Surgical Management of Proximal Humerus & Clavicle Malunions

Key Takeaway
Malunions of the proximal humerus and clavicle present complex reconstructive challenges. Disruption of normal anatomy limits shoulder range of motion and strength. Successful management requires a deep understanding of deforming muscle forces, advanced preoperative imaging, and meticulous surgical execution. This guide details the biomechanics, clinical evaluation, and step-by-step surgical techniques—including corrective osteotomy and plate fixation—to restore anatomical alignment and optimize functional outcomes in shoulder girdle malunions.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of proximal humerus and clavicle malunions represents one of the most formidable challenges in modern orthopedic shoulder reconstruction. Malunion in the shoulder girdle typically results from inadequate initial operative reduction, secondary loss of fixation, or the nonoperative management of significantly displaced fractures. As the demographic landscape shifts toward an older, more active population, the incidence of osteoporotic proximal humerus fractures has surged, carrying with it a proportional increase in the prevalence of complex malunions. Concurrently, high-energy trauma in younger demographics continues to produce severe clavicular and humeral fractures that, when managed suboptimally, progress to debilitating osseous deformities.
The disruption of the normal anatomical relationships between the tuberosities, the humeral head, the humeral shaft, and the clavicular strut profoundly alters the biomechanical milieu of the shoulder girdle. This disruption is rarely an isolated osseous event; it is almost universally accompanied by severe soft-tissue pathology. Capsular contracture, rotator cuff tearing or retraction, intra-articular adhesions, and potential neurological injury combine to severely limit glenohumeral and scapulothoracic range of motion, drastically decreasing the overall strength and function of the upper extremity. The patient presenting with a chronic malunion typically reports intractable pain, profound weakness, and an inability to perform basic activities of daily living, necessitating highly specialized surgical intervention.
Historically, the management of these complex deformities was fraught with high complication rates and unpredictable functional outcomes. Early attempts at joint-preserving osteotomies often failed due to a lack of understanding of the intricate soft-tissue contractures and the precarious vascular supply to the humeral head. However, advancements in three-dimensional imaging, a deeper understanding of shoulder biomechanics, and the evolution of sophisticated arthroplasty systems—particularly the reverse total shoulder arthroplasty (RTSA)—have revolutionized our reconstructive capabilities. Today, the orthopedic surgeon possesses an extensive armamentarium to address these pathologies, ranging from extra-articular corrective osteotomies with rigid plate fixation to complex arthroplasty with concurrent tuberosity reconstruction.
Despite these technological advancements, the fundamental principles of meticulous preoperative planning, profound anatomical knowledge, and precise surgical execution remain paramount. The surgeon must navigate distorted anatomical landmarks, dense scar tissue, and altered neurovascular relationships. The decision-making process is highly nuanced, requiring a careful assessment of the patient's physiological age, functional demands, bone stock quality, and the chronicity of the malunion. This chapter provides an exhaustive, evidence-based guide to the pathoanatomy, evaluation, and step-by-step surgical management of proximal humerus and clavicle malunions, designed to equip the advanced orthopedic surgeon with the strategies necessary to optimize patient outcomes in these complex scenarios.
Detailed Surgical Anatomy and Biomechanics
Understanding the predictable patterns of displacement in proximal humerus malunions requires a thorough grasp of the deforming muscular forces acting upon the shoulder girdle. Each anatomical segment has specific tendinous insertions that dictate its trajectory when fractured, and these forces become rigidly fixed in the malunited state. The humeral shaft consistently displaces anteromedially due to the powerful pull of the pectoralis major inserting on the lateral lip of the bicipital groove. The proximal articular fragment tends to be abducted by the resting tone of the rotator cuff if the tuberosities remain attached. The greater tuberosity displaces posterosuperiorly due to the combined forces of the supraspinatus, infraspinatus, and teres minor muscles, while the lesser tuberosity displaces medially, driven by the pull of the subscapularis muscle.
