Arthrodesis of the Shoulder: Indications, Positioning, and Surgical Techniques
Key Takeaway
Shoulder arthrodesis is a powerful salvage procedure for complex glenohumeral pathology, including paralytic disorders, intractable infections, and failed arthroplasty. Achieving optimal functional outcomes relies heavily on precise arm positioning—typically 20 to 30 degrees of abduction, 20 to 30 degrees of forward flexion, and 40 degrees of internal rotation. Rigid internal fixation using dynamic compression or reconstruction plates ensures high union rates and facilitates early rehabilitation without the need for prolonged spica casting.
Arthrodesis of the Upper Extremity: General Principles
Arthrodesis of the upper extremity—encompassing the shoulder, elbow, and wrist—represents a critical, albeit increasingly rare, surgical intervention in modern orthopedic practice. The general principles of joint fusion dictate that the primary goal is to provide a stable, painless articulation at the expense of motion. In the upper extremity, arthrodesis is performed far less frequently than in the lower extremity. This disparity is largely due to the profound disability associated with sacrificing motion in the shoulder or elbow, coupled with the remarkable advancements in successful shoulder and elbow arthroplasty.
While the development of reverse total shoulder arthroplasty (RTSA) and total elbow arthroplasty (TEA) has significantly shortened the list of indications for fusion, arthrodesis remains an indispensable salvage procedure. It is particularly valuable for patients with profound paralytic disorders, intractable infections, or massive bone and soft-tissue loss where arthroplasty is destined to fail.
Shoulder Arthrodesis
Historical Context and the Evolution of Fixation
Around the turn of the 20th century, shoulder arthrodesis was a relatively common procedure. The primary indications at that time were upper extremity paralysis caused by poliomyelitis or severe joint destruction secondary to tuberculosis. Because the procedure reliably eliminated pain and provided a stable fulcrum for the arm, the list of indications expanded over the ensuing decades.
The earliest techniques relied entirely on extra-articular fusion to prevent the invasion of tuberculous infection from the joint space. With the advent of modern antitubercular pharmacotherapy, these extra-articular techniques became obsolete. Subsequent procedures evolved to utilize intra-articular decortication of the glenohumeral and acromiohumeral joints, supplemented by various types of bone grafting. However, these early methods lacked internal fixation, necessitating prolonged, debilitating postoperative immobilization in a shoulder spica cast.
Clinical Pearl: External support alone rarely maintains complete, rigid fixation of the shoulder. The micromotion inherent in cast immobilization significantly increases the risk of nonunion. Modern shoulder arthrodesis mandates rigid internal fixation to stabilize contact surfaces, promote primary bone healing, and allow for early rehabilitation.
In the early 1950s, Sir John Charnley introduced the concept of external fixation to apply dynamic compression across the fusion site. While innovative, fusion rates with external fixation alone were generally poor, and patients still required a spica cast for up to three months. In 1957, Carroll introduced a wire loop technique connecting the glenoid and humeral head, which allowed for postoperative adjustments in arm position.
The paradigm shifted dramatically in the 1960s with the introduction of internal fixation. Moseley and May described techniques utilizing screw fixation, which minimized soft-tissue dissection and lowered infection rates but still carried a high nonunion rate without spica casting. In 1970, the AO group revolutionized the procedure by publishing a technique utilizing rigid plate and screw fixation, allowing patients to mobilize without a spica cast. Kostuik and Schatzker later introduced double-plating techniques (using a posterior buttress plate), achieving a 100% union rate in their series.
Biomechanics of Fixation:
Miller et al. conducted a landmark biomechanical study evaluating various fixation constructs for shoulder arthrodesis. They demonstrated that double plating (utilizing 4.5 dynamic compression plates) provided the highest bending strength and torsional stiffness.
This was followed, in decreasing order of strength, by single plating, external fixation combined with screws, external fixation alone, and screws alone. Conversely, Rühmann et al. demonstrated in a cadaveric study that specific six-screw configurations could provide mechanical stability comparable to a 16-hole reconstruction plate. Today, the use of a malleable pelvic reconstruction plate is highly favored, as it allows for precise intraoperative contouring over the spine of the scapula and down the humeral shaft, minimizing hardware prominence while maintaining rigid compression.
Indications and Contraindications
Indications for glenohumeral arthrodesis have diminished significantly due to the near-eradication of polio, the decline of advanced tuberculosis, and the excellent functional outcomes of modern shoulder arthroplasty. Nevertheless, shoulder arthrodesis remains the procedure of choice for specific, complex pathologies where a stable, painless limb is required.
Current Indications for Shoulder Arthrodesis:
* Intractable Infection: Bacterial or tubercular infections that are uncontrolled with medication or serial debridements. In cases of persistent infection with joint incongruency, arthroplasty is strictly contraindicated. Arthrodesis, following aggressive debridement of sequestra, provides definitive management.
* Paralytic Disorders: Arthrodesis is highly effective for stabilizing flail limbs caused by traumatic brachial plexus injuries or obstetrical plexus palsies. By fusing the glenohumeral joint, patients can utilize intact scapulothoracic and trapezius musculature to achieve functional arm positioning.
