Arthrodesis of the Ankle, Knee, and Hip: Advanced Surgical Principles and Techniques

Key Takeaway
Arthrodesis remains a highly effective surgical solution for end-stage arthritis, providing reliable pain relief and functional restoration. Achieving a successful fusion requires meticulous joint preparation, rigid fixation, and precise alignment. This guide details the biomechanical principles, surgical approaches, and fixation strategies—including internal compression and external frames—essential for orthopedic surgeons to optimize patient outcomes, restore plantigrade weight-bearing, and minimize complications such as nonunion or adjacent segment disease.
Principles of Major Joint Arthrodesis
Arthrodesis is a definitive surgical procedure designed to produce solid bony ankylosis across a diseased or severely damaged joint. While modern arthroplasty has largely superseded fusion for primary osteoarthritis, arthrodesis remains an indispensable, highly satisfactory solution for complex pathologies, including chronic infection, massive bone loss from tumors, severe high-energy trauma, paralytic conditions, and neuropathic (Charcot) arthropathy.
The primary biomechanical trade-off of arthrodesis is the sacrifice of joint mobility for absolute stability and pain relief. Consequently, arthrodesis invariably alters the biomechanics of the kinetic chain, increasing mechanical stress and energy requirements during ambulation. The energy expenditure increases significantly depending on the joint fused: ankle arthrodesis increases energy expenditure by approximately 10%, knee arthrodesis by 25-30%, and hip arthrodesis by up to 35%. Despite these physiological demands, the ability to achieve a stable, painless, and highly functional limb—especially in young, vigorous laborers—often outweighs the disadvantages of stiffness. Furthermore, modern reconstructive techniques now allow for the successful conversion of hip, and occasionally knee, arthrodeses to total joint arthroplasties later in life if adjacent segment disease becomes debilitating.
Clinical Pearl: Arthrodesis techniques are broadly categorized into intraarticular, extraarticular, or combined approaches. Extraarticular techniques are particularly advantageous in pediatric patients to preserve cartilaginous growth potential, or in the presence of active intraarticular infection (e.g., tuberculosis) and massive avascular necrosis. Intraarticular techniques, conversely, allow for superior correction of complex deformities and are preferred when adequate healthy cancellous bone can be apposed.
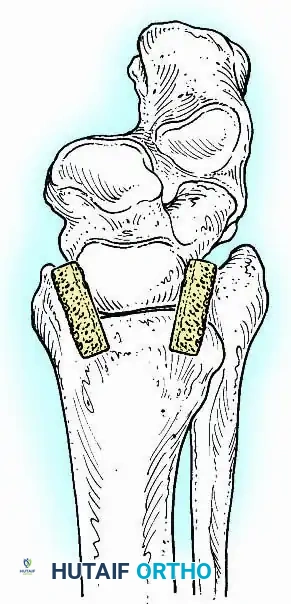
When local bone stock is deficient, the augmentation of the fusion site with bone grafts—preferably autogenous cancellous bone harvested from the iliac crest or proximal tibia—is mandatory. The prepared bony surfaces must be held in rigid apposition under compression using internal or external fixation. In highly complicated scenarios involving severe malposition, active infection, or compromised soft-tissue envelopes, circular external fixation (e.g., the Ilizarov method) provides unparalleled versatility.
Ankle Arthrodesis
Arthrodesis of the ankle is performed with significantly greater frequency than that of the hip or knee. The most common indication is end-stage posttraumatic arthritis, which accounts for over 70% of cases.

Other primary indications include rheumatoid arthritis, chronic osteomyelitis, neuromuscular instability, and the salvage of a failed total ankle arthroplasty (TAA). Recently, ankle arthrodesis has seen increased utilization in patients with severe, nonbraceable neuropathic (Charcot) arthropathy. However, surgeons must be acutely aware that complication rates—specifically deep infection and nonunion—are exponentially higher in the neuropathic population. Advanced techniques, such as the use of adolescent condylar blade plates, large-diameter cannulated AO screws, and antibiotic-impregnated allograft mixtures, have been developed to mitigate these risks.
Optimal Positioning and Biomechanics
The functional success of an ankle arthrodesis is entirely dependent on precise spatial alignment. Malpositioning leads to rapid degeneration of the subtalar and midtarsal joints, altered gait mechanics, and severe forefoot overload.
