Step-by-Step Guide: Minimally Invasive Approach to the Proximal Humerus

Key Takeaway
Here are the crucial details you must know about Step-by-Step Guide: Minimally Invasive Approach to the Proximal Humerus. The minimally invasive anterolateral approach to the proximal humerus is a surgical technique for inserting intramedullary nails. It treats acute, pathologic, or nonunion humeral shaft fractures. This approach involves a 2-cm incision from the acromion, splitting the deltoid muscle, and precisely identifying the humeral entry point for optimal fracture stabilization.
Introduction and Epidemiology
This article provides a detailed step-by-step guide to the minimally invasive anterolateral approach to the proximal humerus, specifically tailored for the insertion of intramedullary nails. This technique remains a cornerstone in the surgical management of various humeral shaft pathologies, offering distinct advantages over traditional open plating techniques in appropriately selected cases. The application of intramedullary nailing for humeral shaft fractures represents a significant advancement in orthopedic traumatology, effectively balancing robust mechanical fixation with the critical preservation of the surrounding soft tissue envelope.
The minimally invasive approach is primarily indicated for the treatment of acute humeral shaft fractures, pathologic humeral shaft fractures, and the management of delayed union and nonunion of the humeral diaphysis. Epidemiologically, humeral shaft fractures account for approximately one to three percent of all skeletal fractures. The demographic distribution demonstrates a classic bimodal curve. The first peak occurs in young, active males, predominantly secondary to high-energy trauma such as motor vehicle collisions or significant falls. The second peak is observed in elderly females, typically associated with low-energy ground-level falls superimposed on severe osteopenia or osteoporosis.
While a substantial proportion of isolated humeral shaft fractures can be managed non-operatively with functional bracing (Sarmiento bracing), surgical intervention is increasingly preferred for specific fracture morphologies, polytraumatized patients, or individuals requiring expedited functional rehabilitation. Intramedullary nailing provides a load-sharing construct that maintains coronal and sagittal alignment while permitting early range of motion, thereby mitigating the risk of post-traumatic shoulder and elbow arthrofibrosis.
The evolution of the anterolateral approach reflects a broader paradigm shift in orthopedic surgery towards minimally invasive osteosynthesis. By avoiding extensive periosteal stripping and minimizing disruption to the fracture hematoma, this approach optimizes the biological environment for secondary bone healing via callus formation.
Surgical Anatomy and Biomechanics
Proximal Humeral Anatomy and Articular Considerations
The proximal humerus is a complex anatomical region characterized by the humeral head, anatomical neck, surgical neck, greater tuberosity, and lesser tuberosity. The humeral head, covered entirely by hyaline articular cartilage, articulates with the glenoid fossa of the scapula to form the glenohumeral joint. The extensive articular surface necessitates meticulous consideration of the intramedullary nail entry point to prevent iatrogenic cartilage damage and subsequent degenerative arthropathy.
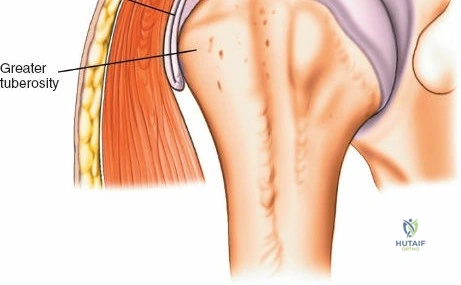
The greater tuberosity serves as the insertion footprint for the supraspinatus, infraspinatus, and teres minor tendons, while the lesser tuberosity receives the subscapularis tendon. These structures collectively form the rotator cuff, which is critical for dynamic shoulder stability and kinematics. The bicipital groove, housing the long head of the biceps tendon, lies anteriorly between the tuberosities and serves as a crucial landmark during surgical orientation.