* Combined Insufficiency of the Rotator Cuff and Deltoid: Patients lacking the muscle power to drive an arthroplasty (including RTSA) are better served by a fusion.
* Unreconstructable Rotator Cuff Tears in Young Laborers: A young, heavy manual laborer with massive, irreparable cuff tears and secondary osteoarthritis may function better with a solid fusion than with an arthroplasty, which carries a high risk of early aseptic loosening under heavy loads.
* Failed Shoulder Arthroplasty: When revision arthroplasty is impossible due to massive bone loss, absent musculature, or chronic infection, arthrodesis serves as a definitive salvage option.
* Recurrent Instability: Multidirectional instability or voluntary dislocations associated with severe arthritis that have failed multiple soft-tissue and bony stabilization procedures.
* Neoplastic Lesions: Tumor resections requiring massive allografts or resulting in profound soft-tissue deficits.
Surgical Warning: Shoulder arthrodesis relies entirely on the compensatory motion of the scapulothoracic articulation. Therefore, adequate function of the trapezius, levator scapulae, and serratus anterior muscles is an absolute prerequisite for a successful functional outcome.
Contraindications:
* Absolute: Contralateral shoulder fusion (bilateral fusions severely restrict activities of daily living, particularly perineal care), ipsilateral elbow fusion, and Charcot arthropathy (due to unacceptably high nonunion rates).
* Relative: Osteonecrosis with intact musculature (better treated with arthroplasty) and advanced age with low functional demands.
Preoperative Planning and Optimal Positioning
The most critical determinant of functional success in shoulder arthrodesis is the intraoperative positioning of the arm. An improperly positioned fusion will result in severe functional limitations, winging of the scapula, and chronic pain.
Historically, the optimal position has been a subject of intense debate. In 1974, Rowe recognized the severe disadvantages of excessive abduction and flexion, which lead to scapular winging at rest and muscle fatigue. Rowe recommended a position of 20 degrees of abduction, 30 degrees of forward flexion, and 40 to 50 degrees of internal rotation.
Subsequent functional analyses by Hawkins and Neer refined these parameters. They identified a range of acceptable positions, recommending 25 to 40 degrees of abduction, 20 to 30 degrees of flexion, and 25 to 30 degrees of internal rotation.
Cofield and Briggs, in a study of 71 shoulder arthrodeses, concluded that the degree of internal rotation is the single most important factor in determining functional success. Insufficient internal rotation prevents the patient from reaching their midline, face, or contralateral shoulder. Groh et al. defined symptomatic malunion requiring corrective osteotomy as greater than 15 degrees of flexion, and rotation of less than 40 degrees or more than 60 degrees.
Intraoperative Clinical Assessment of Position:
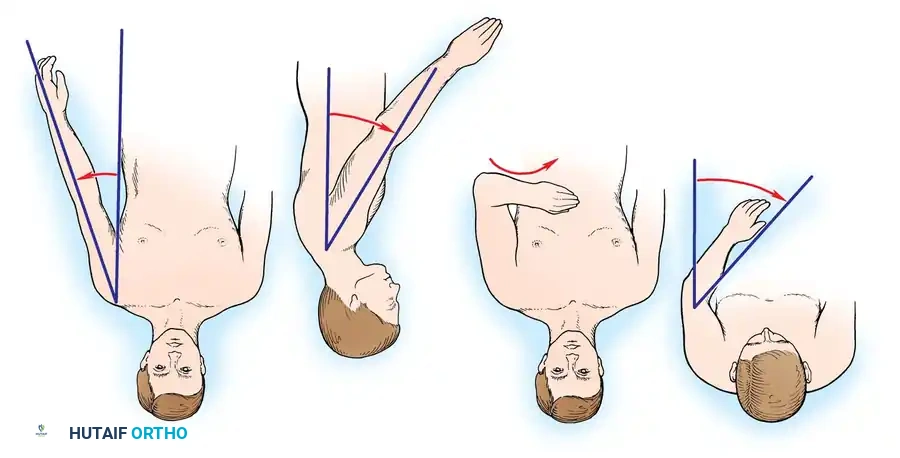
Because radiographic measurement of these angles intraoperatively can be challenging due to patient positioning, clinical landmarks are heavily relied upon.
1. Abduction: Measured clinically as the angle formed between the medial border of the humerus and the lateral border of the trunk.