The universally accepted optimal position for ankle fusion is:
* Sagittal Plane: 0 degrees of flexion (neutral dorsiflexion/plantarflexion). Equinus positioning must be strictly avoided, as it causes genu recurvatum and midfoot breakdown.
* Coronal Plane: 0 to 5 degrees of valgus. Varus positioning locks the transverse tarsal joint, creating a rigid, unforgiving foot during the stance phase.
* Axial Plane: 5 to 10 degrees of external rotation, matching the contralateral limb's tibial torsion.
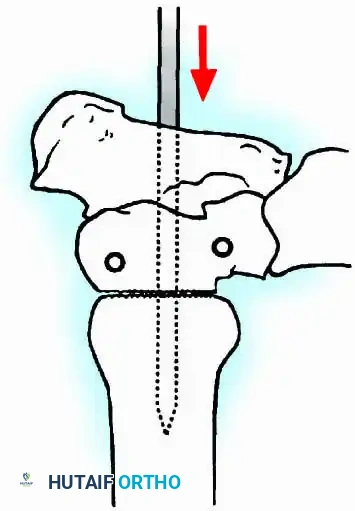
* Translation: Slight posterior displacement of the talus relative to the tibia. This decreases the anterior lever arm of the foot, reducing the bending moment at the fusion site and facilitating an easier rollover during gait.
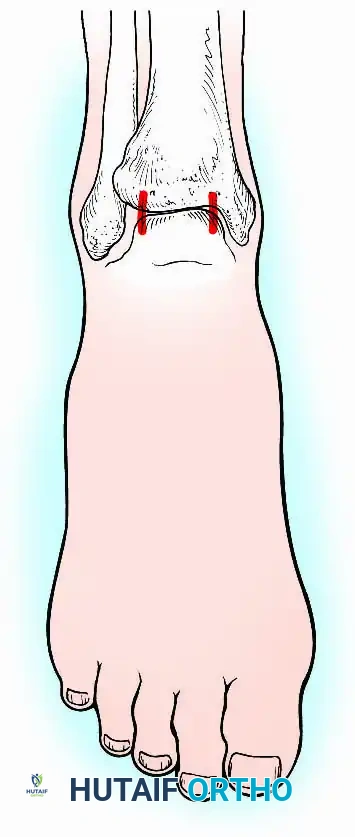
Surgical Warning: To accurately assess alignment intraoperatively, the lower extremity must be draped free from the toes to above the knee. Assessing rotation without visualizing the tibial tubercle and patella will inevitably lead to malrotation.
Following a successful fusion (achieved in 80% to 90% of modern cohorts), patients experience profound pain relief. However, the loss of tibiotalar motion restricts hindfoot kinematics, making ambulation on uneven terrain challenging. Running is generally precluded. Postoperatively, gait efficiency can be significantly enhanced by prescribing a rocker-bottom shoe modification with a solid-ankle, cushioned-heel (SACH) insert to simulate plantarflexion at heel strike and dorsiflexion at toe-off.
General Principles of Joint Preparation
Regardless of the specific approach or fixation method utilized, several universal principles must be strictly observed to ensure a high probability of union:
- Surface Area: Create broad, flat, bleeding cancellous surfaces. The subchondral bone plate must be adequately breached or resected to expose osteogenic marrow.
- Rigid Stability: The arthrodesis site must be stabilized with rigid internal or external fixation, applying dynamic compression across the osteotomy surfaces.
- Plantigrade Alignment: The hindfoot must be perfectly aligned to the mechanical axis of the leg, and the forefoot aligned to the hindfoot, to create a stable, plantigrade weight-bearing surface.
Surgical Approaches for Ankle Arthrodesis
The soft-tissue envelope surrounding the ankle is notoriously thin, lacking robust subcutaneous fat, and is frequently compromised by previous trauma, scarring, or multiple surgeries. Surgical approaches must respect angiosomes and avoid undue tension on skin flaps. Full-thickness fasciocutaneous flaps are mandatory to prevent marginal necrosis and skin slough.
