margin of the sigmoid notch, at the ulnar (medial) border of the lunate fossa.
- Select a high-tensile, absorbable suture—typically 2-0 or 3-0 polyglactin 910 (Vicryl) or polydioxanone (PDS)—armed with a small, round needle.
- Place horizontal mattress sutures into the substance of the avulsed TFCC. Pass the suture from the proximal undersurface to the distal surface of the fibrocartilage to ensure a secure bite.
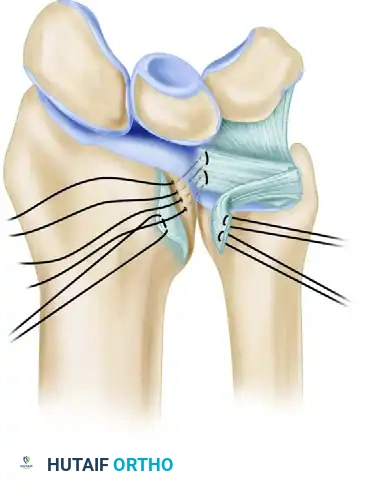
Figure B: Suture placement into the TFCC through holes drilled in the dorsoulnar aspect of the distal radius. Horizontal mattress sutures are directed in a palmar and ulnar direction to exit at the edge of the lunate fossa and sigmoid notch.
- Remove the small needles from the sutures.
- To retrieve the sutures through the transosseous tunnels, pass a straight needle (without suture) in reverse through the drill holes to capture and pull the ends of the suture pairs dorsally. Alternatively, a wire loop (Hewson suture passer) or a specialized nitinol suture passer can be utilized with excellent efficacy.
6. DRUJ Reduction and Fixation
- Flex the patient's elbow to 90 degrees and position the forearm in neutral to slight supination. This position anatomically reduces the DRUJ and relaxes the dorsal radioulnar ligament.
- While maintaining this reduction, stabilize the DRUJ by driving a transarticular Kirschner wire (0.045-inch, 0.062-inch, or 2.0-mm) from the distal ulna into the radius, positioned just proximal to the sigmoid notch.
- With the joint pinned and reduced, systematically tighten the repair sutures. Tie the knots securely over the dorsal cortical bridge of the distal radius, just proximal to the lunate fossa.
7. Capsular and Retinacular Closure
- Reattach the dorsal edge of the TFCC (the dorsal radioulnar ligament) to the dorsoulnar aspect of the distal radius. Suture it directly to the previously reflected flap of periosteum using 3-0 absorbable sutures.
- Retinacular Augmentation: If the dorsal radioulnar ligament is found to be attenuated or of poor tissue quality, reinforce the repair using a flap of the extensor retinaculum (created during the initial Z-plasty), based at the dorsoradial margin of the ECU sheath.
- Close the ulnocarpal joint capsule, the remaining extensor retinaculum, and the skin in sequential anatomical layers.
POSTOPERATIVE CARE AND REHABILITATION
Strict adherence to postoperative protocols is mandatory to protect the transosseous repair while mitigating the risk of profound wrist stiffness.
- 0 to 2 Weeks: The patient is placed in a well-molded, long-arm cast with the forearm in neutral to slight supination. At 2 weeks, the cast is removed for wound inspection, suture removal, and pin site care. A new long-arm cast is immediately applied.
- 4 to 6 Weeks: The transarticular radioulnar Kirschner pins are removed in the clinic. The patient remains immobilized in the long-arm cast.
- 8 Weeks: The long-arm cast is discontinued (total cast time: 8 weeks). The patient is transitioned to a custom-molded, long-arm thermoplastic splint. A therapist-supervised rehabilitation program is initiated, focusing strictly on gentle, active forearm pronation-supination and wrist flexion-extension exercises. Passive stretching is contraindicated at this stage.
- 10 to 14 Weeks: As active range of motion improves, a progressive strengthening program is introduced. The long-arm splint is gradually weaned (worn for a total of 6 weeks post-cast removal).
- Return to Activity: Return to heavy manual labor or competitive sports is delayed until the patient achieves a pain-free range of motion and grip strength reaches at least 80% of the contralateral, uninjured extremity (typically 4 to 6 months postoperatively).
CHRONIC INSTABILITY OF THE DISTAL RADIOULNAR JOINT
While acute Class 1D injuries can often be successfully repaired, delayed presentation or failure of initial management leads to chronic DRUJ instability. This condition is highly debilitating and presents complex reconstructive challenges.
Pathophysiology and Etiology
Symptomatic chronic instability of the DRUJ may manifest following:
1. Isolated, unrecognized trauma to the DRUJ (missed TFCC tears).
2. Malunion of distal radius and ulna fractures.
3. Unsuccessful primary attempts to repair the TFCC.
4. Degenerative or inflammatory arthritis (e.g., Rheumatoid Arthritis) destroying the ligamentous constraints.
The Role of Distal Radius Malunion
The kinematics of the DRUJ are exquisitely sensitive to the spatial relationship between the radius and the ulna. Cadaveric biomechanical studies have definitively shown that architectural distortion of the distal radius profoundly disrupts DRUJ congruity:
* Sagittal Plane Angulation: Angulation of distal radial fractures resulting in a volar convexity (dorsal tilt) of more than 20 to 30 degrees significantly alters the tension of the radioulnar ligaments, leading to dorsal subluxation of the ulna.
* Radial Shortening: Radial shortening is the most critical factor disturbing radioulnar kinematics. Shortening of more than 5 mm implies catastrophic damage to the TFCC and invariably leads to ulnocarpal abutment and DRUJ subluxation.
Ulnar Styloid Fractures
The relationship between ulnar styloid fractures and DRUJ instability remains a topic of academic debate. However, a landmark clinical study of 166 distal radial fractures by May et al. suggested that significantly displaced fractures through the base of the ulnar styloid—where the deep radioulnar ligaments (the foveal attachment) insert—highly correlate with chronic DRUJ instability. Tip fractures, which only involve the superficial collateral ligaments, rarely cause instability.
Clinical Presentation of Chronic Instability
Patients with symptomatic chronic DRUJ instability typically present with profound weakness, a painful clunk during forearm rotation, and symptoms directly related to the dorsal displacement of the distal ulna. The "piano key" sign (dorsal prominence of the ulnar head that is easily ballotable) is a hallmark clinical finding.
While most acute injuries, when treated with the rigorous open repair techniques described above, result in a stable DRUJ, chronic cases often require complex salvage procedures. These may include anatomic ligament reconstructions (e.g., Adams-Berger procedure using tendon allografts), ulnar shortening osteotomies to tighten the interosseous membrane and ulnocarpal ligaments, or, in cases of severe arthrosis, salvage operations such as the Darrach procedure, Sauvé-Kapandji procedure, or total DRUJ arthroplasty.
CONCLUSION
The open repair of Class 1D TFCC injuries is a technically demanding but highly rewarding procedure. By meticulously restoring the anatomical footprint of the radioulnar ligaments at the sigmoid notch via transosseous fixation, surgeons can reliably restore DRUJ stability. Success relies heavily on precise surgical execution, recognition and management of ulnar variance, rigid temporary transarticular pinning, and strict adherence to a phased, prolonged postoperative rehabilitation protocol.
You Might Also Like