2. Flexion: Determined by observing the angle the humerus forms with the horizontal plane of the thorax.
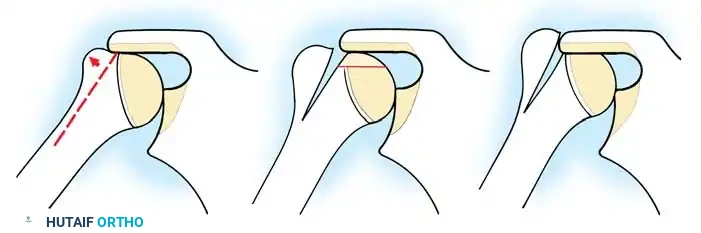
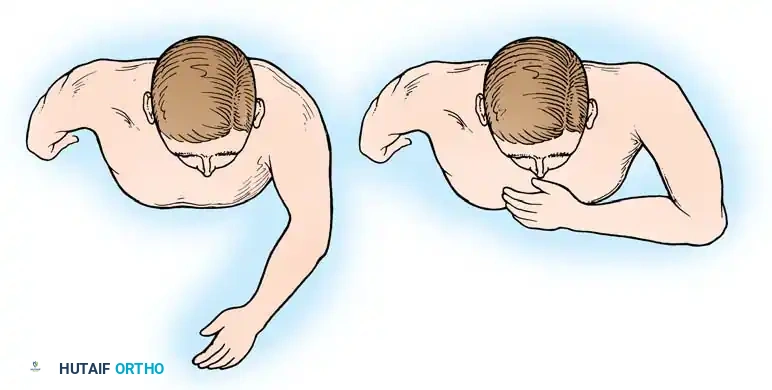
3. Internal Rotation (The Hand-to-Mouth Test): With the shoulder provisionally fixed in the desired abduction and flexion, the elbow is flexed to 90 degrees. The hand should rest comfortably over the ipsilateral chest, midway between the sternum and the axilla. Further flexion of the elbow should allow the tip of the thumb to easily reach the patient's chin and mouth.
Surgical Approaches and Step-by-Step Technique
The modern standard for shoulder arthrodesis involves intra-articular decortication combined with rigid internal plate fixation, capturing the acromion, humeral head, and glenoid.
1. Patient Positioning and Incision
The patient is typically placed in a beach-chair position or lateral decubitus position, depending on surgeon preference. The entire forequarter, including the neck, chest, and arm down to the hand, must be prepped and draped free to allow for intraoperative assessment of arm positioning.