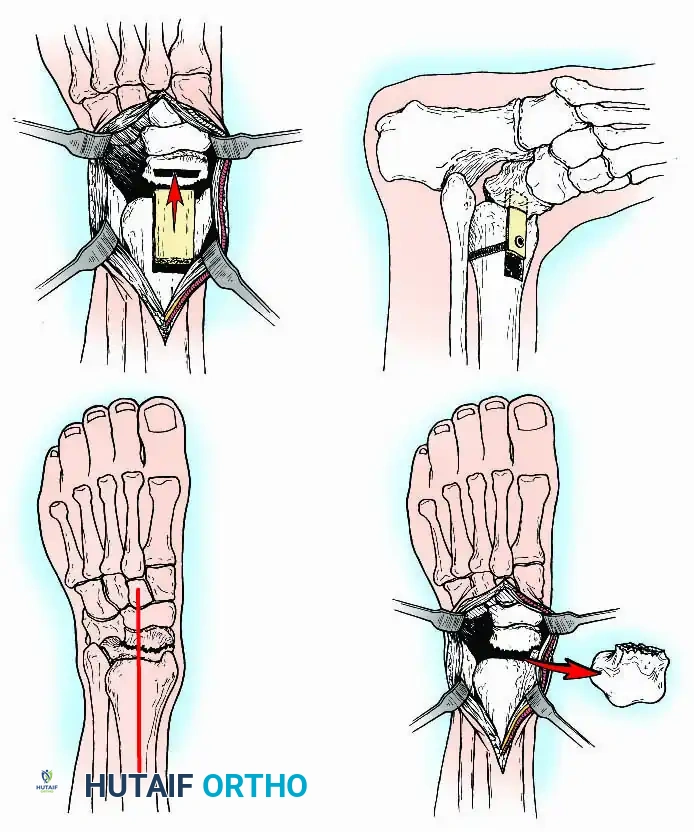
Anterior Approach
The anterior approach is typically performed through the internervous plane between the extensor hallucis longus (EHL) and the extensor digitorum longus (EDL), often utilizing the anterior tibial tendon sheath. This provides excellent, direct visualization of the central tibiotalar articulation and allows for easy posterior translation of the talus. However, access to the medial and lateral gutters is restricted, sometimes necessitating accessory incisions.
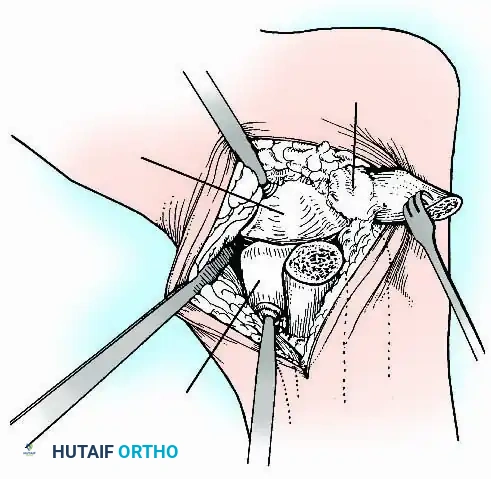
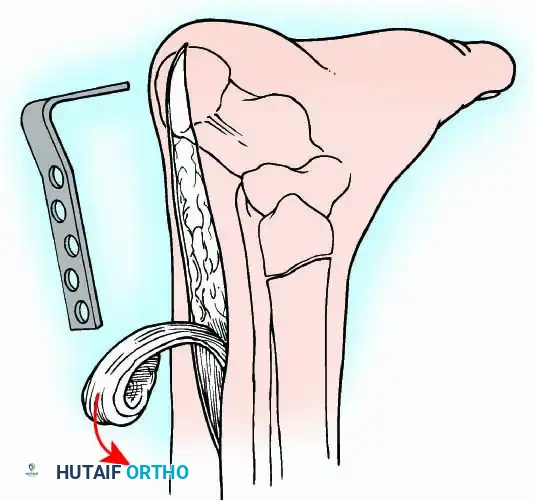
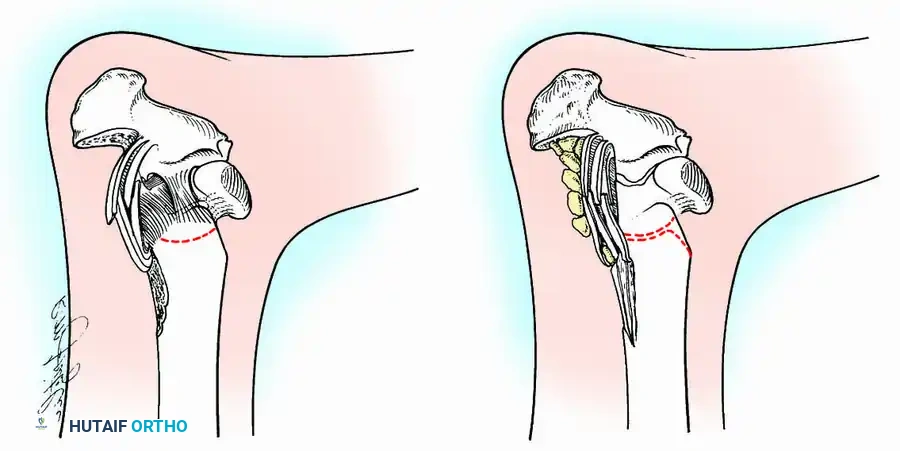
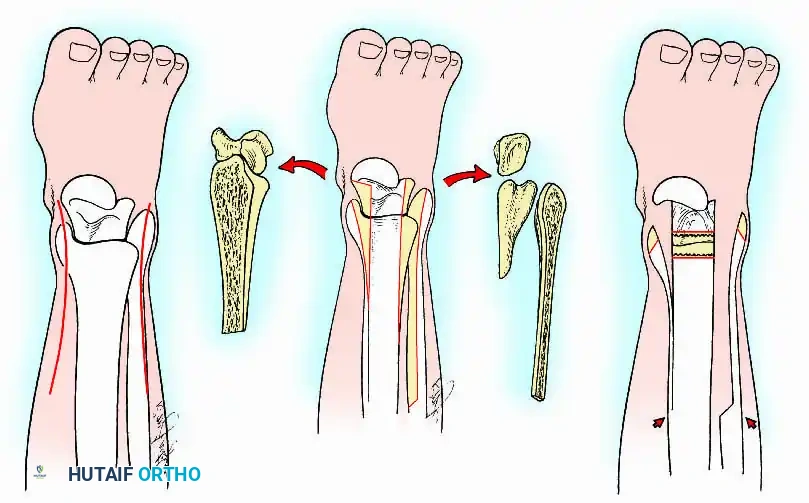
Transmalleolar (Transfibular) Approach
