Extensor Reconstruction in Total Knee Arthroplasty: Essential Strategies
Key Takeaway
Discover the latest medical recommendations for Extensor Reconstruction in Total Knee Arthroplasty: Essential Strategies. **Reconstruction in total** for severe knee extensor mechanism disruption is a rare, complex surgical challenge. It's crucial for enabling ambulation and maintaining prosthesis stability. This procedure is complicated by patient factors such as poor skin viability and vascular compromise from prior surgeries. High forces on the knee often lead to failed simple repairs, sometimes making fusion or amputation preferable.
Introduction and Epidemiology
Complete disruption or total dysfunction of the extensor mechanism of the knee is a devastating complication, fortunately occurring in less than 1 percent of all primary and revision total knee arthroplasties. Despite its rarity, the restitution of the extensor mechanism remains arguably the greatest challenge in all of knee surgery. Adequate functioning of the extensor apparatus is an absolute prerequisite not only to enable ambulation and stair climbing but to preserve the dynamic stability of the prosthesis itself. Without a functional extensor mechanism, the knee is rendered unstable, leading to recurrent effusions, profound functional disability, and accelerated wear or failure of the arthroplasty components.
The etiology of extensor mechanism failure is multifactorial, but it is predominantly vascular in origin. While most cases involve some element of acute or repetitive trauma, the underlying insult is frequently iatrogenic. The vast majority of these patients have been the recipients of multiple surgical procedures. Even a successful primary total knee arthroplasty is usually accompanied by a medial parapatellar arthrotomy, extensive fat pad excision, and occasionally a lateral retinacular release. Each of these surgical steps serves to incrementally devascularize the peripatellar tissues.

Each subsequent revision surgery further decreases the blood supply to this critical anatomical zone. The axiom "less is truly more" applies heavily to peripatellar surgery in the revision setting. When disruption occurs, whether at the level of the quadriceps tendon, the patella, or the patellar tendon, simple reconstructive techniques and direct primary repairs are uniformly doomed to failure due to the enormous tension placed on these compromised tissues. Consequently, advanced reconstructive strategies, including structural allografts and synthetic mesh augmentations, are required to restore function.
Surgical Anatomy and Biomechanics
Vascular Anatomy of the Extensor Mechanism
Understanding the vascular supply to the extensor mechanism is critical for the arthroplasty surgeon, as ischemia is the primary driver of tendon attenuation and subsequent rupture. The patella and its tendinous attachments are supplied by an anastomotic ring fed by the genicular arteries. The superior medial, superior lateral, inferior medial, and inferior lateral genicular arteries form the extraosseous arterial ring.
During a standard medial parapatellar arthrotomy, the blood supply from the superior and inferior medial genicular arteries is disrupted. Excision of the infrapatellar fat pad further compromises the inferior vascular contributions. If a lateral retinacular release is performed to improve patellar tracking, the superior lateral genicular artery—often the dominant remaining blood supply to the patella—is severed. This profound devascularization leads to avascular necrosis of the patella, tendon attenuation, and an exponentially increased risk of catastrophic rupture.

Biomechanical Considerations
The biomechanical demands placed upon the extensor mechanism are immense, explaining why direct primary repair of chronic disruptions yields uniformly dismal results. The quadriceps muscle group acts through the patella, which functions as a fulcrum to increase the moment arm of the extensor mechanism.
The forces visited upon the knee during routine activities of daily living are staggering. During stair climbing and arising from a seated position, the joint reaction forces and the tension transmitted through the patellar tendon often approximate seven to eight times total body weight. Even minimal activities generate substantial force; a lower extremity held in full extension will experience forces equivalent to 1.5 times body weight simply when the patient is moving about in bed. These extreme tensile forces dictate that any reconstructive effort must possess exceptional initial ultimate tensile strength and be protected by rigid immobilization until biologic incorporation or robust scar formation occurs.
Indications and Contraindications
The management of extensor mechanism disruption requires a highly individualized approach. An overall assessment of the patient’s likelihood of success must precede any complex reconstructive surgery.
Patient Selection and Soft Tissue Assessment
In many individuals presenting with this complication, the anterior soft tissue envelope is heavily scarred, thin, or poorly vascularized. Because a bulk whole extensor mechanism allograft will consume significantly more space than the native tissue it is replacing, the viability and compliance of the anterior skin flap are critical to the technical success of the procedure.
Many of these individuals are compromised hosts, suffering from medical comorbidities such as diabetes mellitus, inflammatory arthropathies, or chronic corticosteroid use. The ability of the patient to withstand a substantial operation, and more importantly, to comply with 12 weeks of absolute or relative immobilization, must be carefully considered.

