Solving Severe Acetabular Bone Loss with Cup-Cage Reconstruction

Key Takeaway
Discover the latest medical recommendations for Solving Severe Acetabular Bone Loss with Cup-Cage Reconstruction. Acetabular bone loss, often due to aseptic loosening of hip implants, manifests as acute groin pain and inability to weight bear. Radiological assessment typically reveals severe osteolysis of the ilium and ischium. Diagnosis centers on the extent of acetabular bone loss. Treatment, such as cup-cage reconstruction, aims to address significant defects and restore stability in complex revision total hip arthroplasty cases.
Introduction and Epidemiology
Severe acetabular bone loss represents one of the most formidable challenges in revision total hip arthroplasty. This complex clinical scenario is often encountered in cases of failed previous reconstructions, periprosthetic joint infection, extensive osteolysis, tumor resections, or significant trauma. The etiology is multifactorial, frequently stemming from aseptic loosening, septic loosening, component migration, or osteolysis secondary to polyethylene wear.
The classification of acetabular bone loss is critical for surgical planning. The Paprosky classification is widely adopted, categorizing defects based on the integrity of the host bone and the direction of component migration.
* Type 1: Minimal loss, intact rim and columns.
* Type 2A: Mild superior migration, intact columns, deficient superior dome.
* Type 2B: Moderate superior migration, intact columns, deficient superior dome and medial wall.
* Type 2C: Medial migration with intact columns.
* Type 3A: Severe superior migration, compromise of ischial tuberosity and posterior column, often with cavitary and segmental defects.
* Type 3B: Extensive superior and medial migration, complete loss of the posterior column and superior dome, often with pelvic discontinuity.
The American Academy of Orthopaedic Surgeons classification also delineates defects based on morphology, including cavitary, segmental, combined, protrusio, and pelvic discontinuity. Severe bone loss, particularly Paprosky Type 3A and 3B defects, frequently necessitates reconstruction techniques that go beyond conventional cementless hemispheric components with augments. Historically, structural allografts and isolated anti-protrusio cages were utilized; however, these demonstrated high long-term failure rates due to graft resorption and mechanical fatigue failure of the cages in the absence of biologic fixation.
The cup-cage construct, utilizing a cemented polyethylene liner within a metal cage that bridges a highly porous primary acetabular shell, has emerged as a robust solution for these challenging cases. This reconstructive strategy aims to achieve immediate mechanical stability, bridge critical bone defects, and provide a stable environment for potential host bone ingrowth into the porous shell, thereby restoring hip biomechanics and function. The increasing prevalence of revision total hip arthroplasty in an aging population underscores the importance of mastering these complex reconstructive techniques.
Surgical Anatomy and Biomechanics
Pelvic Ring and Acetabular Anatomy
A thorough understanding of pelvic anatomy and biomechanics is paramount for successful acetabular reconstruction. The acetabulum is formed by the fusion of the ilium, ischium, and pubis, creating a hemispheric socket. Key anatomical landmarks dictate the safe zones for hardware placement and the structural integrity of the reconstruction.

The anterior column extends from the anterior superior iliac spine through the anterior acetabulum to the pubic symphysis. The posterior column runs from the posterior ilium through the sciatic notch and posterior acetabulum to the ischial tuberosity. Radiographic landmarks such as the teardrop, Kohler line, and the ilioischial line are vital for assessing the degree of medialization and column integrity. The quadrilateral surface, a thin bony plate located between the anterior and posterior columns, is frequently compromised in severe medial migration. The ischial tuberosity serves as a critical posterior-inferior fixation point for the inferior flange of the cage.
Biomechanical Principles of Cup Cage Constructs
The pelvis functions as a complex ring structure, transferring axial loads from the spine through the sacroiliac joints to the lower extremities. The acetabulum typically supports approximately four to six times body weight during single-limb stance. In severe bone loss, particularly with pelvic discontinuity where the superior hemipelvis is mechanically separated from the inferior hemipelvis, this load transfer mechanism is catastrophically compromised.

