Operative Management of Sternoclavicular Joint Dislocations and Instability
Key Takeaway
Chronic anterior sternoclavicular joint dislocations are often well-tolerated, making nonoperative management the standard of care. However, in patients experiencing persistent weakness, fatigue, or symptomatic instability, surgical intervention may be warranted. This guide details the biomechanics, indications, and step-by-step surgical techniques for sternoclavicular joint reconstruction, emphasizing medial clavicle resection and costoclavicular stabilization while strictly avoiding catastrophic complications associated with metallic fixation.
INTRODUCTION TO THE STERNOCLAVICULAR JOINT
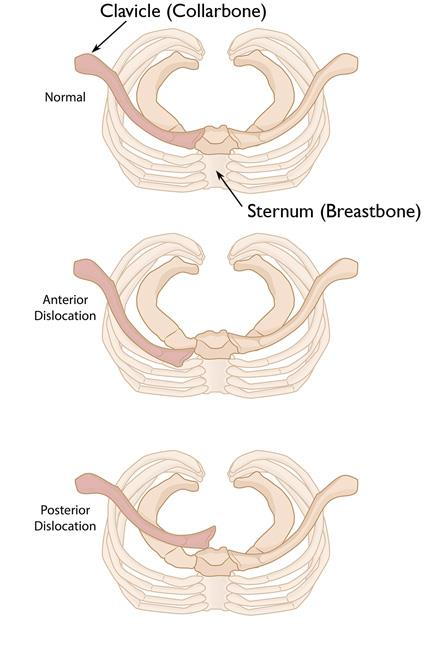
The sternoclavicular (SC) joint is the sole true synovial articulation connecting the appendicular skeleton of the upper extremity to the axial skeleton. Due to its unique diarthrodial saddle-shaped morphology and the presence of an intra-articular fibrocartilaginous disc, the SC joint possesses an extraordinary degree of mobility, facilitating elevation, depression, protraction, retraction, and axial rotation of the clavicle.
Despite its inherent osseous incongruity—where less than half of the medial clavicle articulates with the shallow clavicular notch of the manubrium—the SC joint is remarkably stable. This stability is conferred almost entirely by its robust ligamentous complex, primarily the posterior capsular ligament and the extra-articular costoclavicular (rhomboid) ligament. Consequently, dislocations of the SC joint are rare, accounting for less than 3% of all shoulder girdle injuries.
When dislocations do occur, they are predominantly anterior. Most authors and experienced shoulder surgeons agree that old, unreduced anterior dislocations of the sternoclavicular joint usually cause minimal, if any, functional disability. However, a distinct subset of patients—often heavy laborers or high-level athletes—may complain of persistent weakness, fatigue, and pain during strenuous use of the arm. It is in this highly selected demographic that surgical intervention may be considered, though it remains a formidable undertaking fraught with unique anatomical risks.
BIOMECHANICS AND PATHOANATOMY
Understanding the biomechanics of the SC joint is paramount before contemplating any surgical intervention. The joint acts as a pivot point for the shoulder girdle.
Ligamentous Stabilizers
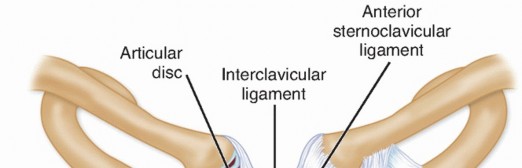
- Capsular Ligaments: The anterior and posterior capsular ligaments are thickenings of the joint capsule. Biomechanical studies have definitively shown that the posterior capsule is the most critical structure preventing both anterior and posterior translation of the medial clavicle.
- Costoclavicular Ligament: Often referred to as the rhomboid ligament, this structure consists of an anterior and posterior fasciculus. It anchors the inferior aspect of the medial clavicle to the first rib and its costal cartilage, resisting superior displacement and limiting elevation.
- Interclavicular Ligament: Spans the jugular notch, connecting the superomedial aspects of both clavicles, resisting downward displacement of the distal clavicle.
- Intra-articular Disc Ligament: A dense, fibrous structure that divides the joint into two separate synovial cavities. It acts as a shock absorber and prevents medial displacement of the clavicle over the manubrium.
Clinical Pearl: The posterior capsular ligament is the primary restraint to anterior translation. Therefore, in an anterior dislocation, the posterior capsule is invariably avulsed or ruptured, alongside the anterior capsule.
INDICATIONS AND CONTRAINDICATIONS FOR SURGERY
The Principle of "Skillful Neglect"
For the vast majority of chronic, unreduced anterior SC joint dislocations, the treatment of choice is nonoperative. Rockwood famously championed the concept of "skillful neglect." Because the medial clavicle displaces anteriorly, it moves away from the vital mediastinal structures (trachea, esophagus, great vessels, and brachial plexus). Patients typically develop a painless pseudarthrosis and regain near-normal shoulder kinematics.