These deforming forces result in characteristic deformity patterns that the surgeon must recognize. In two-part surgical neck malunions, fractures frequently heal in varus and anterior angulation. The shaft is pulled anteromedially by the pectoralis major, while the proximal fragment is abducted. Severe deformities in this plane result in a profound loss of forward flexion and abduction due to the altered center of rotation and the mechanical block created by the prominent greater tuberosity. Two-part greater tuberosity malunions are characterized by the tuberosity being drawn posteriorly and superiorly. Healing in this non-anatomical position creates a mechanical block to abduction and external rotation, frequently leading to severe subacromial impingement. A classic, though not strictly pathognomonic, sign of a greater tuberosity malunion is the complete absence of external rotation when the arm is maximally abducted.
Three-part and four-part malunions present even greater biomechanical derangements. In three-part malunions involving the greater tuberosity and surgical neck, the articular head fragment is internally rotated by the intact subscapularis, the shaft displaces anteromedially, and the greater tuberosity migrates posterosuperiorly. This results in severe functional impairment due to the combined loss of abduction and external rotation. Four-part malunions and fracture-dislocations represent the most formidable reconstructive challenges. They are characterized by severe articular incongruity, dense muscular contractures, a high incidence of osteonecrosis (AVN) of the humeral head, and frequent concomitant neurological deficits. The glenohumeral joint is effectively destroyed, and the normal force couples of the rotator cuff are rendered nonfunctional.

In the context of the clavicle, the biomechanics are equally unforgiving. The clavicle acts as the sole osseous strut connecting the axial skeleton to the upper extremity, maintaining the scapula at a constant distance from the sternum. Malunions of the clavicle, particularly those with significant shortening (greater than 1.5 to 2.0 cm) or severe angular deformity, profoundly alter the resting position of the scapula. This results in scapular protraction, anterior tilt, and downward rotation—a condition broadly termed scapular dyskinesia. This altered scapulothoracic articulation drastically reduces the efficiency of the rotator cuff and deltoid, leading to generalized shoulder weakness, early fatigue, and potential thoracic outlet-type symptoms due to the narrowing of the costoclavicular space. Restoration of clavicular length and alignment is therefore not merely a cosmetic endeavor, but a critical requirement for restoring normal shoulder biomechanics.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for a proximal humerus or clavicle malunion must be meticulously tailored to the individual patient. Operative management is rarely indicated for purely radiographic abnormalities; rather, it is driven by the patient's clinical symptoms and functional deficits. The primary indication for surgery is severe, intractable pain that has failed exhaustive conservative management, including targeted physical therapy, nonsteroidal anti-inflammatory medications, and judicious use of corticosteroid injections. A secondary, yet equally compelling indication is a profound functional loss that prevents the patient from performing essential activities of daily living or returning to their required occupational duties.
In the proximal humerus, the specific type of surgical reconstruction—joint-preserving osteotomy versus arthroplasty—depends heavily on the status of the articular cartilage, the viability of the humeral head, and the chronicity of the malunion. Joint-preserving corrective osteotomies are indicated in younger, high-demand patients with intact articular cartilage, a viable humeral head (no evidence of AVN), and a malunion that is amenable to mobilization and rigid internal fixation. Conversely, arthroplasty (hemiarthroplasty, anatomic total shoulder, or reverse total shoulder) is indicated for older patients, those with established osteonecrosis, severe intra-articular incongruity, or massive, irreparable rotator cuff tearing associated with the malunion.
For clavicular malunions, operative intervention is indicated in the presence of symptomatic shortening greater than 1.5 to 2.0 cm, severe angular deformity causing skin compromise or neurovascular impingement (thoracic outlet syndrome), and chronic pain localized to the malunion site combined with demonstratable scapular dyskinesia. Extra-articular corrective osteotomy with rigid plate fixation, often supplemented with structural intercalary bone grafting, is the gold standard for these indications. The surgeon must carefully assess the patient's physiological ability to tolerate a complex reconstructive procedure and a prolonged, demanding postoperative rehabilitation protocol.