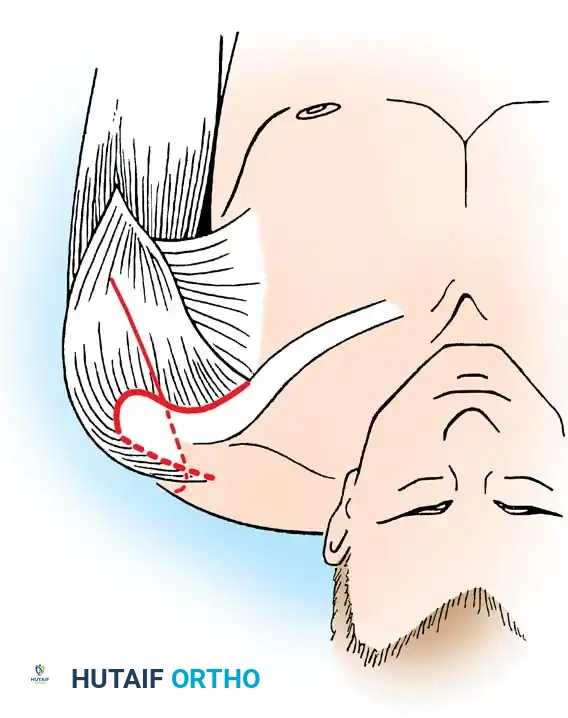
A broad strap incision is utilized. The incision begins over the spine of the scapula, extends laterally over the acromion, and curves distally down the anterolateral aspect of the humerus.
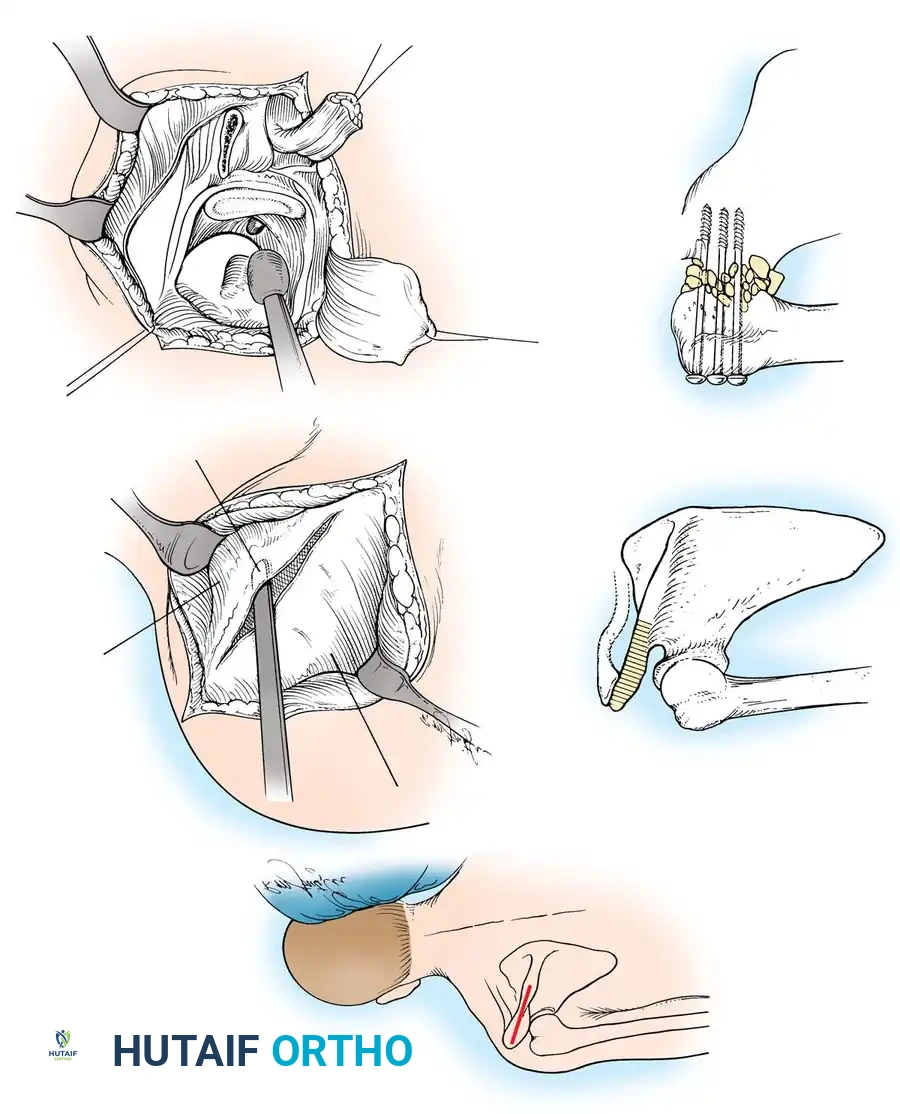
2. Surgical Exposure
The deltoid muscle is split or reflected off the anterior and lateral acromion. The underlying rotator cuff tendons (supraspinatus, infraspinatus, and subscapularis) are systematically excised to fully expose the articular surfaces of the humeral head and the glenoid fossa. The undersurface of the acromion is also exposed, as it will serve as a secondary fusion bed.
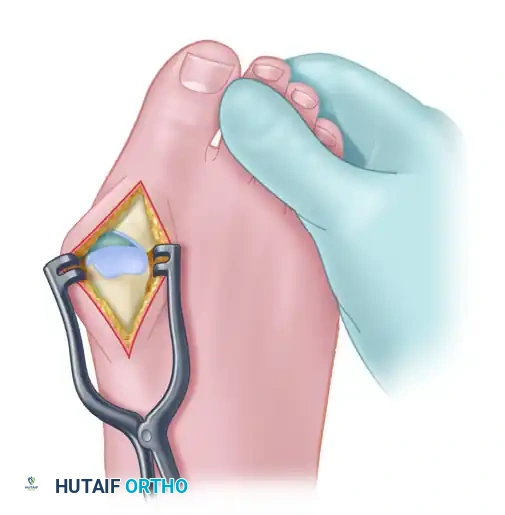
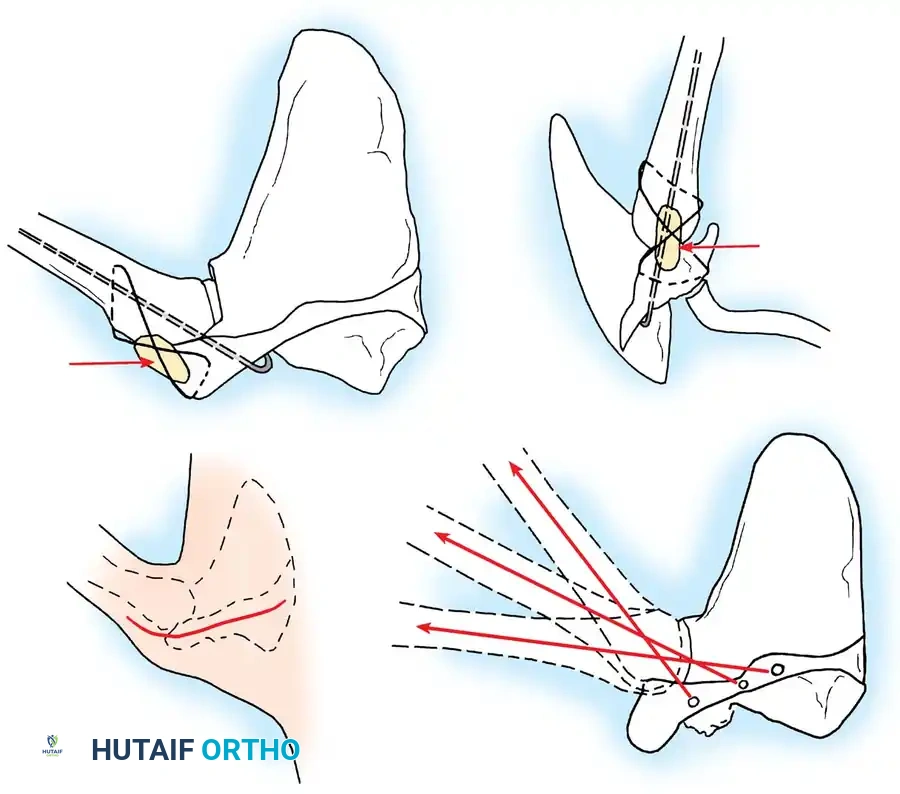
3. Joint Preparation and Decortication
Meticulous preparation of the bony surfaces is paramount to achieving a solid arthrodesis. All articular cartilage must be aggressively removed using a combination of osteotomes, gouges, and high-speed burrs.
