Proximal Humerus Fractures: Essential Guide to Anatomy & Recovery
Key Takeaway
For anyone wondering about Proximal Humerus Fractures: Essential Guide to Anatomy & Recovery, Humerus fractures proximal are a common injury, representing 4-5% of all fractures and 45% of humerus fractures. With an incidence of 300,000 annually, they often result from a fall onto an outstretched arm in older individuals with osteoporosis, making them fragility fractures. Most (85%) are nondisplaced, affecting women more than men due to osteoporosis.
Introduction and Epidemiology
Proximal humerus fractures represent a significant and growing proportion of orthopedic trauma, comprising approximately 4% to 5% of all fractures and accounting for 45% of all humeral fractures. The annual incidence in the United States is estimated at over 300,000 cases, a figure that surpasses the incidence of proximal femur (hip) fractures. This rising prevalence is inextricably linked to an aging demographic and the associated increase in osteoporotic bone conditions.
The epidemiologic distribution of these injuries is classically bimodal. The vast majority of proximal humerus fractures occur in older individuals, particularly females, with a female-to-male ratio of 2:1. In this demographic, a proximal humerus fracture sustained following a low-energy mechanism—most commonly a fall onto an outstretched hand (FOOSH) from a standing height—is definitively categorized as a fragility fracture. This classification necessitates not only orthopedic management of the acute injury but also a comprehensive secondary prevention strategy for underlying osteoporosis.
Conversely, younger patients typically sustain proximal humeral fractures secondary to high-energy trauma, such as motor vehicle collisions, falls from significant heights, or high-velocity athletic injuries. These high-energy mechanisms frequently result in more complex fracture patterns, profound soft tissue disruption, fracture-dislocations, and a higher incidence of concomitant polytrauma.
Despite the profound impact of these injuries, it is critical to note that approximately 85% of proximal humerus fractures are minimally displaced or nondisplaced. These stable injury patterns are highly amenable to non-operative management, yielding predictably favorable functional outcomes when appropriate rehabilitation protocols are instituted. However, the management of the remaining 15%—comprising complex, displaced, and unstable fracture patterns—remains one of the most debated and challenging domains in orthopedic trauma surgery.
Surgical Anatomy and Biomechanics
A profound understanding of the complex osseous geometry, dynamic muscular forces, and precarious neurovascular supply of the proximal humerus is the foundation of successful surgical intervention and complication mitigation.
Osteology and Articular Geometry
The shoulder joint possesses the greatest range of motion of any articulation in the human body. This extreme mobility is achieved at the expense of inherent osseous stability. The glenohumeral articulation is characterized by a marked mismatch in articular surface area; the shallow glenoid fossa accommodates only 25% to 30% of the humeral head at any given time. Consequently, glenohumeral stability is primarily dependent on the dynamic and static soft tissue envelope, comprising the capsulolabral complex, glenohumeral ligaments, and the rotator cuff musculature.

The proximal humerus itself exhibits a highly specific spatial orientation. The articular surface of the humeral head is retroverted approximately 35 to 40 degrees relative to the transepicondylar axis of the distal humerus. The neck-shaft angle typically measures between 130 and 140 degrees. Restoration of these anatomic parameters during operative fixation or arthroplasty is critical for optimizing postoperative kinematics and preventing impingement.