Musculature and Internervous Planes
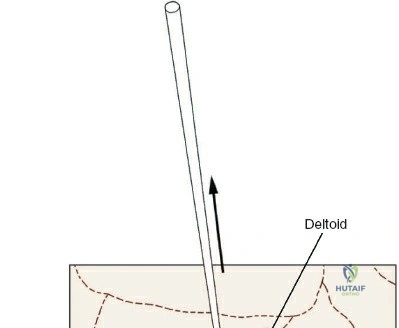
The deltoid muscle envelops the proximal humerus and is innervated exclusively by the axillary nerve. The minimally invasive anterolateral approach typically involves a longitudinal, muscle-splitting dissection of the anterior deltoid fibers. It is paramount to recognize the precise anatomical course of the axillary nerve, which typically traverses transversely across the deep surface of the deltoid, wrapping around the surgical neck of the humerus.
Anatomical studies place the axillary nerve approximately five to seven centimeters distal to the lateral edge of the acromion. Excessive distal dissection or aggressive retraction in this zone risks catastrophic iatrogenic nerve injury. The internervous plane for this specific approach is less formally defined than for traditional open plating (such as the deltopectoral approach), as the primary objective is a restricted, muscle-splitting window solely for the facilitation of intramedullary access and nail insertion.
Neurovascular Structures
Key neurovascular structures in the vicinity of the proximal humerus and humeral shaft include the axillary nerve, radial nerve, musculocutaneous nerve, and the major trunks of the brachial plexus. The axillary nerve is highly vulnerable during proximal humeral approaches and proximal interlocking screw insertion.
The radial nerve courses through the spiral groove on the posterior aspect of the humeral shaft, transitioning from the posterior compartment to the anterior compartment through the lateral intermuscular septum approximately fourteen to sixteen centimeters distal to the greater tuberosity. This anatomical transition makes the radial nerve a critical structure to protect during shaft fixation, particularly during lateral-to-medial distal interlocking screw placement or when manipulating distal fracture fragments. The brachial artery and accompanying veins are situated deep within the medial arm and are generally protected unless there is profound soft tissue trauma, severe medial displacement of fracture fragments, or extensive aberrant dissection.
Biomechanics of Humeral Nailing
Intramedullary nails function as load-sharing implants, stabilizing fractures by providing central mechanical support within the medullary canal. Unlike rigid plate constructs that act as load-bearing devices and rely on absolute stability for primary bone healing, intramedullary nails allow for controlled micromotion at the fracture site. This micromotion is highly osteogenic, promoting robust secondary bone healing via enchondral ossification.
The biomechanical efficacy of a humeral nail is dictated by its working length, radius, and the integrity of the interlocking screws. Antegrade nailing provides superior torsional rigidity compared to unreamed systems, though the decision to ream must be balanced against the risk of thermal necrosis and endosteal vascular disruption. The central position of the nail aligns with the mechanical axis of the humerus, minimizing bending moments and reducing the risk of implant failure compared to eccentrically placed plates.
Indications and Contraindications
The decision to proceed with intramedullary nailing via a minimally invasive anterolateral approach requires careful patient selection, comprehensive radiographic analysis, and a thorough understanding of the fracture morphology. While functional bracing remains the gold standard for many isolated, closed humeral shaft fractures, specific clinical scenarios unequivocally demand surgical stabilization.
Patient Selection Criteria
Polytraumatized patients represent a primary indication for intramedullary nailing. In the setting of multiple injuries, early stabilization of the humerus facilitates upright positioning, nursing care, and the use of the upper extremity for mobilization and transfers. Similarly, bilateral humeral shaft fractures, "floating elbow" variants (ipsilateral humeral and forearm fractures), and fractures associated with major vascular injuries requiring repair are absolute indications for operative intervention.
Pathologic fractures, or impending pathologic fractures based on Mirels' criteria, are exceptionally well-suited for intramedullary nailing. The nail spans the entire diaphysis, protecting the entire structural length of the bone against subsequent metastatic lesions, a distinct advantage over localized plate osteosynthesis.