| Clinical Parameter | Indications for Surgical Reconstruction | Absolute & Relative Contraindications |
|---|---|---|
| Proximal Humerus | Intractable pain failing >6 months of conservative care; Severe functional deficit (e.g., forward elevation <90°); Symptomatic tuberosity displacement >1cm causing mechanical block; Impending skin breakdown from prominent hardware/bone. | Active glenohumeral or systemic infection (Absolute); Charcot arthropathy (Absolute); Medically unfit for prolonged anesthesia (Absolute); Asymptomatic malunion regardless of radiographic appearance (Relative); Inability to comply with complex rehab (Relative). |
| Clavicle | Symptomatic shortening >1.5-2.0 cm with scapular dyskinesia; Thoracic outlet syndrome secondary to costoclavicular space narrowing; Refractory pain at the malunion site; Severe cosmetic deformity causing psychological distress in a symptomatic patient. | Active local osteomyelitis (Absolute); Severe osteoporosis precluding rigid plate fixation (Relative); Asymptomatic shortening (Relative); Active smokers unwilling to cease tobacco use prior to osteotomy/grafting (Relative). |
| Neurological Status | Compressive neuropathy directly attributable to the osseous deformity that has failed conservative management. | Profound, irreversible brachial plexopathy or isolated axillary nerve palsy (Relative contraindication for anatomic TSA/osteotomy; may require RTSA or arthrodesis as a salvage procedure). |
Pre-Operative Planning, Templating, and Patient Positioning
History, Physical Examination, and Advanced Imaging
A meticulous preoperative evaluation is the cornerstone of successful malunion reconstruction. The surgeon must ascertain the original mechanism of injury, the initial treatment modality (operative vs. nonoperative), and the exact timeline of events. If previous surgery was performed, obtaining the operative notes and determining the specific type of hardware utilized is mandatory to ensure the appropriate extraction equipment (e.g., stripped screw removal kits, specific screwdrivers, metal-cutting burrs) is available in the operating room. Range of motion (ROM) testing must rigorously differentiate between active and passive limits. A severe restriction in passive ROM strongly suggests dense capsular or extracapsular contracture, which will require extensive surgical release.
Because many patients with proximal humeral malunions harbor subclinical neurological deficits, the function of the axillary, suprascapular, and musculocutaneous nerves must be rigorously documented preoperatively. Electromyography (EMG) and nerve conduction studies (NCS) are highly recommended if a deficit is suspected, as preexisting nerve dysfunction significantly alters the surgical plan and postoperative expectations. Advanced imaging is non-negotiable. While a complete trauma series of standard radiographs (True AP, Scapular Y, and Axillary lateral views) provides a baseline, Computed Tomography (CT) with 3D reconstructions is the gold standard. 3D CT clarifies the spatial relationships between the malunited tuberosities, the humeral head, and the shaft, and is essential for evaluating articular congruity, glenoid version, and available bone stock for implant fixation.
Digital Templating and 3D Modeling
Modern reconstruction relies heavily on digital templating. For proximal humerus arthroplasty, templating software allows the surgeon to determine the optimal size and position of the glenoid baseplate, assess the need for bone grafting, and select the appropriate humeral stem size. In cases of severe deformity, patient-specific instrumentation (PSI) or 3D-printed anatomical models can be invaluable. These models allow the surgeon to physically hold the deformed bone, plan the exact trajectory of the osteotomy, and pre-contour fixation plates prior to the incision, significantly reducing intraoperative time and minimizing soft-tissue dissection. For clavicle malunions requiring lengthening, the contralateral normal clavicle should be imaged and used as a template to determine the exact dimensions of the required intercalary structural bone graft.
Patient Positioning and Anesthesia
Patient positioning is critical for optimizing surgical exposure and facilitating intraoperative fluoroscopy. General anesthesia with endotracheal intubation is standard, often supplemented with a regional interscalene nerve block for postoperative analgesia. The patient is typically placed in a beach-chair (semi-sitting) position, with the backrest elevated to approximately 45 to 60 degrees. A small bump or pad is placed behind the ipsilateral medial scapular border to protract the shoulder girdle, bringing the glenohumeral joint and clavicle forward.
