Operative Management of Madelung Deformity

Key Takeaway
Madelung deformity is a rare congenital condition characterized by premature growth arrest of the volar-ulnar distal radial physis. Surgical intervention is indicated for persistent pain, functional deficit, or progressive deformity. Techniques include Vickers ligament excision in skeletally immature patients, combined with distal radius dome osteotomy or Watson balanced radial osteotomy to restore carpal alignment, correct ulnar positive variance, and optimize distal radioulnar joint kinematics.
INTRODUCTION AND PATHOANATOMY
Madelung deformity is a complex congenital abnormality of the wrist characterized by a primary growth disturbance of the palmar and ulnar aspects of the distal radial physis. This localized premature physeal arrest leads to a progressive, multiplanar deformity of the radiocarpal and distal radioulnar joints (DRUJ). The condition is predominantly bilateral, exhibits a strong female predilection, and typically becomes clinically apparent during the adolescent growth spurt.
Genetically, Madelung deformity is frequently associated with mutations or deletions in the short stature homeobox-containing (SHOX) gene, commonly presenting as a manifestation of Léri-Weill dyschondrosteosis or Turner syndrome.
The pathoanatomic hallmark of Madelung deformity is the presence of the Vickers ligament, an anomalous, thickened radiolunate ligament. This structure originates from the volar-ulnar metaphysis of the radius and inserts onto the lunate, creating a robust tether across the volar-ulnar physis.
Biomechanics of the Deformity
The tethering effect of the Vickers ligament, combined with the asymmetric growth arrest of the distal radius, produces a predictable cascade of biomechanical alterations:
* Distal Radius: Develops an exaggerated volar tilt and ulnar inclination.
* Carpus: The lunate subsides proximally into the V-shaped defect created between the deformed radius and the relatively overgrown ulna. The entire carpus translates palmarly and ulnarly.
* Distal Ulna: Continues to grow normally, resulting in significant positive ulnar variance, dorsal subluxation of the ulnar head, and severe DRUJ incongruity.
Clinical Pearl: The dorsal prominence of the distal ulna is often the primary cosmetic complaint of the patient, but the primary source of pain is typically ulnocarpal impaction and radiocarpal incongruity driven by the volar-ulnar subsidence of the carpus.
CLINICAL PRESENTATION AND EVALUATION
Patients typically present between the ages of 8 and 14 years. The classic triad of symptoms includes:
1. Deformity: Prominent dorsal distal ulna and volar translation of the hand.
2. Pain: Insidious onset of ulnar-sided wrist pain, exacerbated by weight-bearing or forceful grip.
3. Decreased Range of Motion: Profound limitation in forearm supination and wrist extension.
Radiographic Evaluation
Standard posteroanterior (PA) and lateral radiographs of the wrist are mandatory.
Key radiographic parameters to assess include:
* Ulnar Tilt: Often exceeds 33 degrees (normal is 22 degrees).
* Volar Tilt: Markedly increased on the lateral view, often exceeding 20-25 degrees.
* Lunate Subsidence: The lunate migrates proximally past the articular surface of the radius.
* Ulnar Variance: Severe positive ulnar variance is universally present in advanced cases.
* Carpal Slip: The entire proximal carpal row shifts ulnarly and palmarly.
Advanced imaging, such as Magnetic Resonance Imaging (MRI), is highly sensitive for identifying the Vickers ligament and evaluating the integrity of the triangular fibrocartilage complex (TFCC), which is often attenuated or torn due to chronic DRUJ subluxation.
INDICATIONS FOR SURGERY
Surgical intervention is not strictly indicated for asymptomatic, mild deformities. However, operative management is highly recommended for:
* Persistent, intractable wrist pain failing conservative management (splinting, NSAIDs).
* Progressive functional limitations, particularly severe loss of supination.
* Progressive radiographic deformity in a skeletally immature patient.
* Severe cosmetic deformity causing significant psychological distress.