Indications for Surgical Intervention
Surgery is rarely, if ever, indicated primarily for acute or chronic anterior dislocations. However, operative management may be considered in the following scenarios:
* Intractable Pain and Weakness: Patients who experience debilitating fatigue or weakness of the upper extremity during heavy lifting or athletic endeavors.
* Underlying Joint Laxity: Patients with symptomatic, multidirectional instability of the SC joint that has failed extensive conservative rehabilitation (scapular stabilization protocols).
* Failed Prior Reconstructions: Patients who have undergone previous attempts at stabilization (using sutures, fascia, or tendons) that have subsequently failed, leading to painful degenerative changes.
Contraindications
- Asymptomatic or mildly symptomatic anterior dislocations.
- Patients unwilling or unable to comply with strict postoperative immobilization protocols.
- Absolute Contraindication: The use of unconstrained metallic hardware (e.g., Steinmann pins, Kirschner wires) across the SC joint.
Surgical Warning: Migration of metallic fixation in the sternoclavicular joint can occur with disastrous, often fatal, consequences. K-wires and Steinmann pins have been documented to migrate into the aorta, heart, pulmonary artery, and spinal cord. Under no circumstances should transarticular metallic pins be used for SC joint stabilization.
HISTORICAL AND ALTERNATIVE SURGICAL PROCEDURES
When surgery is deemed necessary, the surgeon must choose between anatomical reconstruction, extra-anatomical stabilization, or resection arthroplasty. Historically, several basic surgical procedures have been described, reflecting the difficulty of achieving durable stability in this joint.
Fascial and Tendinous Reconstructions
- Speed, Key, and Conwell Technique: Described the use of an autologous fascia lata graft looped around the medial clavicle and the first rib to recreate the costoclavicular ligament.
- Bankart and Milch Technique: Utilized a fascia lata graft passed directly between the clavicle and the sternum to reconstruct the capsular ligaments.
- Burrows Technique: Recommended the use of the subclavius tendon, mobilizing its lateral insertion and routing it to stabilize the medial clavicle.
The Booth and Roper Procedure
Booth and Roper recognized the need for a robust, vascularized stabilization method. They recommended a subperiosteal dissection of the sternal origin of the sternocleidomastoid (SCM) muscle, extending inferiorly to include a strip of sternal periosteum.
* Technique: This tendoperiosteal strip is left attached superiorly, threaded subperiosteally under the medial end of the first rib, passed up behind the rib, and then routed through a drill hole (oriented superior to inferior) in the medial clavicle. The strip is then tensioned and sutured back onto itself.
* Advantage: Utilizes local, vascularized tissue.
* Disadvantage: Technically demanding and relies on the integrity of the sternal periosteum, which may be attenuated in chronic instability.
MEDIAL CLAVICLE RESECTION AND ARTHROPLASTY
Resection of the medial end of the clavicle has been advocated by prominent authors including Salvatore, DePalma, Rockwood, Bateman, and Milch. It is particularly indicated when the SC joint exhibits severe degenerative joint disease (osteoarthritis) or in cases of chronic, irreducible dislocations where the articular surfaces are deformed.
The Biomechanical Dilemma of Resection
A critical caveat of medial clavicle resection is the potential for postoperative upper extremity weakness and iatrogenic instability. The costoclavicular (rhomboid) ligament inserts approximately 1.0 to 1.5 cm lateral to the medial articular surface of the clavicle.
Pitfall: If the medial end of the clavicle is resected for degenerative changes, the surgeon must be meticulously careful not to damage the costoclavicular ligament. Resecting more than 1.5 cm of the medial clavicle without reconstructing the costoclavicular ligament will result in gross multidirectional instability of the remaining clavicle.
Rockwood’s Resection and Stabilization Technique
For patients in whom attempts to reduce and stabilize the joint have failed, or those with severe chronic symptoms, Rockwood recommended a formal sternoclavicular arthroplasty with resection of the medial clavicle and concurrent stabilization.
Key Elements of the Rockwood Procedure:
1. Resection: Excision of exactly 1 inch (2.5 cm) of the medial clavicle.
2. Débridement: Complete excision of the intra-articular disc ligament and degenerative capsular tissue.
3. Stabilization: Because a 1-inch resection inevitably sacrifices the costoclavicular ligament, the remaining medial clavicle must be stabilized to the first rib. Rockwood utilized a 3-mm cotton Dacron tape or a robust strip of autologous fascia lata passed in a figure-of-eight fashion.
4. Muscle Transfer: Detachment of the clavicular head of the sternocleidomastoid muscle. This temporarily eliminates the deforming superior pull of the SCM on the clavicle, protecting the reconstruction during the healing phase.
STEP-BY-STEP SURGICAL APPROACH: SC JOINT ARTHROPLASTY AND RECONSTRUCTION
The following details the contemporary approach to medial clavicle resection and costoclavicular reconstruction, heavily influenced by Rockwood's principles.
1. Patient Positioning and Anesthesia
- Anesthesia: General endotracheal anesthesia is mandatory. A thoracic surgeon should be alerted and available on standby due to the proximity of the great vessels.
