Matched and Wafer Distal Ulnar Resection: A Comprehensive Surgical Guide
Key Takeaway
Distal ulnar resection encompasses joint-sparing and joint-sacrificing techniques to address distal radioulnar joint (DRUJ) pathology. The matched ulnar resection, pioneered by Watson, contours the distal ulna to articulate smoothly with the radius, preserving the ulnar sling mechanism. Alternatively, the wafer procedure decompresses the ulnocarpal joint while retaining the triangular fibrocartilage complex (TFCC) and ulnar styloid. Proper patient selection and meticulous surgical execution are paramount to restoring pain-free forearm rotation and grip strength.
Introduction to Distal Ulnar Resection Arthroplasty
Pathology of the distal radioulnar joint (DRUJ) and the ulnocarpal articulation presents a complex biomechanical challenge in orthopedic hand and wrist surgery. Conditions such as severe rheumatoid arthritis, post-traumatic osteoarthritis, and ulnar impaction syndrome frequently lead to debilitating wrist pain, restricted forearm rotation, and diminished grip strength. Historically, the Darrach procedure (simple resection of the distal ulna) was the gold standard; however, it frequently resulted in painful radioulnar convergence, ulnar stump instability, and extensor tendon rupture.
To mitigate the complications associated with traditional distal ulnar excision, advanced techniques such as the “Matched” Distal Ulnar Resection (described by Watson et al.) and the Wafer Distal Ulnar Resection (described by Feldon) were developed. These procedures are meticulously designed to decompress the ulnar side of the wrist while preserving the critical soft-tissue stabilizers, most notably the triangular fibrocartilage complex (TFCC) and the extensor carpi ulnaris (ECU) subsheath.
This comprehensive guide details the indications, biomechanical principles, step-by-step surgical techniques, and postoperative rehabilitation protocols for both the matched and wafer distal ulnar resection procedures.
Biomechanics and Pathoanatomy of the DRUJ
A profound understanding of DRUJ kinematics is mandatory before undertaking any distal ulnar resection. The DRUJ is a highly constrained soft-tissue joint with minimal inherent osseous stability. The radius rotates around the fixed ulna during pronation and supination, translating volarly in pronation and dorsally in supination.
The Ulnar Sling Mechanism
The stability of the distal ulna is governed by the "ulnar sling" mechanism, a complex fascial and ligamentous network comprising:
* The Triangular Fibrocartilage Complex (TFCC).
* The Extensor Carpi Ulnaris (ECU) tendon and its robust subsheath.
* The volar and dorsal radioulnar ligaments.
* The pronator quadratus.
💡 Clinical Pearl
The primary goal of modern distal ulnar resection is not merely bone removal, but the meticulous preservation and re-tensioning of the ulnar sling mechanism. Failure to preserve the deep fascia of the ECU sheath inevitably leads to dorsal subluxation of the ulnar stump and dynamic radioulnar impingement.
“Matched” Distal Ulnar Resection (Watson Technique)
Watson et al. conceptualized the matched ulnar arthroplasty to address DRUJ pathology caused by rheumatoid arthritis and post-traumatic deformities. Unlike the transverse osteotomy of a traditional Darrach procedure, the matched resection contours the distal ulna into a long, sloping shape. This geometry matches the contour of the distal radius, allowing full supination and pronation without impingement, while permitting the large cancellous surface of the resected ulna to adhere securely to the ulnar sling mechanism.
Indications
- Advanced rheumatoid arthritis with DRUJ destruction.
- Post-traumatic DRUJ osteoarthritis.
- Failed prior DRUJ procedures (salvage).
- Chronic, irreparable DRUJ instability with secondary arthritic changes.
Contraindications
- Longitudinal radioulnar dissociation (Essex-Lopresti injury).
- Incompetent ulnar soft-tissue envelope (lack of an intact ECU subsheath or capsular sling).
- High-demand manual laborers (relative contraindication, as grip strength may be permanently reduced).
Surgical Technique: Matched Distal Ulnar Resection
1. Patient Positioning and Preparation
- Place the patient supine on the operating table with the operative arm extended onto a radiolucent hand table.
- Administer regional or general anesthesia.
- Apply a well-padded proximal pneumatic tourniquet.
- Following standard limb exsanguination, inflate the tourniquet to 250 mm Hg (or 100 mm Hg above systolic pressure).
- Prepare and drape the hand and forearm in a standard sterile fashion.
- Fully pronate the forearm on the hand table to bring the distal ulna into a prominent dorsal position.
2. Surgical Approach
- Incise the skin dorsally in a transverse straight line or a zigzag pattern, centered approximately 2.5 cm proximal to the distal end of the ulna.
- Carefully dissect through the subcutaneous tissues, identifying and protecting the dorsal sensory branches of the ulnar nerve.