This approach utilizes a lateral incision over the distal fibula. A transfibular osteotomy is performed, reflecting the distal fibula distally or excising it entirely to be used as autograft. This provides unparalleled exposure of the lateral half of the joint and the posterior facet. It is highly effective for correcting severe varus/valgus deformities. A supplementary medial incision (medial malleolar osteotomy) can be added for complete joint exposure.
Posterior Approach
The posterior approach is indicated primarily for isolated tibiotalar fusions in patients with severely compromised anterior soft tissues (e.g., previous flap coverage, severe scarring). It is also the workhorse approach for combined tibiotalocalcaneal (TTC) arthrodesis. The plane of dissection typically follows an internervous route behind the fibula, mobilizing the Achilles tendon and neurovascular bundle.
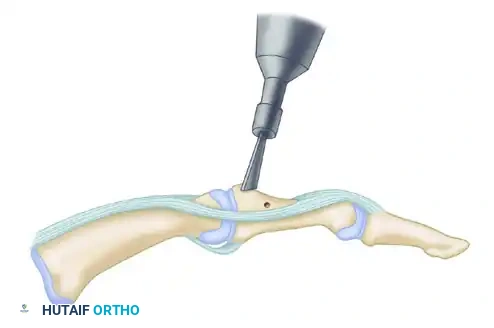
Preparation of Joint Surfaces
Two primary philosophies exist for joint preparation:
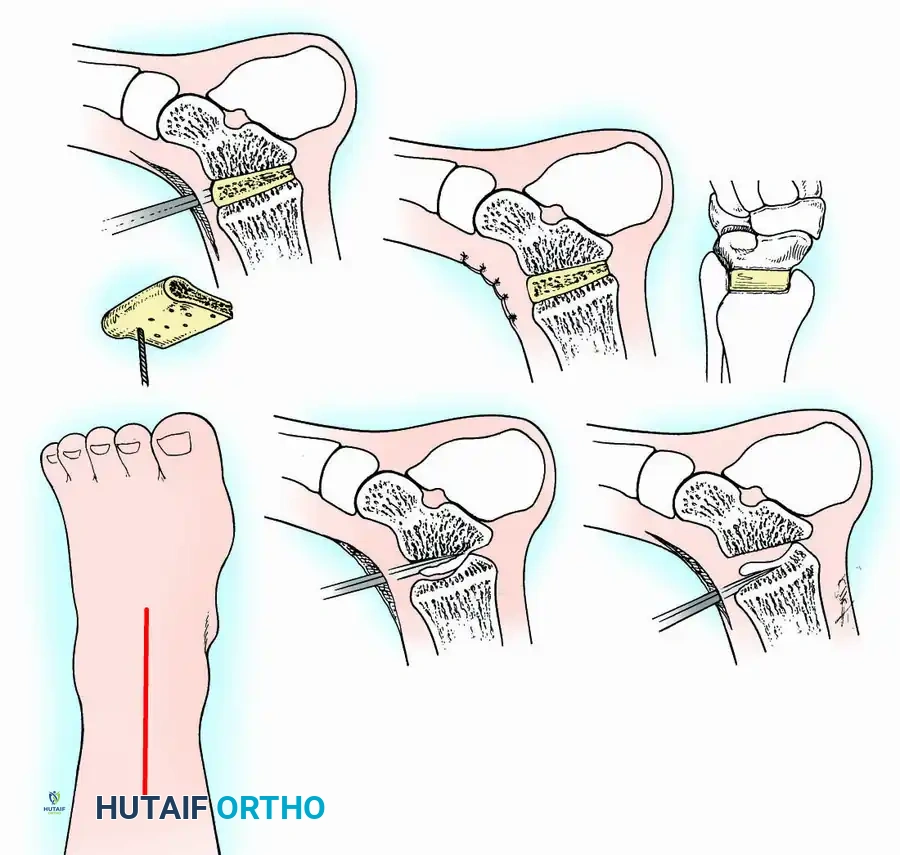
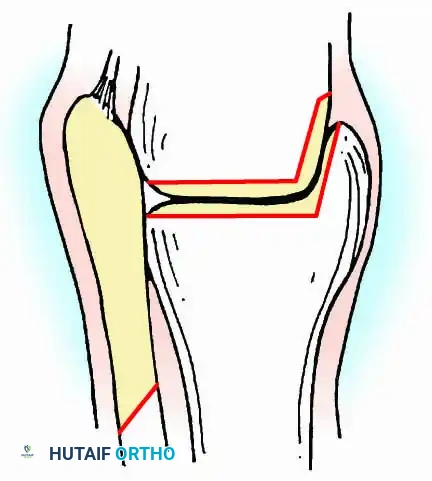
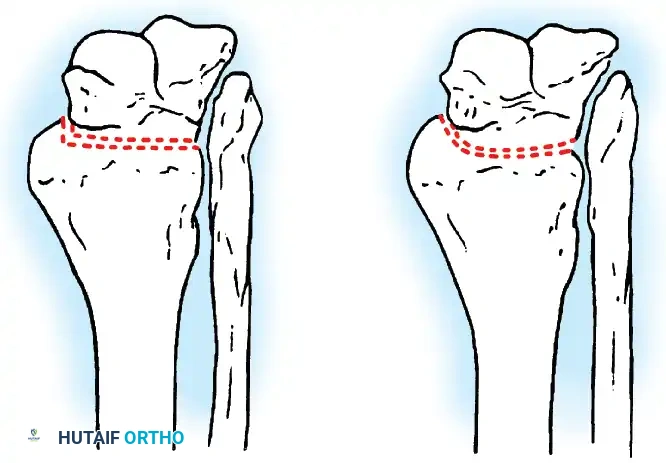
- Contour Preservation (Fishscaling): The remaining articular cartilage is meticulously denuded using curettes, and the subchondral bone is "fishscaled" or aggressively petalled with a sharp osteotome. This preserves the native ball-and-socket contour of the ankle, maximizing inherent bony stability and minimizing limb shortening.