The glenoid is decorticated down to bleeding subchondral bone. The humeral head is similarly denuded. To maximize the surface area for fusion, the undersurface of the acromion is decorticated, and a corresponding flat surface is created on the superior aspect of the greater tuberosity.
In some techniques, an intra-articular osteotomy of the humeral head is performed to create a flat, broad cancellous surface that perfectly mates with the decorticated glenoid.

4. Provisional Fixation and Positioning
The arm is placed into the predetermined optimal position (20-30° abduction, 20-30° flexion, 40° internal rotation). The hand-to-mouth test is performed. Once the position is confirmed, heavy Steinmann pins or K-wires are driven from the lateral humerus, through the humeral head, and into the glenoid vault to provisionally hold the construct.
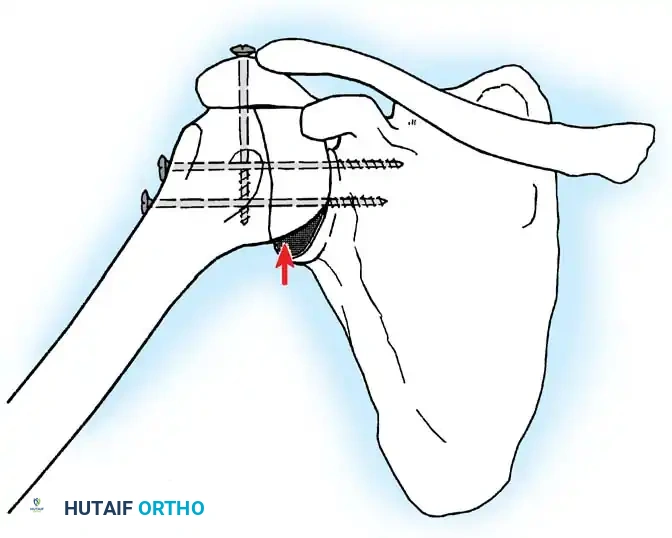
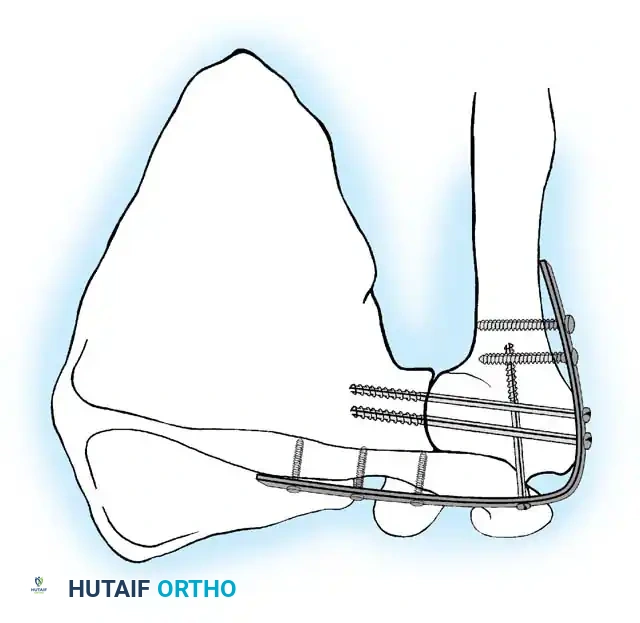
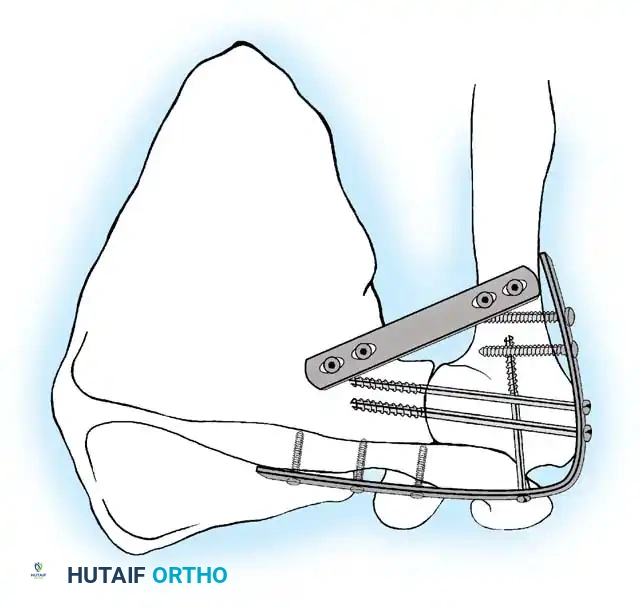
5. Rigid Internal Fixation
The most robust biomechanical construct involves a heavy, malleable plate (such as a 10- to 14-hole 4.5mm pelvic reconstruction plate or a dynamic compression plate). The plate is meticulously contoured to lie flat along the spine of the scapula, bend over the acromion, and extend down the lateral shaft of the humerus.