Contraindications must be strictly observed to prevent catastrophic outcomes. Active local or systemic infection is an absolute contraindication to the insertion of intramedullary hardware. Severe medullary canal stenosis, whether congenital or secondary to previous trauma, may preclude the passage of even the smallest diameter nails. Furthermore, fractures with intra-articular extension into the glenohumeral joint or extremely distal fractures lacking sufficient metaphyseal bone for distal interlocking screw purchase are better managed with alternative fixation strategies, such as open reduction and internal fixation with locking plates.
| Clinical Parameter | Indications for Operative Fixation (IMN/Plating) | Indications for Non-Operative Management (Bracing) |
|---|---|---|
| Fracture Morphology | Segmental fractures, severe displacement, distraction | Acceptable alignment (<20° anterior bowing, <30° varus/valgus, <3cm shortening) |
| Soft Tissue Status | Open fractures, associated vascular injury | Closed fractures with intact skin envelope |
| Patient Profile | Polytrauma, bilateral fractures, floating elbow | Isolated injury, compliant patient |
| Pathology | Pathologic fractures, impending pathologic fractures | Traumatic etiology with adequate bone stock |
| Neurologic Status | Progressive radial nerve palsy after manipulation | Primary radial nerve palsy (expectant management often appropriate) |
Pre Operative Planning and Patient Positioning
Imaging and Templating
Meticulous preoperative planning is the foundation of a successful minimally invasive intramedullary nailing procedure. Standard radiographic evaluation must include orthogonal views of the entire humerus, encompassing both the shoulder and elbow joints. A true anteroposterior (Grashey) view and a Scapular Y view are critical for assessing the proximal extension of the fracture and evaluating the integrity of the greater tuberosity.
If there is any suspicion of occult intra-articular extension or complex proximal comminution, a non-contrast Computed Tomography scan with two-dimensional multiplanar reconstructions and three-dimensional surface rendering should be obtained. Preoperative templating is mandatory to estimate the appropriate nail diameter and length. The contralateral, uninjured humerus can be utilized as a template if bilateral full-length radiographs are available. The surgeon must ensure that the selected nail length allows for adequate distal purchase without impinging on the olecranon fossa.
Operating Room Setup
Patient positioning significantly influences surgical access and the ease of intraoperative fluoroscopy. The procedure is most commonly performed with the patient in the beach chair position, though the supine or lateral decubitus positions are viable alternatives depending on surgeon preference and concurrent injuries.
In the beach chair configuration, the patient's torso is elevated to approximately thirty to forty-five degrees. The operative arm must be completely free-draped to allow for unrestricted manipulation, traction, and multi-planar fluoroscopic imaging. The head is secured in a specialized headrest, ensuring the cervical spine remains in a neutral alignment.
The C-arm fluoroscopy unit is typically positioned parallel to the patient, entering from the contralateral side or superiorly from the head of the bed. The monitor should be placed in the surgeon's direct line of sight. Prior to making the incision, the surgeon must confirm that unobstructed anteroposterior and lateral fluoroscopic views of the entire humerus, from the humeral head to the distal articular surface, can be reliably obtained.
Detailed Surgical Approach and Technique
Incision and Superficial Dissection
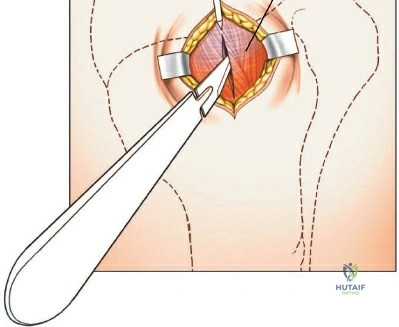
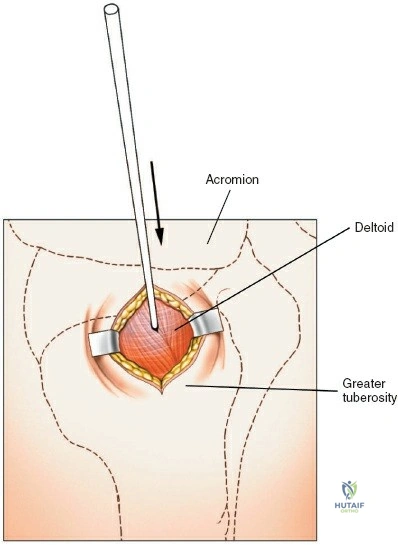
The minimally invasive anterolateral approach begins with precise anatomical landmark identification. The anterolateral tip of the acromion is palpated, and a three to five-centimeter longitudinal incision is made extending distally from this point. Subcutaneous tissues are sharply dissected to expose the underlying deltoid fascia.