The patient's head must be securely secured in a specialized headrest, ensuring the cervical spine remains in a neutral position to prevent iatrogenic brachial plexus traction injuries. The involved upper extremity is tucked into the side using a specialized arm positioner (e.g., a McConnell or Spider arm positioner), allowing it to be draped free for unhindered intraoperative manipulation. If an autogenous structural bone graft from the iliac crest is anticipated for a clavicle reconstruction, the ipsilateral or contralateral iliac crest must be meticulously prepped and draped into the sterile field before the procedure begins.
Step-by-Step Surgical Approach and Fixation Technique
Proximal Humerus Malunion Reconstruction
The surgical approach to the proximal humerus is typically via an extensile deltopectoral incision. The incision begins at the tip of the coracoid process and extends distally along the deltopectoral groove. The cephalic vein is identified and generally retracted laterally with the deltoid muscle to preserve its primary venous drainage, though medial retraction with the pectoralis major is an acceptable alternative depending on the specific venous branching patterns encountered. Deep dissection involves identifying the conjoined tendon and gently retracting it medially. The clavipectoral fascia is incised, exposing the subscapularis and the underlying malunited proximal humerus.
The first critical intraoperative step is the identification and protection of the axillary nerve. The nerve is located by palpating the anterior border of the subscapularis inferiorly, passing anterior to the subscapularis muscle belly and inferior to the glenohumeral joint capsule. A sweeping finger maneuver (the "tug test") can confirm its location. Once protected, the surgeon must address the osseous deformity. If a joint-preserving osteotomy is planned, the malunited tuberosities are carefully osteotomized using sharp, curved osteotomes, taking extreme care to preserve their tendinous attachments. The capsular contractures are systematically released (anterior, inferior, and posterior capsulotomies) to mobilize the joint.
If arthroplasty is indicated (e.g., RTSA for a chronic 4-part malunion in an older patient), the humeral head is resected. The critical challenge in arthroplasty for malunion is the mobilization and secure reattachment of the tuberosities. The greater and lesser tuberosities must be sharply mobilized from the shaft, heavily tagged with non-absorbable heavy sutures (e.g., #5 FiberWire), and meticulously repaired around the arthroplasty implant and to the humeral shaft. Failure to achieve rigid tuberosity fixation will result in catastrophic functional failure, regardless of the implant chosen.
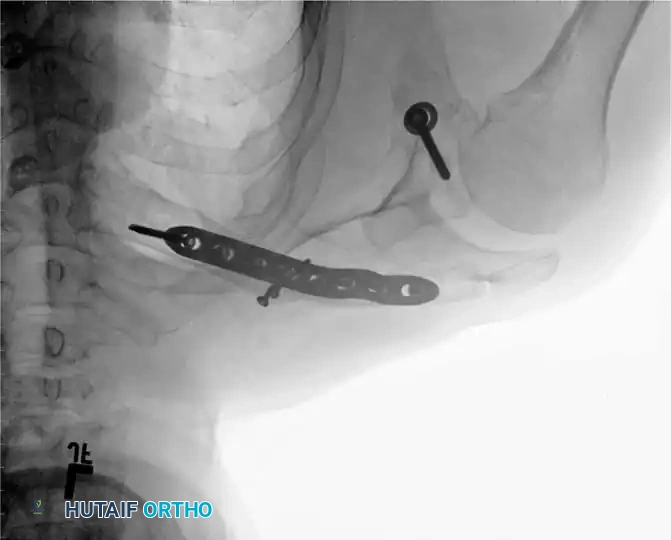
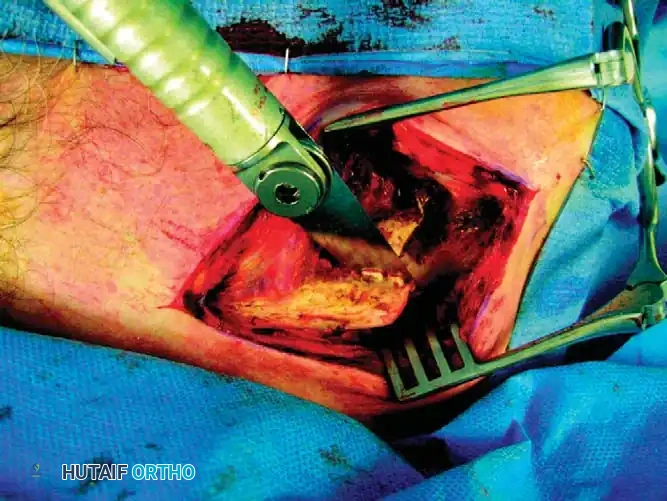
Clavicular Malunion: Osteotomy and Plate Fixation Technique
Associated shoulder girdle malunions—particularly of the clavicle—frequently demand extra-articular corrective osteotomy and rigid plate fixation. Severe shortening alters the resting position of the scapula, leading to scapular dyskinesia and generalized shoulder weakness.