- Positioning: The patient is placed in the supine or modified beach-chair position. A rolled towel or sandbag is placed between the scapulae to allow the shoulders to fall posteriorly, opening the anterior SC joint space.
- Prep and Drape: The entire forequarter, neck, and anterior chest (down to the costal margin) must be prepped and draped free to allow full manipulation of the upper extremity.
2. Incision and Exposure
- A 7 to 8 cm transverse incision is made centered over the medial clavicle, extending medially over the manubrium.
- Subcutaneous tissues and the platysma are divided in line with the incision.
- The supraclavicular nerves should be identified and protected to prevent painful postoperative neuromas.
3. Subperiosteal Dissection and SCM Detachment
- The periosteum of the medial clavicle is incised longitudinally.
- Crucial Step: The clavicular head of the sternocleidomastoid muscle is carefully detached from the superior aspect of the medial clavicle. This removes the superior deforming force.
- Subperiosteal dissection is carried circumferentially around the medial clavicle.
- Warning: Posterior dissection must be strictly subperiosteal. A blunt retractor (e.g., a malleable ribbon or Darrach retractor) is carefully placed posterior to the clavicle to protect the brachiocephalic vein, common carotid artery, and pleura.
4. Medial Clavicle Resection
- Using a microsagittal saw, an osteotomy is performed exactly 1 inch (2.5 cm) lateral to the articular surface.
- The medial fragment is carefully elevated. The intra-articular disc ligament and any remaining capsular attachments are sharply excised.
- The medullary canal of the remaining lateral clavicular stump is identified and slightly smoothed with a rasp to prevent fraying of the graft.
5. Costoclavicular Stabilization (Figure-of-Eight)
- Attention is turned to the first rib. The subclavius muscle is elevated to expose the superior surface of the first rib.
- Subperiosteal dissection is performed around the first rib. A curved ligature carrier or right-angle clamp is passed carefully under the first rib from anterior to posterior.
- Two drill holes (4.5 mm) are made in the superior cortex of the remaining clavicular stump, approximately 1 cm lateral to the osteotomy site.
- A robust graft (semitendinosus allograft, autologous fascia lata, or heavy non-absorbable tape) is passed under the first rib and threaded through the drill holes in the clavicle in a figure-of-eight configuration.
- The shoulder is pushed posteriorly (reducing the clavicle inferiorly), and the graft is tensioned and tied/sutured securely.
6. Closure
- The detached clavicular head of the sternocleidomastoid is loosely sutured to the anterior fascia or the pectoralis major fascia, rather than directly back to the clavicle, to prevent immediate superior tension.
- The platysma is closed meticulously to ensure a cosmetically acceptable scar.
- Subcutaneous tissues and skin are closed in a standard fashion.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of a sternoclavicular joint reconstruction relies as much on strict postoperative compliance as it does on surgical execution.
- Phase I (Weeks 0-6): The patient is placed in a strict shoulder immobilizer or sling. Absolute restriction of active shoulder elevation and abduction. Pendulum exercises and elbow/wrist/hand range of motion (ROM) are permitted.
- Phase II (Weeks 6-10): The sling is discontinued. Gentle, progressive passive and active-assisted ROM begins. Forward elevation is limited to 90 degrees initially.
- Phase III (Weeks 10-16): Full active ROM is restored. Gradual strengthening of the periscapular stabilizers (trapezius, rhomboids, serratus anterior) and rotator cuff is initiated.
- Phase IV (Months 4-6): Return to heavy lifting, manual labor, or contact sports is generally restricted until at least 6 months postoperatively, contingent upon the restoration of normal strength and the absence of pain.
COMPLICATIONS
Surgical intervention at the SC joint is not without significant risk. Surgeons must be prepared to manage the following complications:
1. Neurovascular Injury: The most feared complication. Penetration of the posterior periosteal sleeve can result in catastrophic injury to the brachiocephalic vessels, pneumothorax, or damage to the recurrent laryngeal nerve.
2. Recurrent Instability: Often due to graft failure, inadequate tensioning, or failure to detach the SCM muscle, leading to superior migration of the clavicular stump.
3. Upper Extremity Weakness: As noted by Salvatore and DePalma, resection of the medial clavicle alters the biomechanical resting length of the shoulder girdle musculature, which can result in subjective weakness during overhead activities.
4. Cosmetic Deformity: The loss of the medial clavicular prominence leaves a visible asymmetry at the base of the neck, which patients must be counseled about preoperatively.
CONCLUSION
While the sternoclavicular joint is critical for normal shoulder mechanics, chronic anterior dislocations are remarkably well-tolerated by the majority of patients. The primary indication for surgery remains intractable pain or functional weakness that precludes normal activity. When operative intervention is mandated, the historical use of transarticular metallic pins must be absolutely avoided. Instead, a meticulously performed medial clavicle resection combined with a robust costoclavicular ligament reconstruction—respecting the delicate posterior mediastinal anatomy—provides the most reliable and safe pathway to restoring function and alleviating pain.
You Might Also Like