The anterior and middle thirds of the deltoid muscle are identified. A longitudinal split is created in the deltoid muscle strictly in line with its fibers. It is imperative to limit the distal extent of this split to a maximum of five centimeters from the acromial edge to absolutely prevent iatrogenic transection of the axillary nerve. A heavy non-absorbable suture can be placed at the distal apex of the split to serve as a physical barrier against inadvertent distal propagation during subsequent retraction and reaming.
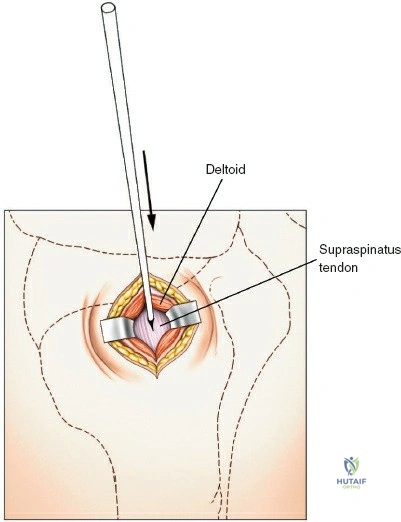
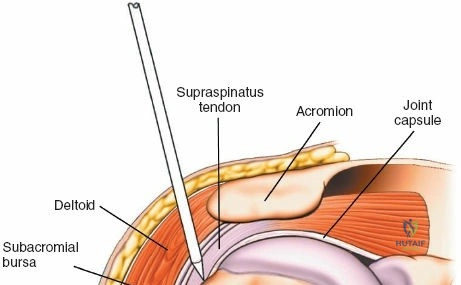
Rotator Cuff Management and Entry Point
Deep to the deltoid, the subdeltoid bursa is excised to expose the underlying rotator cuff. The approach to the intramedullary canal necessitates traversing the rotator cuff. Historically, a longitudinal split through the supraspinatus tendon was utilized; however, modern techniques advocate for an incision through the rotator interval or a highly targeted, minimal incision at the precise insertion footprint to minimize postoperative cuff dysfunction.
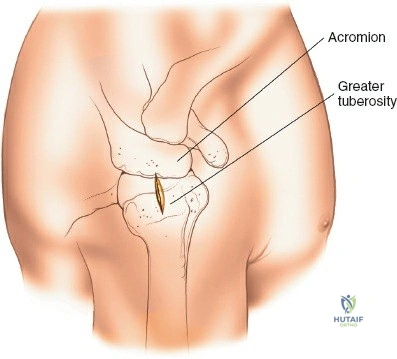
The determination of the exact entry point is the most critical step of the procedure. For straight nails, the entry point is located at the absolute apex of the humeral head, slightly medial to the greater tuberosity and in line with the longitudinal axis of the medullary canal. For modern, anatomically pre-bent nails, the entry point is slightly more lateral, situated directly on the greater tuberosity.
A sharp awl or a threaded guide pin is advanced under biplanar fluoroscopic guidance to breach the proximal cortex. The trajectory must be perfectly aligned with the diaphysis in both the coronal and sagittal planes to prevent eccentric reaming, iatrogenic comminution, or cortical blowout.