Surgical Warning: Prophylactic release of the Vickers ligament in asymptomatic patients remains controversial. However, in skeletally immature patients with documented progression, early physiolysis and ligament excision can prevent the need for complex corrective osteotomies later in life.
SURGICAL MANAGEMENT STRATEGIES
The surgical approach to Madelung deformity is dictated by the patient's skeletal maturity and the severity of the deformity.
1. Vickers Ligament Excision and Dome Osteotomy (Carter and Ezaki)
Carter and Ezaki established a foundational algorithm for managing Madelung deformity. They recommended excision of the ligament of Vickers alone in very young, skeletally immature patients to release the tether and allow potential remodeling of the physis.
If considerable deformity already exists, they advocated for combining the ligament excision with a dome distal radial osteotomy.
* Biomechanics of the Dome Osteotomy: The dome shape allows for multiplanar correction (restoring volar tilt and ulnar inclination) without the need for structural bone grafting. It maximizes cancellous bone contact, ensuring rapid union. Furthermore, the dome osteotomy tends to provide better volar coverage to the lunate and corrects some of the ulnar positive variance by effectively lengthening the radius.
* Clinical Outcomes: In their landmark series of 23 wrists, Carter and Ezaki noted the presence of a Vickers ligament in 91% of cases. Dome osteotomy was utilized in 16 wrists and successfully relieved pain in all patients.
* Ulnar Management: Despite radial correction, ulnar shortening may be required at a later date if ulnar wrist pain persists in association with positive ulnar variance. In the Carter and Ezaki series, 10 of the 23 wrists eventually required ulnar shortening to relieve persistent ulnar-sided wrist pain.
2. Watson et al. Balanced Radial Osteotomy
For severe deformities, Watson et al. described a highly effective "balanced" radial osteotomy. This technique utilizes a closing wedge on the radial aspect of the distal radius and an opening wedge on the ulnar aspect, effectively realigning the articular surface while simultaneously lengthening the radius to address ulnar positive variance.
STEP-BY-STEP SURGICAL TECHNIQUE
Preoperative Planning and Positioning
- Anesthesia: General anesthesia or regional brachial plexus block.
- Positioning: The patient is placed supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm.
- Fluoroscopy: A mini-C-arm must be positioned to allow seamless AP and lateral imaging throughout the procedure.
Approach and Vickers Ligament Excision
- Incision: An extended volar Henry approach is utilized. The incision is made over the flexor carpi radialis (FCR) tendon, extending distally across the wrist crease.
- Superficial Dissection: The FCR sheath is incised, and the tendon is retracted ulnarly to protect the median nerve. The radial artery is identified and carefully retracted radially.
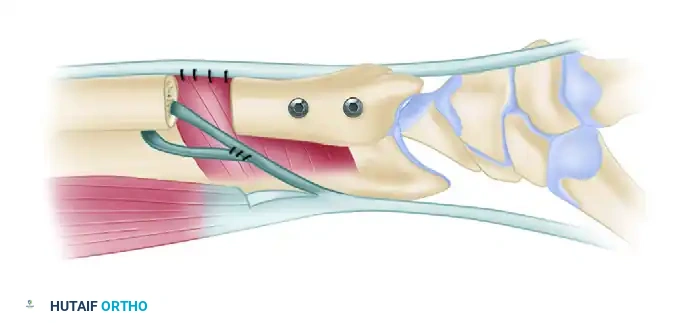
- Deep Dissection: The pronator quadratus is identified and elevated from its radial insertion, reflecting it ulnarly to expose the volar metaphysis of the distal radius.
- Identification of the Vickers Ligament: The anomalous ligament is identified as a thick, fibrous band originating from the volar-ulnar metaphysis, traversing the physis, and inserting onto the volar aspect of the lunate.
- Excision: The ligament is sharply excised. In skeletally immature patients, a localized physiolysis (resection of the tethered physeal bar) is performed, and interpositional fat may be placed to prevent reformation of the bony bar.
Execution of the Watson Balanced Radial Osteotomy
If the deformity is severe, the Watson balanced osteotomy is performed following ligament excision.