Screws are placed sequentially:
1. Scapular Spine: Cortical screws are placed into the dense bone of the scapular spine.
2. Acromiohumeral Fixation: Screws are passed through the plate, across the acromion, and into the humeral head.
3. Glenohumeral Fixation: Long, fully threaded cortical or cancellous screws are directed through the plate, through the humeral head, and deep into the glenoid neck and vault. This is the most critical step for achieving compression across the primary fusion site.
4. Humeral Shaft: The distal portion of the plate is secured to the humeral diaphysis.
If additional stability is required, or if bone quality is poor, a second plate (double plating technique) can be applied posteriorly.
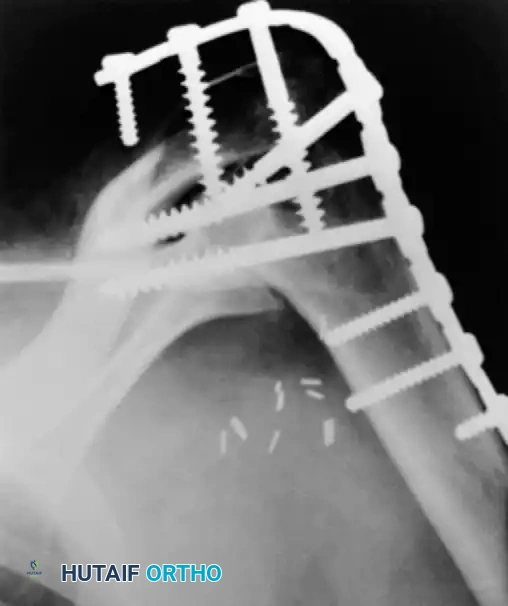
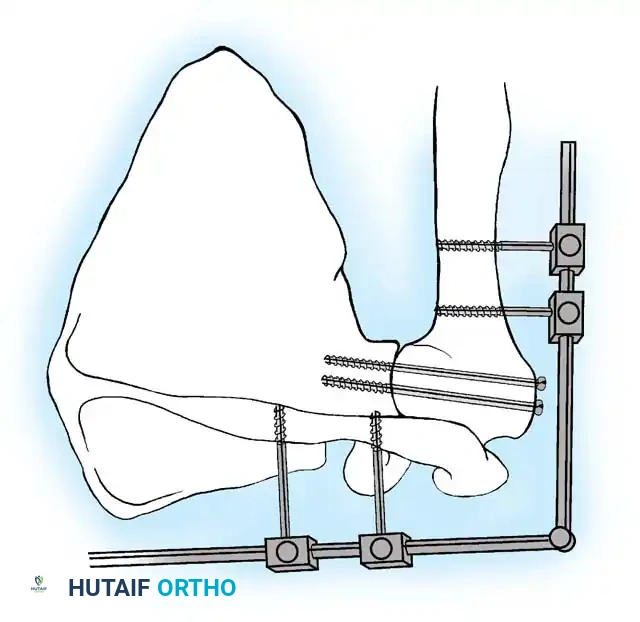
Radiographic confirmation of a contoured reconstruction plate achieving rigid acromiohumeral and glenohumeral compression.
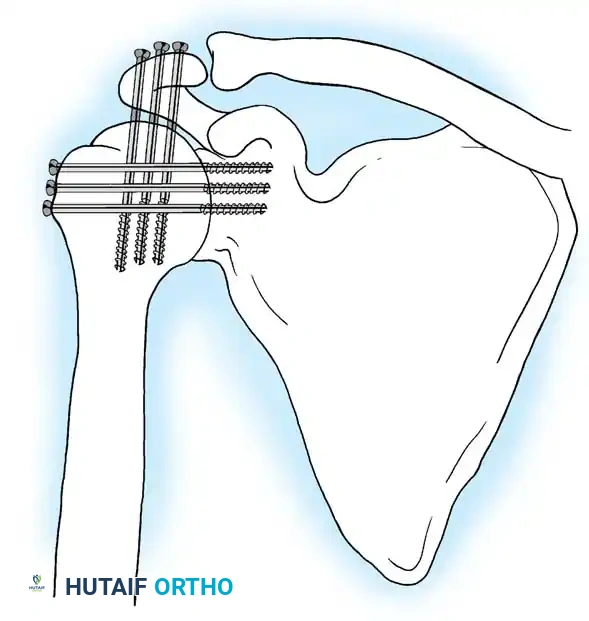
Alternative Fixation: Screw-Only Constructs
In cases where soft-tissue coverage is extremely poor, or hardware prominence is a major concern, a screw-only construct may be utilized. This involves passing multiple large-fragment (6.5mm or 7.3mm) cannulated screws from the proximal humerus into the glenoid, and from the acromion into the humeral head. While this requires less dissection, it is biomechanically inferior to plate fixation and often necessitates postoperative spica casting.