1. Incision and Flap Elevation: Make an oblique incision along the superior surface of the clavicle, following Langer's lines to optimize cosmetic healing. Raise the skin and subcutaneous tissue as a full-thickness flap to identify the underlying platysma and myofascia.
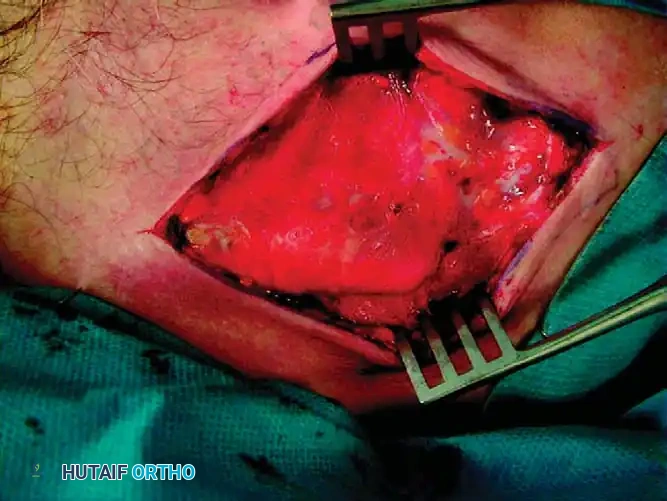
2. Myofascial Preservation: Raise the myofascial layer as contiguous flaps. It is critical to preserve this layer so that a robust, two-layered closure can be achieved over the hardware later. This meticulous soft-tissue handling minimizes the risk of plate prominence, hardware irritation, and devastating wound breakdown over the subcutaneous clavicular border.
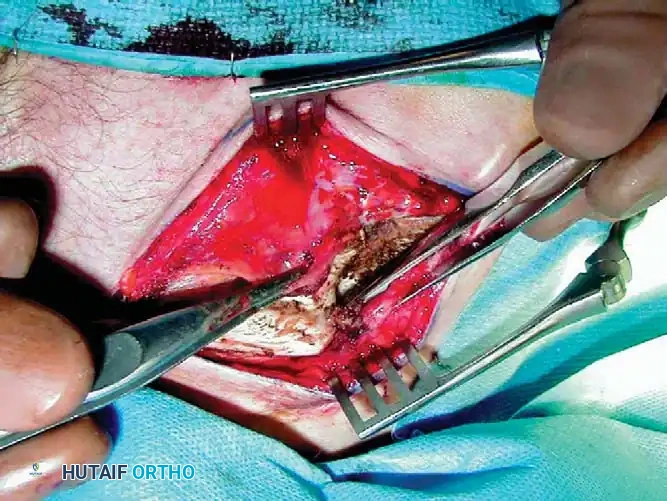
3. Identifying the Malunion: Carefully dissect down to the periosteum to identify the malunion site. Plan the corrective osteotomy. In most cases, the original fracture plane can be identified. In extensively remodeled malunions, an oblique sliding osteotomy or a transverse osteotomy for intercalary grafting may be required.