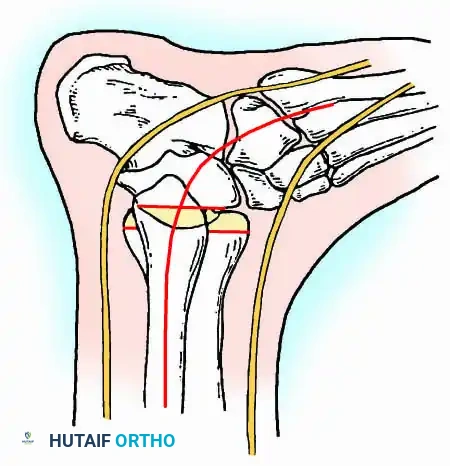
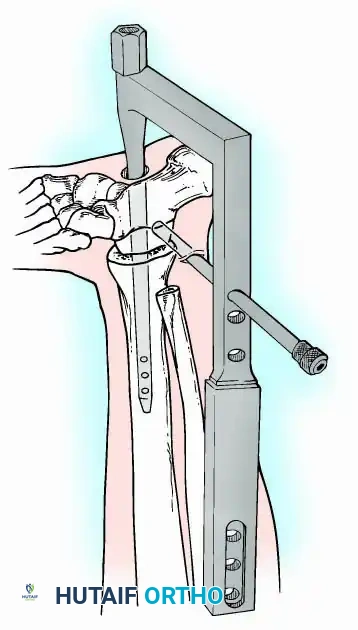
- Planar Resection (Parallel Cuts): Two parallel cuts are made—one through the distal tibial plafond and one through the talar dome—using an oscillating saw. This technique resects a minimal amount of bone but creates perfectly flat, highly vascular cancellous surfaces that allow for excellent apposition and easy posterior translation of the talus. Extramedullary alignment guides (often repurposed from total knee arthroplasty systems) can be utilized to ensure precise, parallel resections.