Operative vs Non Operative Management
In certain clinical scenarios, particularly in the multiply revised, infected, or severely medically compromised patient, arthrodesis or transfemoral amputation may be preferable to the heroics of a revision total knee arthroplasty combined with an extensor allograft insertion.
| Clinical Scenario | Recommended Management Strategy | Rationale and Considerations |
|---|---|---|
| Acute disruption with robust soft tissue | Primary repair with synthetic augmentation | Rare in TKA; requires pristine tissue quality and strict immobilization. |
| Chronic disruption with viable skin envelope | Whole Extensor Mechanism Allograft or Synthetic Mesh | Gold standard for chronic TKA extensor failure. Requires adequate skin elasticity. |
| Disruption with severe soft tissue compromise | Soft tissue expansion or Flap coverage prior to reconstruction | Gastrocnemius rotation flap may be required to provide vascularized coverage. |
| Active periprosthetic joint infection | Two stage revision with static spacer | Infection must be eradicated before any permanent extensor reconstruction. |
| Multiply revised knee with massive bone loss | Knee Arthrodesis | Provides a stable, painless limb for ambulation when reconstruction is futile. |
| Non ambulatory patient or severe vascular disease | Non operative bracing or Amputation | Heroic surgery is contraindicated if the patient cannot participate in rehabilitation. |
Pre Operative Planning and Patient Positioning
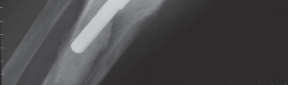
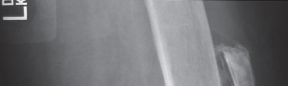
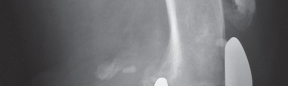
Thorough preoperative planning is mandatory to optimize outcomes and minimize intraoperative complications. The surgeon must obtain orthogonal radiographs of the affected knee to assess the status of the arthroplasty components. Component loosening, severe osteolysis, or malpositioning must be addressed concurrently with the extensor mechanism reconstruction.
Graft Selection and Sizing
If a Whole Extensor Mechanism Allograft is selected, the graft must be ordered well in advance. The allograft consists of the tibial tubercle, patellar tendon, patella, and quadriceps tendon from a cadaveric donor. The surgeon must specify a right or left knee to match the native anatomy, particularly regarding the contour of the tibial tubercle and the patellar articular surface. Alternatively, synthetic mesh reconstruction using heavy monofilament polypropylene or similar materials has gained significant traction due to the avoidance of disease transmission, elimination of allograft supply constraints, and reduced bulk beneath compromised skin flaps.
Patient Positioning
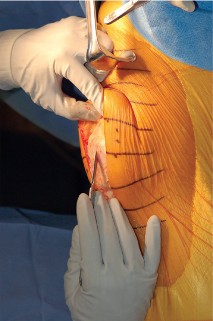
The patient is positioned supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to prevent external rotation of the limb, ensuring the patella points directly anteriorly. A sterile tourniquet is applied to the proximal thigh, although its use should be minimized to preserve vascularity to the skin flaps. The entire lower extremity is prepped and draped free to allow full range of motion during the procedure and to assess extensor mechanism tensioning accurately.
Detailed Surgical Approach and Technique
The surgical technique for extensor mechanism reconstruction demands meticulous soft tissue handling, rigid osseous fixation, and precise tensioning.
Approach and Exposure
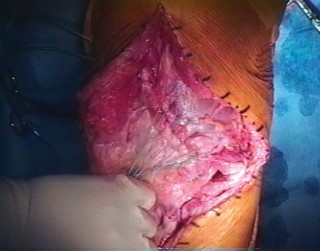
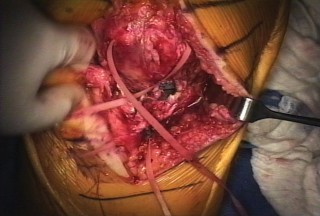
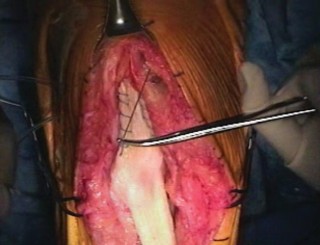
The previous midline longitudinal incision is utilized. Full-thickness fasciocutaneous flaps must be raised to preserve the subdermal vascular plexus. Subcutaneous dissection is strictly avoided to prevent skin flap necrosis. The arthrotomy is typically performed through the previous medial parapatellar approach.
The joint is thoroughly debrided of all fibrotic scar tissue, and the arthroplasty components are inspected. If the components are well-fixed and appropriately positioned, they are retained. The native, dysfunctional patella is typically excised, taking care to preserve the medial and lateral retinacular tissues for later closure and graft coverage. The native quadriceps tendon is identified, mobilized, and prepared to receive the proximal aspect of the reconstruction.
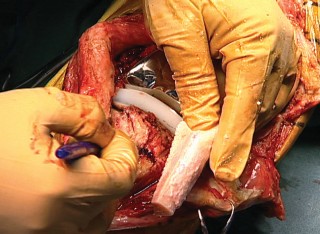
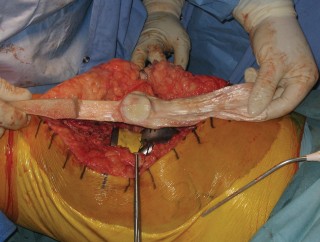
Allograft Preparation
When utilizing a Whole Extensor Mechanism Allograft, the graft is thawed in warm saline containing broad-spectrum antibiotics. The tibial bone block is meticulously shaped using an oscillating saw and a high-speed burr. A standard bone block configuration is approximately 2 to 3 centimeters in length, 1.5 centimeters in width, and 1.5 centimeters in depth.