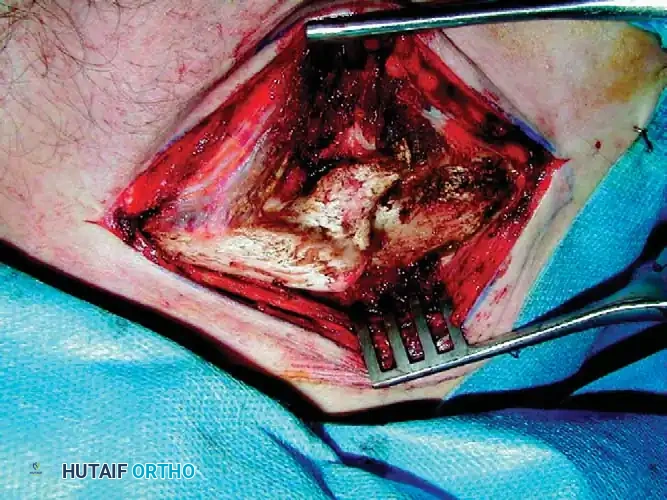
4. Executing the Osteotomy: Use a combination of sharp osteotomes and a microsagittal saw to recreate the original fracture line or execute the planned cut. The saw must be cooled continually with chilled saline irrigation to prevent thermal necrosis of the bone, which could precipitate a nonunion. Crucially, place a malleable retractor deep to the clavicle to protect the underlying subclavian vessels and brachial plexus from catastrophic iatrogenic injury.
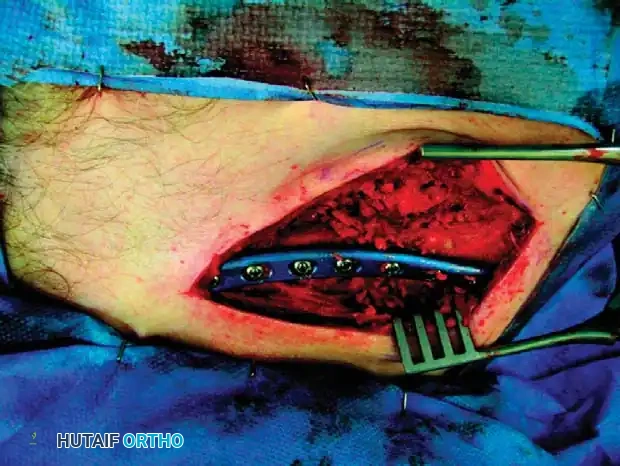
5. Mobilization and Canal Preparation: Hold the proximal and distal fragments with reduction forceps (e.g., pointed Weber clamps). Realign the clavicle, using as little soft-tissue stripping as possible to preserve the vital periosteal blood supply. Reestablish the medullary canal using a 3.5-mm drill bit in both the proximal and distal fragments to encourage endosteal bleeding and stimulate osteogenesis.


6. Correcting Malrotation and Fixation: Rotate the distal fragment anteriorly so that its flat superior surface matches the proximal segment, creating congruent surfaces. Make absolutely no attempt to explore or decompress the brachial plexus deep to the clavicle during this maneuver, as the altered anatomy places these structures at high risk. Once anatomically reduced, provisionally fix the osteotomy with a 2.0-mm Kirschner wire. Apply a pre-contoured superior or anteroinferior locking compression plate (LCP). If an intercalary graft is used, ensure rigid compression across both host-graft interfaces.

Complications, Incidence Rates, and Salvage Management
Surgical reconstruction of proximal humerus and clavicle malunions is technically demanding and carries a significantly higher complication profile than primary fracture fixation. The distorted anatomy, compromised soft-tissue envelope, and frequently osteopenic bone stock create a challenging environment that predisposes the patient to both intraoperative and postoperative adverse events. The surgeon must be acutely aware of these risks, counsel the patient extensively during the preoperative period, and possess the technical expertise to manage complications when they arise.
Intraoperative complications primarily involve iatrogenic neurovascular injury and fracture propagation. In the proximal humerus, the axillary nerve is at highest risk during extensive inferior capsular releases and mobilization of the proximal shaft. In clavicle osteotomies, the subclavian vein and artery, as well as the brachial plexus, lie directly posterior and inferior to the middle third of the clavicle. Penetration of the protective malleable retractor with a drill bit or saw blade can result in catastrophic hemorrhage. Furthermore, aggressive manipulation of osteopenic bone during deformity correction can lead to iatrogenic fracture propagation, necessitating the immediate availability of longer revision plates, cerclage cables, and structural allografts.