Step 1: Marking the Osteotomies
Under fluoroscopic guidance, the osteotomy sites are planned. A radial-sided bone wedge is marked on the distal radius.
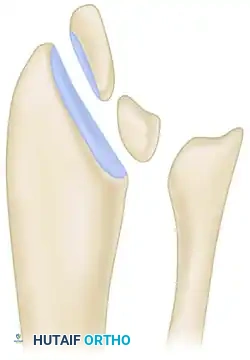
Osteotomies marked on the distal radius with the planned radial-sided bone wedge.
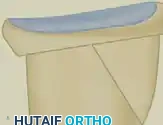
Step 2: Harvesting the Radial Wedge
Using an oscillating saw under continuous saline irrigation, the radial-sided closing wedge is carefully excised. This wedge will serve as the autograft for the ulnar side.

The radial-sided bone wedge is harvested, preparing the radius for realignment.
Step 3: Ulnar Opening Wedge and Graft Insertion
An opening osteotomy is performed on the ulnar side of the distal radius. The distal articular fragment is then rotated and tilted to restore normal volar tilt and ulnar inclination. The harvested radial bone wedge is inserted into the ulnar opening osteotomy to maintain the correction and effectively lengthen the radius.
The harvested bone wedge is inserted into the opening osteotomy on the ulnar side, balancing the radius.
Step 4: Ulnar Resection and Spike Excision
To address the severe DRUJ incongruity and positive ulnar variance, a matched ulnar resection (such as a Darrach procedure or ulnar shortening osteotomy) is often performed concurrently. Any residual radial spike resulting from the osteotomy translation must be meticulously excised to prevent soft tissue irritation or tendon rupture.

Matched ulnar resection has been performed; the prominent radial spike must be excised to ensure a smooth contour.
Fixation Strategy
Following the osteotomy and realignment, rigid internal fixation is required.
* In older adolescents and adults, a volar locking plate is the gold standard. The plate is applied to the volar surface of the radius, securing the distal fragment with locking screws and the proximal shaft with cortical screws.
* In younger, skeletally immature patients where plate placement might bridge and arrest an open physis, smooth Kirschner wires (K-wires) are utilized. Multiple 0.062-inch K-wires are driven percutaneously to stabilize the osteotomy and the inserted wedge.
Pitfall: Failure to adequately release the brachioradialis insertion can lead to a loss of correction and recurrent radial deviation of the distal fragment. Always release the brachioradialis prior to final fixation.
MANAGEMENT OF THE DISTAL ULNA
Addressing the distal ulna is a critical component of managing Madelung deformity. The choice of procedure depends on the patient's age, the severity of the DRUJ arthrosis, and the degree of positive ulnar variance.
- Ulnar Shortening Osteotomy (USO): Indicated for patients with positive ulnar variance but a relatively preserved DRUJ articular surface. This unloads the ulnocarpal joint and tightens the ulnocarpal ligaments. As noted by Carter and Ezaki, this may be performed as a staged procedure if ulnar pain persists after radial correction.
- Sauvé-Kapandji Procedure: Indicated for severe DRUJ arthrosis or fixed dorsal subluxation of the ulnar head. It involves an arthrodesis of the DRUJ and the creation of a proximal ulnar pseudoarthrosis to restore forearm rotation.
- Darrach Procedure (Distal Ulnar Resection): Generally reserved for older, low-demand patients due to the risk of postoperative ulnar stump instability and convergence.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Optimal postoperative care is essential for maximizing functional outcomes and ensuring bony union.
- Phase I (0-2 Weeks): The patient is placed in a bulky, well-padded short-arm volar splint in neutral rotation. Elevation and strict digital range of motion (ROM) exercises are initiated immediately to prevent tendon adhesions and reduce edema.
- Phase II (2-6 Weeks): Sutures are removed at 10-14 days. If rigid plate fixation was achieved, the patient may be transitioned to a removable thermoplastic splint, and gentle active ROM of the wrist and forearm is initiated. If K-wires were used, the patient is placed in a short-arm cast for 4-6 weeks until radiographic union is evident.