Fracture Reduction and Canal Preparation
Once the entry portal is established, a ball-tipped guide wire is introduced and advanced down the medullary canal. Achieving closed reduction of the humeral shaft fracture is necessary to allow passage of the guide wire into the distal fragment. Reduction is typically achieved through a combination of longitudinal traction, manipulation of the distal arm, and the use of percutaneous joysticks or a minimally invasive reduction tool if necessary.
Upon confirming the guide wire is centered within the distal metaphysis via fluoroscopy, the medullary canal is prepared. The decision to ream is multifactorial. Reaming increases the internal diameter of the canal, allowing for the insertion of a larger, biomechanically superior nail. It also generates autologous bone graft that is deposited at the fracture site. However, aggressive reaming must be avoided to prevent thermal necrosis. Reaming is performed sequentially in half-millimeter increments until cortical chatter is appreciated.
Nail Insertion and Interlocking
The selected intramedullary nail is assembled onto the insertion jig and advanced over the guide wire. The nail should be inserted manually with gentle twisting motions; excessive impaction with a mallet should be avoided to prevent iatrogenic fracture propagation. The proximal end of the nail must be countersunk beneath the articular cartilage or the cortical surface of the greater tuberosity to prevent subacromial impingement during shoulder abduction.
Once optimal nail depth and fracture reduction are confirmed, interlocking screws are placed. Proximal interlocking is typically achieved via the targeting jig. Extreme caution must be exercised during the drilling and insertion of proximal screws to avoid injury to the axillary nerve and the ascending branch of the anterior circumflex humeral artery.
Distal interlocking is performed using a freehand "perfect circle" fluoroscopic technique. The radial nerve is at risk during this step, particularly with lateral-to-medial screw trajectories. Many modern nail designs utilize an anterior-to-posterior distal locking option, which significantly reduces the risk of radial nerve injury. Following final fluoroscopic confirmation of hardware placement and fracture alignment, the surgical site is copiously irrigated, the rotator cuff split is meticulously repaired with robust non-absorbable sutures, and the deltoid fascia and skin are closed in layers.
Complications and Management
Despite meticulous surgical technique, the minimally invasive anterolateral approach for humeral nailing carries specific inherent risks. Recognition and prompt management of these complications are vital for optimizing patient outcomes.
Iatrogenic Neurologic Injury
Neurologic complications are among the most devastating adverse events. Axillary nerve palsy can occur due to aggressive distal retraction of the deltoid split or errant placement of proximal interlocking screws. Clinical manifestation includes weakness in shoulder abduction and diminished sensation over the lateral shoulder. Radial nerve palsy is a known risk during distal interlocking, particularly if the drill bit or screw penetrates the posterior or lateral cortex excessively.
If an iatrogenic nerve injury is suspected postoperatively, comprehensive electromyography and nerve conduction studies should be obtained at approximately six weeks if no clinical improvement is observed. Most traction neurapraxias resolve spontaneously with expectant management; however, documented transections require microsurgical exploration and repair or nerve grafting.
Rotator Cuff Pathology and Shoulder Stiffness
Postoperative shoulder pain and stiffness are the most frequently cited drawbacks of antegrade humeral nailing. This morbidity is often multifactorial, stemming from iatrogenic damage to the supraspinatus tendon during entry point creation, prominent proximal hardware causing subacromial impingement, or inadequate postoperative rehabilitation leading to adhesive capsulitis.