Fixation Techniques
Fixation is achieved via external compression frames, large-diameter internal cancellous screws, or intramedullary devices. The choice of fixation depends heavily on bone quality, soft-tissue integrity, and the presence of infection.
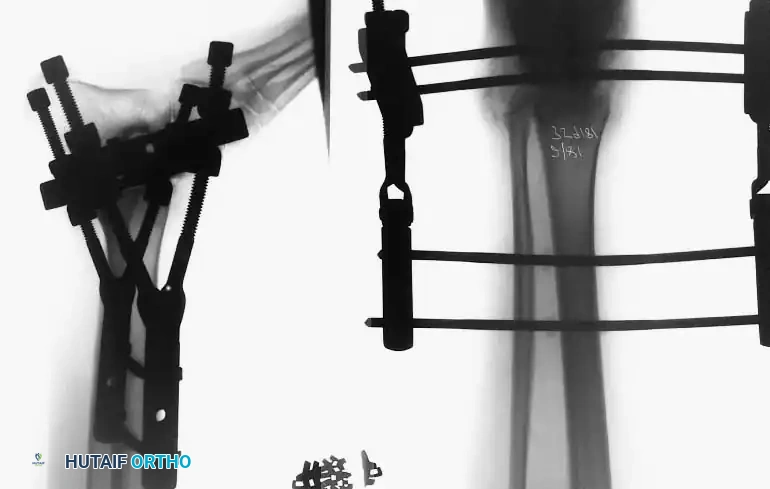
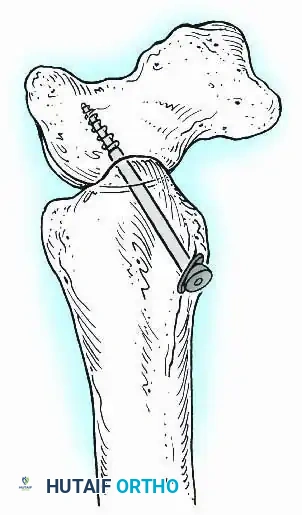
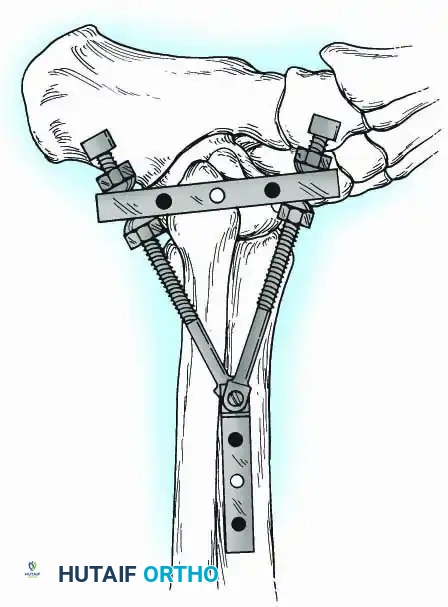
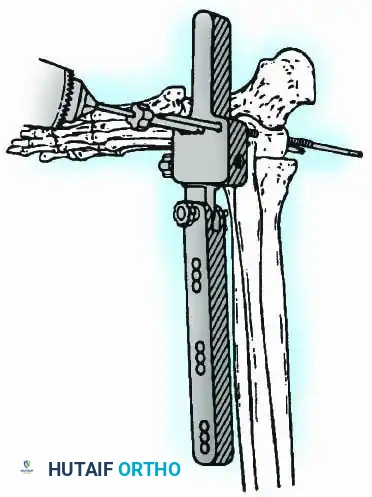
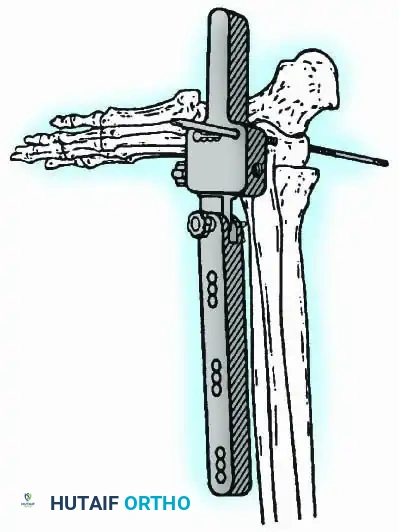
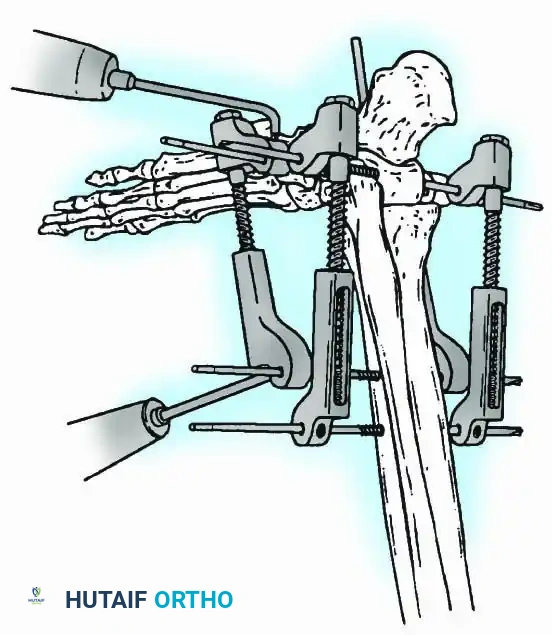
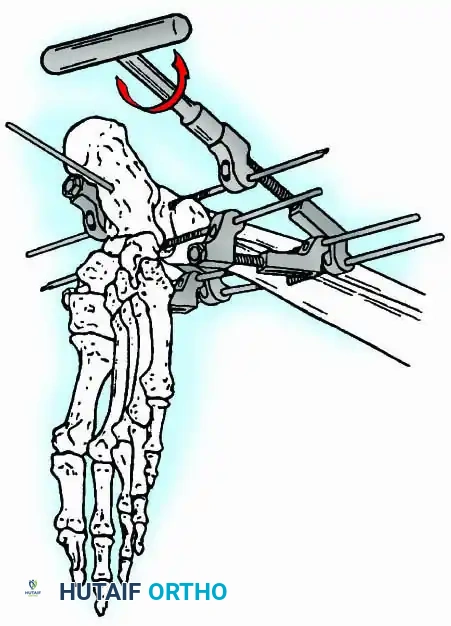
External Fixation