The cup-cage construct addresses these biomechanical challenges by effectively transferring axial loads across the discontinuity to the intact ilium and ischium. The highly porous metal cup (typically fabricated from trabecular metal or highly porous titanium) is impacted into the remaining host bone. This component relies on a high coefficient of friction for initial scratch fit and its high porosity for subsequent osteointegration. However, in Paprosky 3B defects or pelvic discontinuity, the cup alone lacks sufficient initial mechanical stability due to inadequate host bone contact (often less than 50 percent).
The addition of the cage provides a rigid, load-sharing exoskeleton. The cage bridges the defect, securing to the viable ilium superiorly and the ischium inferiorly. This "belt and suspenders" approach unloads the porous cup, protecting it from micromotion and shear forces during the critical early postoperative period, thereby facilitating biologic ingrowth. Once osteointegration of the cup occurs, the construct transitions from relying purely on the mechanical fixation of the cage to a biologically stable construct, significantly reducing the risk of late fatigue failure of the metal cage.
Indications and Contraindications
Patient Selection Criteria
The decision to proceed with a cup-cage reconstruction requires careful evaluation of the patient's bone stock, physiological status, and the specific geometry of the acetabular defect. This technique is primarily reserved for the most severe manifestations of acetabular bone loss.
Primary indications include Paprosky Type 3A and 3B defects where less than 50 percent of host bone is available for primary cup fixation. It is highly efficacious in the management of chronic pelvic discontinuity, massive uncontained segmental defects, and cases of prior catastrophic failure of anti-protrusio cages or structural allografts. Furthermore, it is a valuable technique in patients with irradiated pelvic bone, where biologic ingrowth potential is diminished, and immediate rigid mechanical fixation is paramount.
Contraindications include active periprosthetic joint infection, which must be managed with a staged approach prior to definitive reconstruction. Severe destruction of the ilium or ischium that precludes adequate screw fixation for the cage flanges represents a technical contraindication; in such instances, custom triflange acetabular components or massive structural allografts may be required.
| Clinical Scenario | Operative Indication for Cup-Cage | Alternative / Non-Operative Management |
|---|---|---|
| Paprosky 3B Defect | High indication. Excellent for bridging massive defects and providing stability. | Custom Triflange Acetabular Component (CTAC) if standard cages cannot achieve fixation. |
| Pelvic Discontinuity | High indication. Cage bridges the discontinuity while porous cup allows healing. | Plating of posterior column + porous cup; or conservative management if medically unfit. |
| Active PJI | Contraindicated. | Two-stage exchange. Placement of antibiotic spacer until infection is eradicated. |
| Paprosky 2A/2B Defect | Relative contraindication (overtreatment). | Jumbo porous cup with or without metallic augments. |
| Inadequate Ischial Bone | Contraindicated. Inferior flange requires solid ischial purchase. | CTAC, or massive structural allograft reconstruction. |
| Medically Unstable Patient | Contraindicated. | Girdlestone resection arthroplasty or chronic suppressive antibiotics if infected. |
Pre Operative Planning and Patient Positioning
Advanced Imaging and Templating
Meticulous preoperative planning is the cornerstone of successful cup-cage reconstruction. Standard radiography must include an anteroposterior pelvis view, an anteroposterior view of the affected hip, and Judet oblique views (iliac and obturator) to assess the integrity of the anterior and posterior columns. The presence of a pelvic discontinuity is often suggested by a visible fracture line through the acetabulum, medial translation of the inferior hemipelvis, or a break in the Kohler line.

Computed tomography with metal artifact reduction sequence is mandatory. Thin-slice CT allows for precise evaluation of bone stock, the location and size of cavitary and segmental defects, and definitive diagnosis of pelvic discontinuity. Three-dimensional CT reconstructions are increasingly utilized to visualize the defect morphology and aid in the selection of cage size and flange length. In highly complex cases, 3D-printed anatomical models can be sterilized and brought into the operating room for intraoperative contouring of the cage, significantly reducing surgical time.
Templating involves estimating the size of the highly porous cup, which is often oversized to maximize contact with the remaining peripheral host bone. The cage is then templated to ensure adequate span from the ilium to the ischium. Surgeons must plan for the necessary augments to fill cavitary defects behind the cup and ensure the correct left or right orientation and flange length of the cage.
Positioning and Setup
Patients are typically positioned in the lateral decubitus position using rigid pelvic supports. Ensure the abdomen is free to allow for venous return and minimize epidural venous engorgement. A beanbag or rigid pegboard system is utilized. The surgical field must be draped widely to allow for an extended approach, often necessitating proximal extension into the ilium or distal extension for an extended trochanteric osteotomy. Fluoroscopy should be available and positioned to allow for intraoperative orthogonal views of the pelvis without compromising the sterile field.
Detailed Surgical Approach and Technique
Surgical Exposure and Debridement
The surgical approach must provide extensile access to the entire acetabulum, the posterior column, the ischium, and the lateral ilium. A posterolateral approach is most commonly employed. In cases of severe proximal femoral deformity, retained well-fixed cemented stems, or the need for enhanced acetabular exposure, an extended trochanteric osteotomy is highly recommended. The extended trochanteric osteotomy mobilizes the abductor mechanism and the proximal femur anteriorly, providing unparalleled visualization of the acetabular rim and the ischium.