- Identify the extensor retinaculum and open its proximal edge to expose the distal ulna and the ECU compartment.
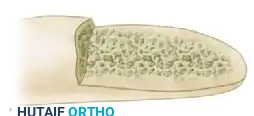
3. Osseous Resection and Contouring
- Elevate the periosteum minimally to expose the distal 5 to 6 cm of the ulna.
- Using a combination of rongeurs, a high-speed burr, or an oscillating saw, resect the distal ulna in a long, sloping shape over a distance of 5 to 6 cm.
- The final contour of the distal ulna must resemble an eccentrically sharpened pencil. This specific geometry prevents point-loading against the radius.
- Usually, the ulnar styloid is resected. Ensure that the distal tip of the resected ulna lies at, or just proximal to, the articular surface of the radius.

- Supinate and pronate the forearm while palpating the space between the radius and the contoured ulna. Ensure that the surfaces are parallel and matching throughout the entire arc of motion.
⚠️ Surgical Warning
If the contoured ulna abuts against the articular sulcus of the distal radius during rotation, you must remove a sufficient amount of the radial sigmoid notch to allow completely free, frictionless movement.
4. Soft Tissue Management (The Ulnar Sling)
- CRITICAL STEP: Leave the deep fascia of the extensor carpi ulnaris (ECU) sheath firmly attached to the periosteum of the ulna. This soft-tissue tether is the primary defense against radioulnar shaft approximation (convergence) and stylocarpal impingement.
- Do not interpose soft tissues between the radius and ulna, as the goal is for the large cancellous surface of the distal ulna to adhere directly to the ulnar sling mechanism, creating a stable, fibrous pseudoarthrosis.
5. Closure
- Confirm free forearm rotation one final time.
- Deflate the tourniquet and obtain meticulous hemostasis using bipolar electrocautery to prevent postoperative hematoma.
- Close the wound by first replacing the ECU compartment. If the native tissue is deficient, utilize a local retinacular flap to stabilize the dorsal aspect of the ulnar stump.
- Close the skin with non-absorbable sutures.
6. Splinting
- If no ulnar shortening was required: Apply a short-arm bulky dressing reinforced with dorsal and palmar plaster splints.
- If ulnar shortening was performed: Apply a rigid sugar-tong splint to strictly control forearm rotation.
Postoperative Care: Matched Resection
The postoperative protocol is dictated by the extent of the resection and whether concurrent ulnar shaft shortening was performed.
- 0 to 2 Weeks: The patient remains in the initial postoperative splint. Elevation and active digit range of motion (ROM) are encouraged immediately to prevent tendon adhesions and reduce edema.
- At 2 Weeks: The splint and skin sutures are removed.
- Standard Resection: A removable short-arm wrist splint is applied. Gentle, active forearm rotation is initiated.
- With Ulnar Shortening: A short-arm cast is applied for an additional 2 weeks to protect the osteotomy site.
- 4 to 6 Weeks: The wrist splint is discontinued for standard resections. Progressive strengthening begins. Most activities of daily living can be resumed.
- 8 to 12 Weeks: For patients who underwent diaphyseal ulnar shortening, cast or splint immobilization continues until radiographic union is confirmed.
- Long-Term: Patients are counseled that return to heavy manual labor may be prolonged, and extreme power-grip activities may be permanently restricted due to altered DRUJ biomechanics.
Wafer Distal Ulnar Resection
While the matched resection is ideal for severe DRUJ destruction, the Wafer Procedure is a joint-sparing alternative designed specifically for ulnocarpal impaction syndrome and central TFCC tears. By resecting only the distal 2 to 4 mm of the ulnar dome (the "wafer"), the surgeon decompresses the ulnocarpal joint while meticulously preserving the ulnar styloid, the DRUJ ligaments, and the peripheral attachments of the TFCC.
Indications
- Ulnar impaction syndrome (ulnocarpal abutment) with positive ulnar variance (typically < 3-4 mm).
- Central, degenerative tears of the TFCC (Palmer Type 2A, 2B, 2C).
- Lunotriquetral ligament tears secondary to ulnar impaction.
Contraindications
- Severe DRUJ osteoarthritis (requires matched resection, Darrach, or Sauvé-Kapandji).
- Ulnar variance greater than +4 mm (better treated with a diaphyseal ulnar shortening osteotomy).
- DRUJ instability.
Surgical Technique: Wafer Distal Ulnar Resection
1. Exposure and Joint Assessment
- The procedure can be performed open or arthroscopically. In the open technique, a dorsal longitudinal incision is made over the DRUJ.
- The extensor retinaculum is incised over the fifth extensor compartment (extensor digiti minimi).
- A dorsal capsulotomy is performed to expose the ulnocarpal joint and the proximal surface of the TFCC.