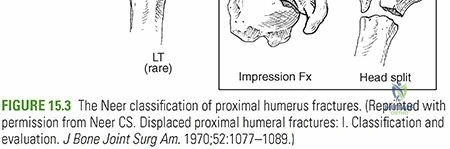
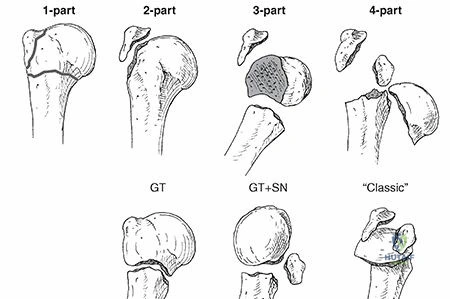
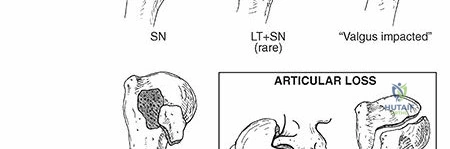
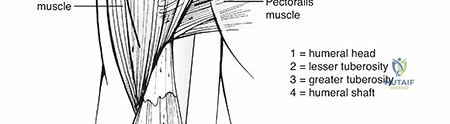
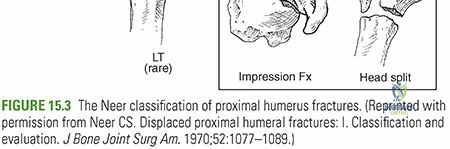
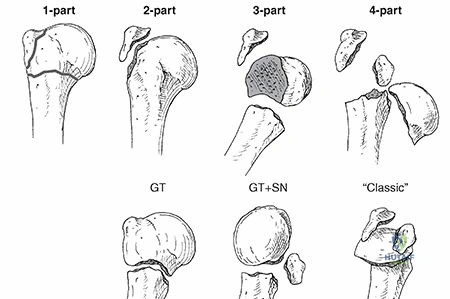
Based on the seminal work of Codman and later refined by Neer, the proximal humerus is conceptualized as four distinct osseous segments, which are separated by the epiphyseal lines. These segments dictate the classification and predictable displacement patterns of proximal humerus fractures:
1. The Humeral Head (articular segment)
2. The Lesser Tuberosity
3. The Greater Tuberosity
4. The Humeral Shaft
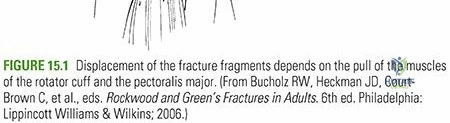
Muscular Deforming Forces
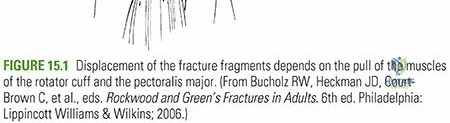
When a fracture disrupts the continuity of the proximal humerus, the attached musculature exerts predictable deforming forces on the isolated segments. Recognizing these vectors is essential for executing closed or open reduction maneuvers.
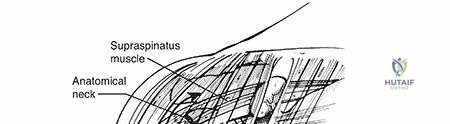
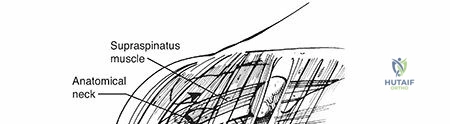
- Greater Tuberosity: The supraspinatus, infraspinatus, and teres minor act in concert to displace an isolated greater tuberosity fragment superiorly and posteriorly. This displacement rapidly leads to subacromial impingement and profound loss of active elevation and external rotation if left unreduced.
- Lesser Tuberosity: The subscapularis tendon inserts on the lesser tuberosity, exerting a strong medial pull. An isolated lesser tuberosity fracture is often associated with posterior shoulder dislocations.
- Humeral Shaft: The pectoralis major, inserting on the lateral lip of the bicipital groove, acts as a powerful deforming force, pulling the humeral shaft medially and anteriorly.
- Proximal Fragment: The deltoid muscle exerts an abduction force on the proximal articular segment, contributing to the classic varus apex-anterolateral deformity seen in surgical neck fractures.
Neurovascular Anatomy
The vascular supply to the humeral head is a critical determinant of fracture healing and the risk of post-traumatic avascular necrosis (AVN). Historically, the anterior humeral circumflex artery (AHCA) and its ascending branch (the arcuate artery), which courses superiorly within the bicipital groove, were considered the dominant blood supply to the humeral head.
However, contemporary quantitative perfusion studies have paradigm-shifted this understanding, demonstrating that the posterior humeral circumflex artery (PHCA) provides the majority (up to 64%) of the blood supply to the humeral head via rich intraosseous anastomoses. The PHCA reaches the head via tendo-osseous vessels penetrating the posterior rotator cuff insertions. Fractures traversing the anatomic neck severely disrupt this delicate intraosseous network, portending a high risk of ischemic necrosis.
Neurologically, the axillary nerve is the structure at greatest risk during both the initial trauma and subsequent surgical approaches. Originating from the posterior cord of the brachial plexus, it courses anteroinferior to the glenohumeral joint capsule before passing through the quadrangular space. Its relatively rigid tethering at the posterior cord and the deltoid fascia, combined with its proximity to the inferior capsule, renders it highly susceptible to traction neuropraxia during anterior fracture-dislocations or aggressive surgical retraction.