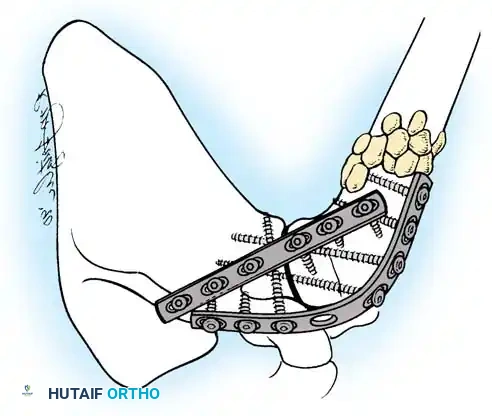
6. Bone Grafting
Autogenous bone graft is highly recommended to augment the fusion mass. Local bone resected from the humeral head or acromion can be packed into the interstices of the fusion site. If local bone is insufficient or of poor quality (e.g., in cases of infection or failed arthroplasty), autologous iliac crest bone graft (ICBG) should be harvested and packed around the glenohumeral and acromiohumeral interfaces.
Postoperative Protocol and Rehabilitation
The advent of rigid internal plate fixation has largely eliminated the need for prolonged, debilitating shoulder spica casts.
- Immobilization: Postoperatively, the patient is placed in a custom-molded thermoplastic shoulder orthosis (abduction brace) that supports the arm in the fused position. This brace is typically worn full-time for 6 to 8 weeks.
- Early Rehabilitation: Immediate active range of motion of the elbow, wrist, and hand is encouraged to prevent distal stiffness.
- Radiographic Follow-up: Serial radiographs are obtained at 2, 6, and 12 weeks. Once clinical and radiographic evidence of trabecular bridging is observed (usually between 8 to 12 weeks), the orthosis is weaned.
- Late Rehabilitation: Physical therapy then focuses on maximizing the strength and endurance of the scapulothoracic musculature (trapezius, serratus anterior, levator scapulae), which will now serve as the sole motor unit for the entire upper extremity.
Complications and Salvage
While modern techniques have improved outcomes, shoulder arthrodesis remains a technically demanding procedure with a recognized complication profile.
- Nonunion: The most common complication, historically occurring in up to 10-15% of cases, though modern plating techniques have reduced this to less than 5%. Nonunion is often asymptomatic and fibrous, providing a stable pseudarthrosis. If painful, revision arthrodesis with bone grafting and revision plating is required.
- Malposition: Excessive abduction leads to chronic pain, scapular winging, and traction on the brachial plexus. Insufficient internal rotation prevents the patient from reaching their mouth or midline. Symptomatic malunion requires a corrective proximal humeral osteotomy.
- Hardware Prominence: The plate over the spine of the scapula and acromion can become prominent and painful, particularly in thin patients. Hardware removal may be considered after 12 to 18 months, provided solid bony union is confirmed on CT scan.
- Adjacent Segment Disease: Over time, the increased mechanical demand placed on the scapulothoracic and acromioclavicular joints can lead to secondary osteoarthritis and chronic periscapular pain.
- Humeral Shaft Fracture: A stress riser is created at the distal end of the fixation plate. Patients are at risk for periprosthetic fractures of the humeral diaphysis if subjected to high-energy trauma.
In conclusion, while the indications for shoulder arthrodesis have narrowed, it remains a highly effective, durable procedure for the appropriate patient. Meticulous attention to intraoperative positioning, aggressive joint decortication, and the application of rigid, biomechanically sound internal fixation are the cornerstones of a successful outcome.
📚 Medical References
- shoulder arthrodesis, J Bone Joint Surg 83A:593, 2001.
- Cofi eld RH: Shoulder arthrodesis and resection arthroplasty, Instr Course Lect 34: 268, 1985.
- Cofi eld RH: Arthrodesis and resectional arthroplasty of the shoulder. In Evarts CM, ed: Surgery of the musculoskeletal system, ed 2, New York, 1990, Churchill Livingstone. Cofi eld RH, Briggs BT: Glenohumeral arthrodesis: operative and long-term functional results, J Bone Joint Surg 61A:668, 1979.
- Damron TA, Rock MG, O’Connor MI, et al: Functional laboratory assessment after oncologic shoulder joint resectors, Clin Orthop Relat Res 348:124, 1998.
- Davis JB, Cottrell GW: A technique for shoulder arthrodesis, J Bone Joint Surg 44A:657, 1962.
- Diaz JA, Cohen SB, Warren RF, et al: Arthrodesis as a salvage procedure for recurrent instability of the shoulder, J Shoulder Elbow Surg 12:237, 2003.
- Emmelot CH, Nielsen HKL, Eisma WH: Shoulder fusion for paralyzed upper limb, Clin Orthop Relat Res 340:95, 1997.
- Gill AB: A new operation for arthrodesis of the shoulder, J Bone Joint Surg 13:287, 1931.
- Gill TJ, Warren RF, Rockwood CA, et al: Complications in shoulder surgery, Instr Course Lect 48:359, 1999.
- Gonzalez-Diaz R, Rodriguez-Merchan EC, Gilbert MS: The role of shoulder fusion in the era of arthroplasty, Int Orthop 21:204, 1997.