Postoperative complications are equally daunting. Nonunion of the osteotomy site or failure of tuberosity healing (in arthroplasty cases) are among the most common causes of functional failure. Tuberosity escape following RTSA for malunion dramatically reduces active forward elevation and external rotation, often resulting in a pseudoparalytic shoulder. Infection, while relatively rare (incidence of 1-3%), is devastating when it occurs in the presence of massive hardware or arthroplasty implants. Avascular necrosis (AVN) of the humeral head following joint-preserving osteotomy is a constant threat, particularly if the ascending branch of the anterior circumflex humeral artery or the posterior circumflex humeral artery are compromised during soft-tissue stripping.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management Protocol |
|---|---|---|---|
| Tuberosity Nonunion / Escape (Post-Arthroplasty) | 15% - 30% | Meticulous heavy suture fixation (#5 FiberWire) through bone tunnels; strict adherence to postoperative immobilization protocols. | Revision fixation if recognized early; if chronic, conversion to RTSA (if not already performed) with latissimus dorsi transfer for external rotation loss. |
| Osteotomy Nonunion (Clavicle or Humerus) | 5% - 10% | Preserve periosteal blood supply; ensure rigid, multi-planar compression plating; utilize autologous bone grafting for large defects. | Revision internal fixation with dual plating (orthogonal), extensive autogenous iliac crest bone grafting, and optimization of metabolic parameters (e.g., Vitamin D, smoking cessation). |
| Avascular Necrosis (Post-Osteotomy) | 10% - 25% | Minimize soft-tissue stripping of the tuberosities; preserve the posteromedial hinge during surgical neck osteotomies. | Conversion to anatomic Total Shoulder Arthroplasty (if cuff intact) or Reverse Total Shoulder Arthroplasty (if cuff deficient/tuberosities severely compromised). |
| Neurological Injury (Axillary or Brachial Plexus) | 2% - 5% | Routine intraoperative identification and protection of the axillary nerve; avoid over-distraction during clavicle lengthening. | Observation and serial EMG/NCS for neuropraxia; early nerve exploration and grafting/transfer if complete disruption is confirmed or no recovery at 3-6 months. |
| Deep Surgical Site Infection | 1% - 3% | Strict sterile technique; meticulous soft-tissue handling and layered closure (myofascial flap over clavicle); prophylactic antibiotics. | Aggressive surgical debridement, implant retention (if stable and early), targeted intravenous antibiotics; two-stage revision arthroplasty for chronic periprosthetic infections. |
Phased Post-Operative Rehabilitation Protocols
The success of a complex malunion reconstruction is as dependent on the postoperative rehabilitation protocol as it is on the surgical execution. The rehabilitation program must strike a delicate, highly individualized balance between protecting the fragile osteotomy or tuberosity repair and preventing the severe joint stiffness that plagues these patients. Communication between the operating surgeon and the physical therapist is absolutely critical; the therapist must be explicitly informed of the bone quality, the rigidity of the fixation, and any specific intraoperative concerns regarding soft-tissue tension.
Phase I: Maximum Protection (Weeks 0 to 6)
Immediately postoperatively, the shoulder is immobilized in a specialized sling or abduction orthosis. The specific position depends on the surgery performed; for example, a greater tuberosity repair may require an abduction sling to minimize tension on the supraspinatus. During this phase, absolute protection of the osseous repair is paramount. Therapy is restricted to passive range of motion (PROM) only, strictly within safe zones determined intraoperatively by the surgeon. Pendulum exercises, passive forward elevation, and gentle external rotation (often limited to neutral or 20 degrees to protect the subscapularis) are initiated. Active motion of the elbow, wrist, and hand is encouraged immediately to prevent distal edema and stiffness.
Phase II: Active-Assisted and Early Active Motion (Weeks 6 to 12)
At approximately 6 weeks, radiographic confirmation of early callus formation or stable hardware positioning is obtained. If satisfactory,
Clinical & Radiographic Imaging Archive