Indications and Contraindications
The decision-making process for proximal humerus fractures is complex, heavily influenced by patient-specific factors (age, functional demand, bone quality, medical comorbidities) and fracture morphology. The Neer classification system remains the most widely utilized framework, defining "parts" not by the mere presence of fracture lines, but by displacement (greater than 1 cm) or angulation (greater than 45 degrees) of the four osseous segments.
| Management Strategy | Primary Indications | Relative Contraindications |
|---|---|---|
| Non-Operative | Minimally displaced 1-part fractures; Non-ambulatory patients; Severe dementia; High perioperative mortality risk. | Open fractures; Polytrauma; Neurovascular compromise. |
| ORIF (Plating/Nailing) | Displaced 2-part and 3-part fractures; Greater tuberosity displacement >5mm in active patients; Valgus-impacted 4-part fractures (in younger patients). | Severe osteopenia precluding screw purchase; Head-splitting fractures in elderly; Fixed glenohumeral arthritis. |
| Hemiarthroplasty | 4-part fractures in younger/middle-aged patients; Head-splitting fractures; Anatomic neck fractures with high AVN risk (intact cuff required). | Rotator cuff arthropathy; Severe tuberosity comminution precluding healing; Elderly low-demand patients. |
| Reverse Total Shoulder (RTSA) | Elderly patients with complex 3- or 4-part fractures; Pre-existing rotator cuff arthropathy; Fracture-dislocations in osteoporotic bone. | Active infection; Axillary nerve palsy/deltoid dysfunction; Young, high-demand laborers. |
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is essential for anticipating intraoperative challenges, selecting the appropriate implant, and optimizing patient outcomes.
Radiographic Evaluation
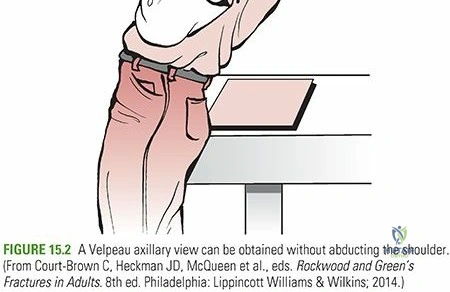
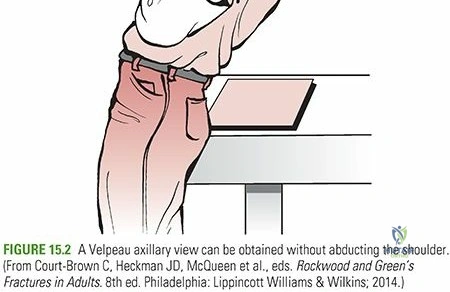
The standard trauma series for the shoulder must include a True Anteroposterior (Grashey) view, a Scapular Y view, and an Axillary lateral view. The axillary lateral is non-negotiable; it is the definitive view for assessing glenohumeral concentric reduction, ruling out subtle posterior dislocations, and evaluating the degree of tuberosity displacement. In cases where pain precludes a standard axillary view, a Velpeau axillary view can be obtained with the patient remaining in the sling.
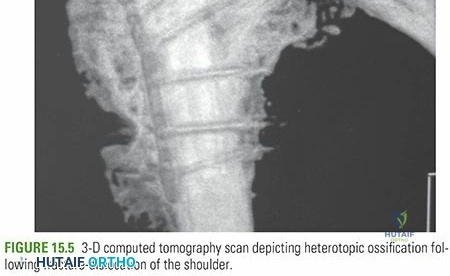
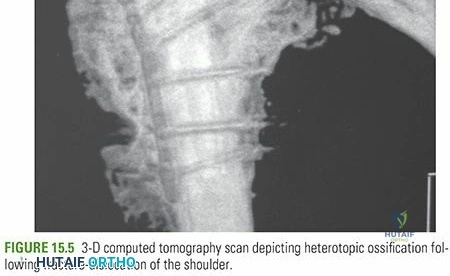
For all complex fracture patterns (displaced 2-part, 3-part, and 4-part fractures), a non-contrast Computed Tomography (CT) scan with 3-dimensional reconstructions is strongly recommended. CT imaging allows for precise spatial localization of the tuberosity fragments, assessment of articular surface involvement (head-splitting components), and evaluation of the medial calcar hinge, which is a critical prognosticator for post-traumatic AVN and structural stability.
Positioning and Setup
Surgical intervention for proximal humerus fractures is typically performed with the patient in the beach chair (semi-fowler) position. The torso is elevated 30 to 45 degrees, and the patient is shifted laterally so the operative shoulder extends completely off the edge of the table, allowing unimpeded extension of the arm.
A radiolucent table or specialized beach chair attachment is mandatory to facilitate unobstructed intraoperative fluoroscopy. The C-arm is typically brought in from the head of the bed or the contralateral side. The surgeon must verify that perfect AP and axillary fluoroscopic images can be obtained prior to sterile draping. The arm is draped free to allow full manipulation, which is critical for reduction maneuvers.
Detailed Surgical Approach and Technique
The choice of surgical approach dictates the visualization of the fracture fragments and the trajectory of internal fixation. The two primary approaches utilized are the deltopectoral approach and the anterolateral deltoid-splitting approach.