Following component extraction, meticulous debridement of all pseudocapsule, particulate debris, and fibrous tissue is performed. The true osseous limits of the defect must be identified. The ischium is exposed by dissecting the hamstrings and sacrotuberous ligament off the ischial tuberosity to prepare the slot for the inferior flange of the cage. Care must be taken to protect the sciatic nerve, which is often encased in scar tissue in the revision setting.
Acetabular Preparation and Cup Insertion
The acetabulum is sequentially reamed to bleeding host bone where possible, though aggressive reaming is avoided to preserve remaining bone stock. The goal is not to create a perfect hemisphere, but rather to identify at least two, preferably three, points of solid host bone contact (typically the superior dome, the ischium, and the pubis).
A highly porous metal cup is then impacted into the defect. The cup is often placed in an off-axis orientation, prioritizing host bone contact and initial stability over anatomic version and inclination. The subsequent cementation of the liner into the cage will correct the final articular geometry. If large cavitary defects remain behind the cup, highly porous metal augments or impacted cancellous allograft are utilized to fill the voids and support the primary shell. Multiple multi-hole screws are placed through the cup into the superior dome and posterior column to maximize initial fixation.
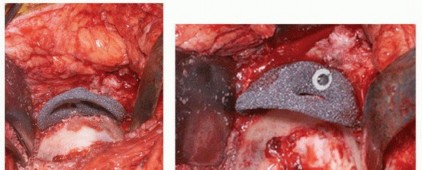
Cage Contouring and Fixation
The appropriate cage is selected based on preoperative templating and intraoperative trialing. The inferior flange is contoured to fit into the prepared ischial slot. The superior flange is contoured to lie flush against the lateral aspect of the ilium. Proper contouring is critical; a poorly contoured cage will experience high bending moments and subsequent fatigue failure.

The cage is inserted by first seating the inferior flange into the ischium. The superior flange is then impacted against the ilium. The cage should sit intimately against the previously placed highly porous cup. Fixation begins with the placement of cortical or cancellous screws through the superior flange into the dense bone of the ilium, aiming toward the sacroiliac joint. Screws are also placed through the central dome of the cage, passing through the cage, the underlying porous cup, and into the host bone, effectively locking the two components together. Care must be taken to avoid the superior gluteal neurovascular bundle during superior flange screw placement and the external iliac vessels during anterior screw placement.
Liner Cementation and Final Reduction
Once the cage is rigidly fixed, the surgical site is thoroughly irrigated and dried. A highly cross-linked polyethylene liner is selected. The back of the liner is often scored to enhance cement interdigitation. High-viscosity polymethylmethacrylate bone cement is applied to the inner surface of the cage.

The liner is pressurized into the cement mantle. The critical advantage of this technique is that the surgeon can manipulate the version and inclination of the polyethylene liner independently of the orientation of the underlying cage and cup. The liner is held in optimal anatomic orientation (typically 15 to 20 degrees of anteversion and 40 to 45 degrees of inclination) until the cement fully cures. Excess cement is meticulously removed to prevent third-body wear. The femoral component is then reconstructed as dictated by the femoral defect, and the hip is reduced and assessed for stability through a full range of motion.
Complications and Management
Intraoperative and Postoperative Challenges
Cup-cage reconstruction is a salvage procedure fraught with potential complications due to the complexity of the surgery, the compromised host tissues, and the extensive nature of the dissection.