- Phase III (6-12 Weeks): K-wires (if used) are removed in the clinic. Formal occupational therapy is commenced, focusing on progressive stretching, restoration of supination, and gradual strengthening.
- Phase IV (>12 Weeks): Return to heavy lifting and contact sports is permitted only after complete radiographic consolidation of the osteotomy and restoration of near-normal grip strength.
COMPLICATIONS AND PITFALLS
While surgical correction of Madelung deformity yields high satisfaction rates, surgeons must be prepared to manage potential complications:
- Recurrent Deformity: Most common in skeletally immature patients who undergo isolated Vickers ligament release without osteotomy, or if the physeal bar is inadequately resected.
- Nonunion/Delayed Union: Particularly a risk at the ulnar opening wedge site if the autograft is poorly compressed or if fixation is inadequate.
- Hardware Irritation: Volar plates may irritate the flexor tendons, necessitating hardware removal after bony union.
- Persistent Ulnar Pain: Often due to unrecognized or unaddressed ulnocarpal impaction. This underscores the importance of Carter and Ezaki's observation that secondary ulnar shortening is frequently required.
- Nerve Injury: The superficial branch of the radial nerve (SBRN) and the median nerve are at risk during the volar approach and must be meticulously protected throughout the procedure.
CONCLUSION
The operative management of Madelung deformity requires a profound understanding of its unique pathoanatomy and biomechanics. By systematically addressing the tethering Vickers ligament, restoring the articular geometry of the distal radius through dome or balanced osteotomies, and managing the inevitable ulnar variance, orthopedic surgeons can reliably alleviate pain, restore function, and correct the cosmetic deformity associated with this challenging condition.
📚 Medical References
- Madelung Deformity Carter PR, Ezaki M: Madelung’s deformity: surgical correction through the anterior approach, Hand Clin 16:713, 2000.
- Darrach W: Habitual forward dislocation of the head of the ulna, Ann Surg 57:928, 1913.
- Gelberman RH, Bauman T: Madelung’s deformity and dyschondrosteosis, J Hand Surg 5A:338, 1980.
- Madelung V: Die spontane Subluxation der Hand nach vome, Verh Dtsch Ges Chir 7:259, 1878.
- Malgaigne JF: Traité des fractures et des luxations, Paris, 18471855.
- [In Treatise on fractures, translated by JH Packard, Philadelphia, 1959, Lippincott.
Milch H: Cuff resection of the ulna for malunited Colles’ fracture, J Bone Joint Surg 23:311, 1941.](https://pubmed.ncbi.nlm.nih.gov/?term=In%20Treatise%20on%20fractures%2C%20translated%20by%20JH%20Packard%2C%20Philadelphia%2C%201959%2C%20Lippincott.%0A%0AMilch%20H%3A%20Cuff%20resection%20of%20the%20ulna%20for%20malunited%20Colles%E2%80%99%20fracture%2C%20J%20Bone%20Joint%20Surg%2023%3A311%2C%201941.)
- Ranawat CS, DeFiore J, Straub LR: Madelung’s deformity: an end-result study of surgical treatment, J Bone Joint Surg 57A:722, 1975.
- Vender MI, Watson HK: Acquired Madelung-like deformity in a gymnast, J Hand Surg 13A:19, 1988.
- Vickers DW: Langenskiöld’s operation (physiolysis) for congenital malformations of bone producing Madelung’s deformity and clinodactyly, J Bone Joint Surg 66B:778, 1984.
- Vickers D, Nielson G: : surgical prophylaxis (physiolysis) during the late growth period by resection of the dyschondrosteosis lesion, J Hand Surg 17B:401, 1992.
- Watson HK, Pitts EC, Herber S: Madelung’s deformity: surgical technique, J Hand Surg 18B:601, 1993.
- White GM, Weiland AJ: Madelung’s deformity: treatment by osteotomy of the radius and Lauenstein procedure, J Hand Surg 12A:202, 1987.
You Might Also Like