Meticulous repair of the rotator cuff defect at the conclusion of the procedure is mandatory. If prominent hardware is identified as the source of persistent pain following fracture union, nail dynamization or complete hardware removal may be indicated. Nonunion and delayed union, while less common with load-sharing intramedullary devices than with rigid plates, can occur, particularly in the setting of atrophic fracture patterns, smoking, or excessive fracture distraction during nail insertion.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Strategy / Management |
|---|---|---|---|
| Shoulder Pain / Impingement | 15% - 30% | Prominent proximal nail, rotator cuff injury at entry point | Aggressive physiotherapy, subacromial injection, hardware removal post-union |
| Iatrogenic Radial Nerve Palsy | 2% - 5% | Errant distal locking screw placement (lateral to medial) | Expectant management (observation), EMG at 6 weeks, nerve exploration if no recovery |
| Iatrogenic Axillary Nerve Palsy | < 2% | Distal deltoid split >5cm, proximal locking screw error | Observation, physical therapy, late nerve reconstruction if permanent |
| Nonunion / Delayed Union | 5% - 10% | Fracture distraction, thermal necrosis from aggressive reaming, smoking | Nail dynamization, exchange nailing with larger diameter, augmentation with bone graft |
| Iatrogenic Fracture Comminution | 3% - 6% | Forceful nail impaction, eccentric entry point, mismatched nail bow | Intraoperative conversion to plate osteosynthesis, cerclage wiring if accessible |
Post Operative Rehabilitation Protocols
Phased Rehabilitation Strategy
The primary objective of postoperative rehabilitation is the rapid restoration of glenohumeral and elbow kinematics without compromising the mechanical integrity of the fracture fixation. The load-sharing nature of the intramedullary nail allows for accelerated rehabilitation compared to non-operative bracing.
Phase I (0 to 2 Weeks Postoperative):
Immediately following surgery, the operative extremity is supported in a standard sling for comfort. Absolute immobilization is discouraged. Starting on postoperative day one, patients are instructed to perform pendulum exercises to prevent dependent edema and early capsular adhesions. Active and active-assisted range of motion of the elbow, wrist, and digits is initiated immediately to prevent distal joint stiffness.
Phase II (2 to 6 Weeks Postoperative):
Upon confirmation of initial soft tissue healing and stable radiographic alignment at the two-week follow-up, the sling is progressively weaned. Active-assisted range of motion of the glenohumeral joint is initiated, focusing on forward elevation in the scapular plane and external rotation. Pulley systems and wand exercises are highly effective during this phase. Active isolated rotator cuff engagement is minimized to protect the surgical repair at the entry site.
Phase III (6 to 12 Weeks Postoperative):
Once radiographic evidence of bridging callus is observed, typically around six to eight weeks, progressive isotonic and isokinetic strengthening exercises are introduced. Emphasis is placed on restoring the dynamic force couples of the rotator cuff and periscapular stabilizers. Full weight-bearing and return to heavy manual labor or high-impact athletics are generally restricted until complete radiographic union is achieved, which typically occurs between three to five months postoperatively.
Summary of Key Literature and Guidelines
Evidence Based Practice
The surgical management of humeral shaft fractures remains a topic of rigorous academic debate, primarily centering on the comparative efficacy of intramedullary nailing versus plate osteosynthesis. A robust body of literature, including several randomized controlled trials and comprehensive meta-analyses, guides current clinical practice.
Landmark studies, such as those by Carroll et al. and Denard et al., have consistently demonstrated that both intramedullary nailing and compression plating yield high rates of fracture union (exceeding ninety percent) for acute humeral shaft fractures. However, the complication profiles differ significantly. Intramedullary nailing is associated with a statistically significant reduction in operative time, intraoperative blood loss, and the incidence of iatrogenic radial nerve palsy compared to open plating.
Conversely, antegrade intramedullary nailing is historically associated with a higher incidence of postoperative shoulder morbidity, specifically decreased range of motion and persistent anterior shoulder pain. This discrepancy has driven the evolution of the minimally invasive anterolateral approach, the refinement of anatomically pre-bent nail designs, and the emphasis on meticulous rotator cuff repair.
Current orthopedic guidelines suggest that while both modalities are acceptable, intramedullary nailing is particularly advantageous for pathologic fractures, segmental fracture patterns, and polytraumatized patients where the minimization of surgical insult is paramount. The decision ultimately relies on a synthesis of fracture morphology, patient physiology, and the precise technical proficiency