Intraoperative complications include neurovascular injury, particularly to the sciatic nerve during ischial exposure or the superior gluteal vessels during iliac fixation. Iatrogenic fracture of the remaining compromised bone can occur during cup impaction or cage seating.
Postoperatively, dislocation remains a significant risk due to altered abductor mechanics, extensive soft tissue release, and potential leg length discrepancies. Infection is a catastrophic complication given the large volume of implanted hardware and the avascular nature of the surrounding scar tissue. Aseptic loosening and mechanical failure of the cage can occur if the underlying porous cup fails to achieve biologic ingrowth, leading to fatigue fracture of the cage flanges over time.
| Complication | Estimated Incidence | Prevention and Salvage Strategy |
|---|---|---|
| Dislocation | 10% - 15% | Prevention: Optimize liner version/inclination in cement; use large femoral heads; consider dual mobility liners. Salvage: Closed reduction, bracing. If recurrent, revision of cemented liner or conversion to constrained liner. |
| Infection (PJI) | 5% - 10% | Prevention: Strict asepsis, systemic antibiotics, local antibiotic powder, minimizing dead space. Salvage: DAIR (Debridement, Antibiotics, Implant Retention) for acute infections. Two-stage exchange for chronic PJI. |
| Sciatic Nerve Palsy | 3% - 8% | Prevention: Careful posterior dissection; avoid excessive retractor tension; identify and protect nerve during ischial slot preparation. Salvage: AFO bracing, physical therapy. Often resolves over 6-12 months if stretch injury. |
| Aseptic Loosening / Cage Breakage | 5% - 10% (at 10 years) | Prevention: Ensure rigid initial fixation; maximize host bone contact with porous cup to ensure load-sharing transition. Salvage: Revision to Custom Triflange, massive structural allograft, or custom 3D printed implants. |
| Vascular Injury | < 1% | Prevention: Respect safe zones for screw placement (avoid anterior-inferior quadrant for external iliacs; avoid superior gluteal notch). Salvage: Immediate vascular surgery consultation, packing, vessel ligation or repair. |
Post Operative Rehabilitation Protocols
Weight Bearing and Mobility
The postoperative rehabilitation protocol must be carefully tailored to protect the mechanical integrity of the reconstruction while promoting early mobilization to prevent systemic complications. Because the initial stability of the cup-cage construct relies entirely on the mechanical fixation of the cage to compromised bone, restricted weight-bearing is universally mandated.
Patients are typically restricted to toe-touch weight-bearing or flat-foot weight-bearing (approximately 20 pounds) on the operative extremity for a minimum of 6 to 12 weeks. This duration allows for the initial phases of biologic ingrowth into the highly porous primary cup. Premature weight-bearing subjects the cage to excessive shear and bending moments, increasing the risk of early hardware failure or loss of fixation.
Standard hip precautions are enforced for 12 weeks to minimize the risk of dislocation, particularly if a standard unconstrained liner was utilized. If an extended trochanteric osteotomy was performed, active abduction is restricted until radiographic evidence of osteotomy union is observed, typically around 8 to 12 weeks.
Deep vein thrombosis prophylaxis is critical given the extensive nature of the surgery and the period of restricted mobility. Pharmacologic prophylaxis (e.g., low molecular weight heparin, direct oral anticoagulants, or aspirin depending on patient risk stratification) is administered for 4 to 6 weeks postoperatively. Clinical and radiographic follow-up is typically conducted at 2 weeks, 6 weeks, 3 months, 6 months, 1 year, and annually thereafter to monitor for component migration, cage fracture, and progressive radiolucent lines.
Summary of Key Literature and Guidelines
Long Term Survivorship and Clinical Outcomes
The clinical efficacy of the cup-cage construct in managing severe acetabular defects has been well-documented in the orthopedic literature, demonstrating superior survivorship compared to historical techniques utilizing massive structural allografts or isolated anti-protrusio cages.

Seminal studies from major tertiary referral centers have validated the biomechanical rationale of the construct. Kosashvili et al. reported on the outcomes of cup-cage reconstructions in patients with severe bone loss and pelvic discontinuity, demonstrating an implant survivorship free of aseptic loosening of over 90 percent at a mean follow-up of five years. They highlighted the critical importance of the highly porous cup achieving biologic fixation, which subsequently unloads the cage and prevents late fatigue failure.
Abdel and colleagues from the Mayo Clinic evaluated the long-term outcomes of cup-cage constructs, noting that while complication rates (such as dislocation and infection) remain higher than in primary or less complex revision arthroplasty, the mechanical durability of the construct is excellent. Their data suggests a 10-year survivorship free from revision for aseptic loosening approaching 85 to 90 percent, a remarkable achievement given the dire preoperative bone stock in these cohorts.
Current academic consensus and guidelines from the American Association of Hip and Knee Surgeons support the use of cup-cage reconstructions or custom triflange acetabular components for Paprosky 3B defects and chronic pelvic discontinuities. The choice between a cup-cage and a custom triflange often depends on surgeon preference, the availability of intact iliac and ischial bone for cage fixation, and the urgency of the procedure, as cup-cage components are available off-the-shelf, whereas custom implants require significant lead time for manufacturing. In conclusion, mastery of the cup-cage technique provides the revision arthroplasty surgeon with a versatile, mechanically sound, and biologically viable solution for the most challenging acetabular reconstructions.
You Might Also Like