- Groh GI, Williams GR, Jarman RN, et al: Treatment of complications of shoulder arthrodesis, J Bone Joint Surg 79A:881, 1997.
- Hawkins RJ, Neer CS II: A functional analysis of shoulder fusions, Clin Orthop Relat Res 223:65, 1987.
- Ingram AJ, Miller TR: Arthrodesis of the shoulder, Memphis, Tenn, 1950 (unpublished). Johnson CA, Healy WL, Brooker AF Jr, et al: External fixation shoulder arthrodesis, Clin Orthop Relat Res 211:219, 1986.
- Jonsson E, Lidgren L, Rydholm U: Position of shoulder arthrodesis measured with moiré photography, Clin Orthop Relat Res 238:117, 1989.
- Kocialkowski A, Wallace WA: Shoulder arthrodesis using an external fixator, J Bone Joint Surg 73B:180, 1991.
- Kostuik JP, Schatzker J: Shoulder arthrodesis—family variant— A.O. technique. In Bateman JE, Welsh RP, eds : Surgery of the shoulder, Toronto, 1984, Mosby. Kumar VP, Satku SK, Mitra AK, et al: Function following limb salvage for primary tumors of the shoulder girdle: 10 patients followed 4 (1–11) years, Acta Orthop Scand 65:55, 1994.
- Lettin A: Shoulder replacement in rheumatoid arthritis, Reconstr Surg Traumatol 18:55, 1981.
- Mah JY, Hall JE: Arthrodesis of the shoulder in children, J Bone Joint Surg 72A:582, 1990.
- Makin M: Early arthrodesis for a fl ail shoulder in young children, J Bone Joint Surg 59:317, 1977.
- May VR Jr: Shoulder fusion: a review of fourteen cases, J Bone Joint Surg 44A:65, 1962.
- Miller BS, Harper WP, Gillies RM, et al: Biomechanical analysis of five fixation techniques used in glenohumeral arthrodesis, Aust N Z J Surg 73:1015, 2003.
- Mitsunaga MM, Jones DA, Parkinson D: Arthrodesis of the paralytic shoulder in children, Orthop Trans 11:186, 1987 (abstract). Mohammed NSE-S: A simple method of shoulder arthrodesis, J Bone Joint Surg 80B:620, 1998.
- Morgan CD, Casscells CD: Arthroscopic-assisted glenohumeral arthrodesis, Arthroscopy 8:262, 1992.
- Moseley HF: Arthrodesis of the shoulder in the adult, Clin Orthop 20:156, 1961.
- Müller ME, Allgower M, Willenegger H: Manual of internal fi xation: techniques recommended by the AO group, Berlin, 1979, Springer-Verlag. Nagano A, Okinaga S, Ochiai N, et al: Shoulder arthrodesis by external fixation, Clin Orthop Relat Res 247:97, 1989.
- Nagy L, Koch PP, Gerber C: Functional analysis of shoulder arthrodesis, J Shoulder Elbow Surg 13:386, 2004.
- O’Connor MI, Sim FH, Chao EYS: Limb salvage for neoplasms of the shoulder girdle: intermediate reconstructive and functional results, J Bone Joint Surg 78A:1872, 1996.
- Oppenheim WL, Lewis K, Jinnah R: Shoulder arthrodesis for neuromuscular impairment in children, Orthop Trans 11:109, 1987 (abstract). Pruitt DL, Hulsey RE, Fink B, et al: Shoulder arthrodesis in pediatric patients, J Pediatr Orthop 12:640, 1992.
- Putti V: Arthrodesis for tuberculosis of the knee and of the shoulder, Chir Organi Mov 18:217, 1933.
- Richards RR, Sherman RMP, Hudson AR, et al: Shoulder arthrodesis using a pelvic-reconstruction plate: a report of eleven cases, J Bone Joint Surg 70A:416, 1988.
- Rouholamin E, Wootton JR, Jamieson AM: Arthrodesis of the shoulder following brachial plexus injury, Injury 22:271, 1991.
- Rowe CR: Re-evaluation of the position of the arm in arthrodesis of the shoulder in the adult, J Bone Joint Surg 56A:913, 1974.
- Rowe CR: Arthrodesis of the shoulder used in treating painful conditions, Clin Orthop Relat Res 173:92, 1983.
- Rühmann O, Kirsch L, Buch S, et al: Primary stability of shoulder arthrodesis using cannulated cancellous screws, J Shoulder Elbow Surg 14:51, 2005.
- Rühmann O, Schmolke S, Bohnsack M, et al: Shoulder arthrodesis: indications, technique, results, and complications, J Shoulder Elbow Surg 14:38, 2005.
- Rybka V, Raunio P, Vainio K: Arthrodesis of the shoulder in rheumatoid arthritis: a review of forty-one cases, J Bone Joint Surg 61B:155, 1979.
- Schroder HA, Frandsen PA: External compression arthrodesis of the shoulder joint, Acta Orthop Scand 54:592, 1983.
- Sjostrom L, Mjoberg B:
You Might Also Like