The edges of the bone block are chamfered to reduce stress risers and to facilitate a press-fit insertion into the host tibia. Heavy non-absorbable cerclage wires or cables are passed through pre-drilled holes in the allograft bone block prior to insertion.
Tibial Host Bed Preparation and Fixation
A corresponding trough is created in the host anterior tibia, slightly medial to the native tibial tubercle to optimize the Q-angle. The trough is undersized by 1 to 2 millimeters to ensure a rigid press-fit of the allograft bone block.
The allograft bone block is impacted into the host trough. Fixation is achieved using the previously placed cerclage wires or cables, which are passed around the proximal tibia or through transverse drill holes in the tibial metaphysis. Supplemental fixation with anterior-to-posterior cortical screws can be utilized to enhance rotational stability and resist the massive pull-out forces generated during knee flexion.
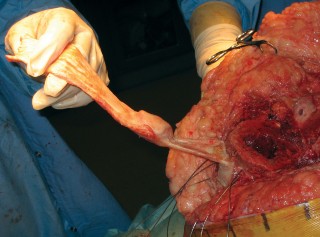
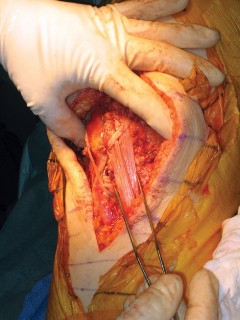
Proximal Tensioning and Fixation
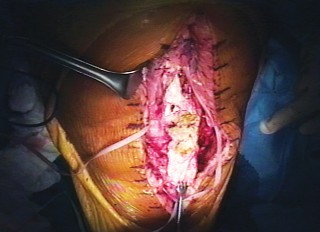
The most critical step of the procedure is the proximal tensioning of the graft. The knee must be placed in full, rigid extension. The allograft quadriceps tendon is draped over the host quadriceps tendon.