2. TFCC Evaluation
- Inspect the TFCC. In cases of ulnar impaction, a central degenerative tear is frequently present.
- Pass a probe through the TFCC tear to directly visualize the ulnar head beneath it.

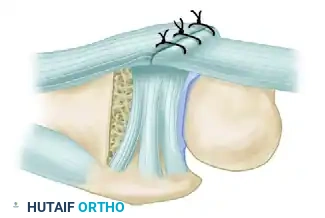
3. The Wafer Resection
- Using a high-speed burr or a fine osteotome, resect the distal 2 to 4 mm of the ulnar articular dome.
- Crucial Anatomy: The resection must be limited to the articular portion of the ulnar head that articulates with the carpus. The ulnar styloid process and the foveal attachments of the TFCC must remain completely intact to preserve DRUJ stability.

- Ensure adequate decompression by passively translating the carpus and confirming that the lunate and triquetrum no longer abut the distal ulna during maximum ulnar deviation and pronation.
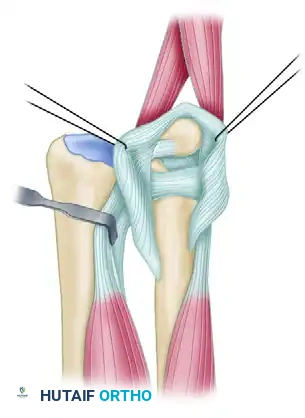
4. TFCC Repair and Closure
- If the TFCC is unstable or redundant following the bony resection, it must be tensioned.
- Place a row of non-absorbable sutures anchoring the dorsal edge of the TFCC to the dorsal capsule. This suspends the TFCC under normal tension and stabilizes the ulna during the healing phase.

- Close the dorsal capsule and the extensor retinaculum. Deflate the tourniquet, achieve hemostasis, and close the skin.
- Apply a bulky hand dressing supported by a volar wrist splint.
Postoperative Care: Wafer Resection
Because the DRUJ ligaments and the ulnar styloid are preserved, rehabilitation following a wafer resection is generally faster than after a matched resection.
- 0 to 7 Days: The wrist is immobilized in the postoperative splint. Strict elevation and active finger motion are mandated.
- At 7 to 10 Days: The splint is removed. A formal course of rehabilitation is initiated, directed at achieving full, active mobilization of the wrist and forearm.
- 10 to 14 Days: Skin sutures are removed.
- 4 to 6 Weeks: Most normal activities of daily living can be resumed. Strengthening exercises for grip and forearm rotation are advanced.
- 8 to 12 Weeks: Return to heavy labor, forceful gripping, and high-impact sports is permitted once the patient is pain-free and has regained symmetrical grip strength.
Complications and Salvage Strategies
While both the matched and wafer resections offer excellent outcomes when indicated, complications can arise from technical errors or progressive disease.
1. Radioulnar Convergence and Impingement
Most commonly seen if the matched resection is too short or if the ECU subsheath is compromised. The remaining ulnar stump converges toward the radius, causing painful impingement during rotation.
* Prevention: Ensure a long, 5-6 cm sloping resection (the "sharpened pencil") and meticulously preserve the ECU fascia.
* Salvage: Revision contouring, soft-tissue interposition arthroplasty, or conversion to a constrained DRUJ prosthesis.
2. Extensor Carpi Ulnaris (ECU) Subluxation
Failure to repair the dorsal retinaculum or the ECU subsheath can lead to painful snapping of the ECU tendon over the ulnar stump during supination.
* Prevention: Utilize a retinacular flap during closure if the native tissue is attenuated.
* Salvage: Surgical reconstruction of the ECU subsheath using a portion of the extensor retinaculum.
3. Persistent Ulnocarpal Pain (Failed Wafer)
If a wafer resection fails to adequately decompress the ulnocarpal joint (often due to unrecognized severe positive ulnar variance > 4mm), the patient will continue to experience impaction symptoms.
* Prevention: Accurate preoperative radiographic assessment of ulnar variance. Choose a diaphyseal shortening osteotomy for variance > 4mm.
* Salvage: Conversion to a formal ulnar shortening osteotomy or a matched distal ulnar resection.
Conclusion
Distal ulnar resection remains a cornerstone in the surgical management of DRUJ and ulnocarpal pathology. The Matched Distal Ulnar Resection provides a reliable, joint-sacrificing option for severe arthritis, relying on precise osseous contouring and soft-tissue preservation to maintain stability. Conversely, the Wafer Resection offers a joint-sparing, highly targeted decompression for ulnar impaction syndrome, preserving the vital kinematics of the DRUJ. Mastery of both techniques, coupled with rigorous patient selection and meticulous postoperative care, ensures optimal functional restoration for the complex wrist patient.
You Might Also Like