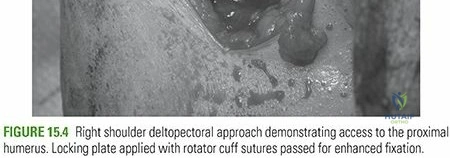
The Deltopectoral Approach
The deltopectoral approach is the workhorse extensile exposure for proximal humerus trauma, offering excellent visualization of the anterior and medial structures and facilitating conversion to arthroplasty if necessary.
- Incision and Superficial Dissection: The incision extends from the tip of the coracoid process distally toward the deltoid tuberosity, following the deltopectoral groove.
- Internervous Plane: The approach utilizes the true internervous plane between the deltoid (axillary nerve) and the pectoralis major (medial and lateral pectoral nerves).
- Cephalic Vein Management: The cephalic vein is identified within the groove. It is typically retracted laterally with the deltoid to preserve its dominant venous tributaries, though medial retraction is acceptable if dictated by the venous anatomy.
- Deep Dissection: The clavipectoral fascia is incised lateral to the conjoint tendon. The conjoint tendon (short head of the biceps and coracobrachialis) is retracted medially. The subdeltoid and subacromial spaces are bluntly developed to mobilize the proximal fragment.
- Biceps Tendon Identification: The long head of the biceps tendon is a critical anatomical landmark, serving as the demarcation between the greater and lesser tuberosities. It is often tenodesed to the pectoralis major or tenotomized in older patients to prevent post-operative bicipital tenosynovitis.
The Anterolateral Deltoid Splitting Approach
The anterolateral approach provides direct orthogonal access to the greater tuberosity and lateral aspect of the humeral head, making it highly advantageous for isolated greater tuberosity fractures or valgus-impacted patterns requiring lateral plate application.
- Incision: A longitudinal incision is made starting at the anterolateral corner of the acromion, extending distally for approximately 5 cm.
- Deltoid Split: The anterior and middle thirds of the deltoid are split bluntly in line with their fibers.
- Axillary Nerve Protection: The critical limitation of this approach is the axillary nerve, which crosses the operative field transversely on the deep surface of the deltoid, approximately 5 to 7 cm distal to the lateral acromial edge. The split must not extend beyond 5 cm to avoid iatrogenic denervation of the anterior deltoid. If distal extension is required for plate fixation, a second small incision is made distal to the nerve, and the plate is slid submuscularly beneath the axillary nerve.
Reduction and Fixation Strategies
Anatomic reduction of the tuberosities and restoration of the medial calcar hinge are the cornerstones of successful Open Reduction and Internal Fixation (ORIF).
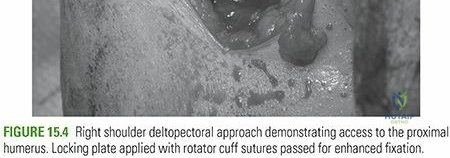
Heavy, non-absorbable traction sutures (e.g., #5 FiberWire) are placed through the bone-tendon junction of the supraspinatus, infraspinatus, and subscapularis. These sutures act as "joysticks" to mobilize the tuberosity fragments out of their retracted positions and are later tied through the plate to neutralize the muscular deforming forces.
The articular segment is elevated and reduced to the humeral shaft. In osteoporotic bone with significant metaphyseal void or medial comminution, an intramedullary fibular strut allograft or structural cancellous bone graft should be utilized. This graft acts as a biologic dowel, providing critical medial support to prevent varus collapse.
Fixation is typically achieved with a Proximal Humeral Locking Plate (PHILOS). The plate is positioned lateral to the bicipital groove and approximately 5 to 8 mm distal to the superior tip of the greater tuberosity to avoid subacromial impingement during abduction. The insertion of calcar screws—locking screws directed into the inferomedial quadrant of the humeral head—is biomechanically imperative. These screws resist the varus bending moments and significantly reduce the incidence of secondary loss of reduction.
Arthroplasty Considerations
When fracture morphology or bone quality precludes stable internal fixation (e.g., head-splitting fractures, severe osteopenia, anatomical neck fractures with disrupted medial hinge), shoulder arthroplasty is indicated.
Historically, hemiarthroplasty was the procedure of choice. However, outcomes of hemiarthroplasty are notoriously unpredictable and are entirely contingent upon anatomic healing of the tuberosities to the implant shaft. Failure of tuberosity healing results in devastating functional deficits, specifically profound weakness in forward elevation and external rotation.
Consequently, Reverse Total Shoulder Arthroplasty (RTSA) has emerged as the preferred treatment for complex 3- and 4-part proximal humerus fractures in the elderly population. RTSA
Clinical & Radiographic Imaging