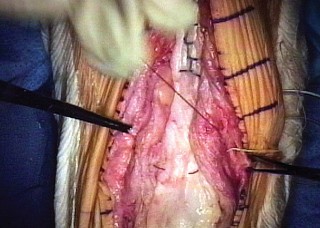
The reconstruction must be tensioned maximally. A common technical error is under-tensioning the graft, which inevitably leads to a profound postoperative extensor lag. Heavy, non-absorbable sutures (such as #5 or #2 ultra-high-molecular-weight polyethylene) are used to weave the allograft and host quadriceps tendons together using a Krackow or similar locking stitch technique. The graft should be tensioned such that the reconstructed patella sits at the appropriate joint line level, avoiding patella baja or alta.
If a synthetic mesh is utilized instead of an allograft, the mesh is secured to the proximal tibia using cementation into a prepared trough or via heavy suture anchors. The mesh is then passed through the host patellar tendon remnants, over the patella, and woven into the host quadriceps tendon under maximal tension with the knee in full extension.
Complications and Management
The complication profile for extensor mechanism reconstruction in the setting of total knee arthroplasty is substantial. Surgeons must counsel patients extensively regarding the high likelihood of postoperative complications, graft attenuation, and the potential need for further surgical intervention.
Extensor Lag and Graft Failure
The most common complication is the development of a postoperative extensor lag. Over time, the allograft tissue or the host-graft interface tends to stretch under the immense biomechanical loads of weight-bearing.
While a mild lag (less than 10 to 15 degrees) is generally well-tolerated and compatible with community ambulation, a progressive or severe lag indicates graft failure. Management of graft failure depends on the patient's functional deficit. Revision reconstruction with synthetic mesh is often the preferred salvage pathway, as repeat allografting carries diminishing returns.
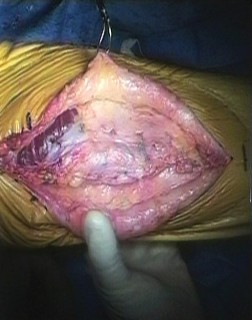
Soft Tissue Necrosis and Infection
Given the compromised nature of the vascular supply and the added bulk of the allograft, wound healing complications are frequent. Skin necrosis over the anterior aspect of the knee can rapidly lead to deep periprosthetic joint infection or graft exposure.
Aggressive management is required for any wound breakdown. This includes prompt surgical debridement and, frequently, the mobilization of a medial or lateral gastrocnemius rotational flap to provide robust, vascularized soft tissue coverage over the reconstruction.
Summary of Complications
| Complication | Estimated Incidence | Prevention and Management Strategies |
|---|---|---|
| Extensor Lag (>15 degrees) | 30% - 50% | Maximize intraoperative tension in full extension; strict adherence to 12-week immobilization. Salvage: Brace or revision reconstruction. |
| Deep Infection | 5% - 10% | Meticulous soft tissue handling; optimize host medical status. Salvage: Two-stage revision, potential arthrodesis. |
| Skin Flap Necrosis | 10% - 15% | Avoid subcutaneous dissection; use full-thickness flaps. Salvage: Gastrocnemius rotation flap. |
| Tibial Bone Block Avulsion | < 5% | Rigid press-fit fixation; multi-planar wire/screw constructs. Salvage: Revision fixation with synthetic augmentation. |
| Arthrofibrosis | 15% - 20% | Expected trade-off for stability. Accept limited flexion (90-100 degrees) to maintain extension power. |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is as critical to the success of the procedure as the surgical technique itself. The reconstructed extensor mechanism relies entirely on mechanical fixation until biologic incorporation or robust fibrotic scar tissue formation occurs.

Following surgery, absolute or relative immobilization is mandatory. The operative limb is placed in a cylinder cast or a rigid, locked hinged knee brace in full extension. The patient is typically permitted to weight-bear as tolerated with the knee locked in extension, as the axial load transmitted through an extended knee does not place undue tensile stress on the extensor reconstruction.
This period of immobilization must be maintained for a minimum of 8 to 12 weeks. Premature initiation of knee flexion is the primary cause of early graft elongation and failure. After the 12-week mark, active and active-assisted knee flexion is initiated in a highly controlled, graduated manner. Flexion is typically advanced by 10 to 15 degrees per week. The ultimate goal of rehabilitation is not to achieve normal knee kinematics, but rather to obtain a stable, brace-free limb capable of full active extension and approximately 90 to 100 degrees of flexion to allow for sitting and stair navigation.
Summary of Key Literature and Guidelines
The literature surrounding extensor mechanism reconstruction underscores the difficulty of the problem and the evolution of surgical techniques. Early attempts at primary repair of tendon disruptions in the setting of total knee arthroplasty yielded uniformly poor outcomes. As noted in foundational studies, simple reconstructive techniques are doomed to failure by the enormous tension placed on the tissues.

The introduction of the Whole Extensor Mechanism Allograft provided the first reliable salvage option. However, long-term follow-up studies have demonstrated a high rate of progressive extensor lag and allograft attenuation over time.
More recently, the use of synthetic mesh (such as Marlex or heavy polypropylene) has emerged as a highly viable, and arguably superior, alternative to allograft reconstruction. Literature comparing the two techniques suggests that synthetic mesh reconstruction provides equivalent or superior restoration of active extension, with a lower profile that is better tolerated by compromised anterior soft tissue envelopes. Furthermore, synthetic mesh does not rely on biologic incorporation, making it highly advantageous in the multiply revised, poorly vascularized knee.
Ultimately, regardless of the material utilized, the principles of extensor reconstruction remain absolute: respect the soft tissue envelope, achieve rigid osseous fixation, tension the graft maximally in full extension, and protect the reconstruction with prolonged postoperative immobilization. Adherence to these essential strategies provides the highest probability of restoring stability and function to the catastrophically failed total knee arthroplasty.
You Might Also Like