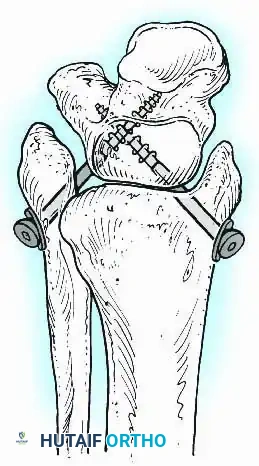
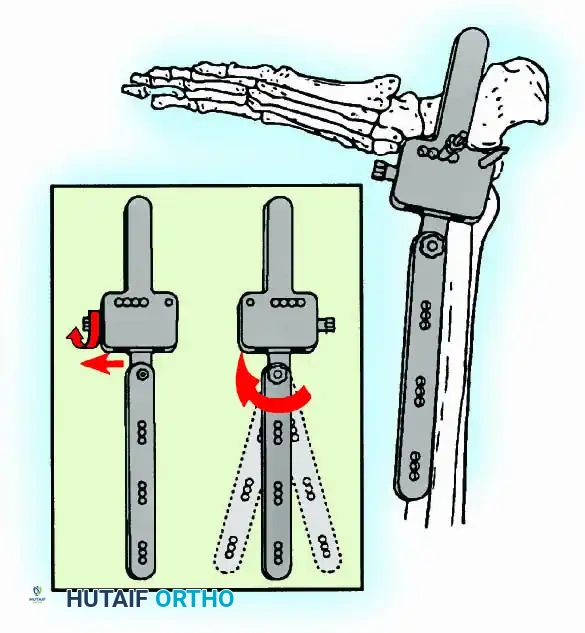
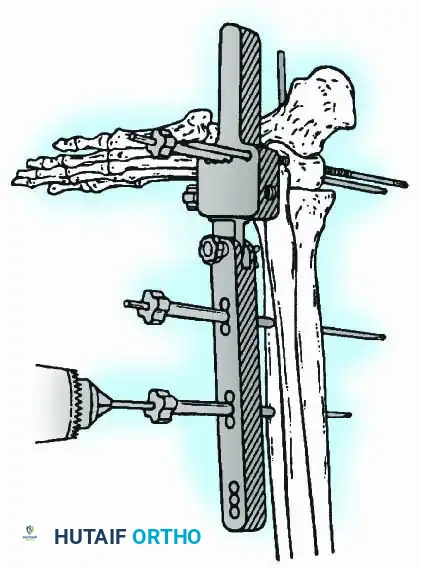
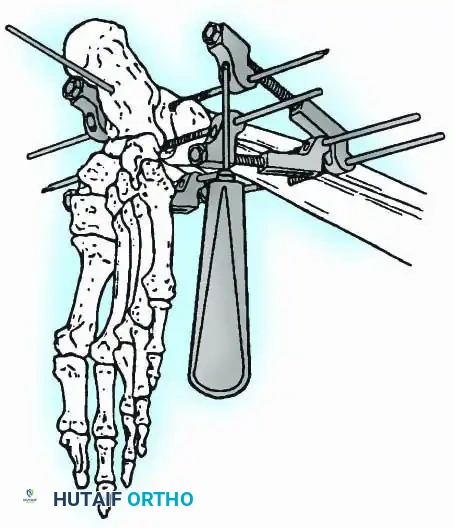
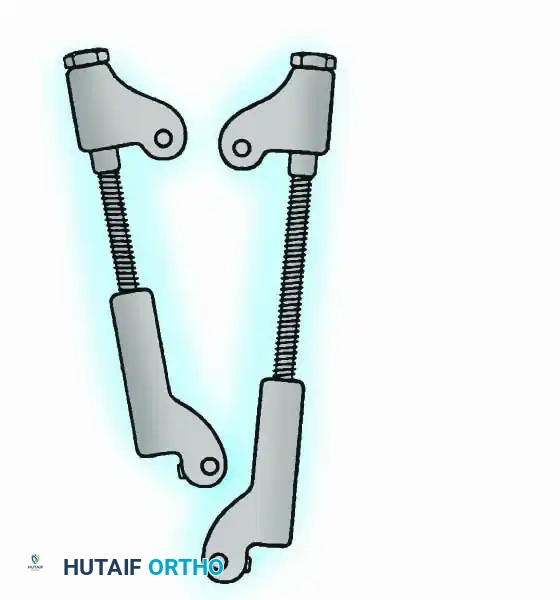
Historically pioneered by Charnley, external compression arthrodesis utilizes pins placed through the distal tibia and the body of the talus. Because Charnley's original uniplanar device lacked rotatory stability, Calandruccio designed a triangular frame to control motion in all three planes while applying massive compression.
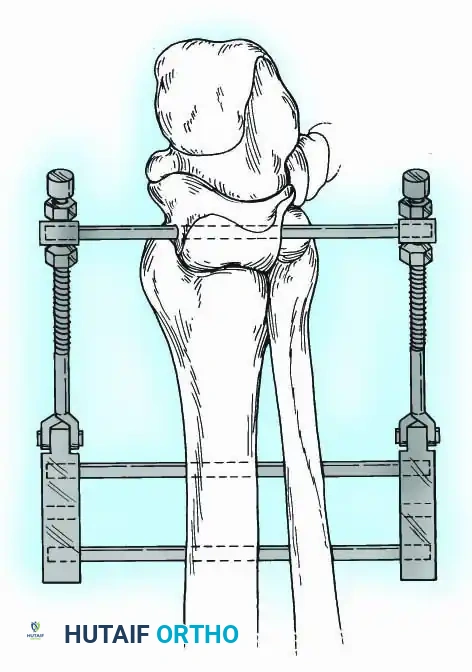
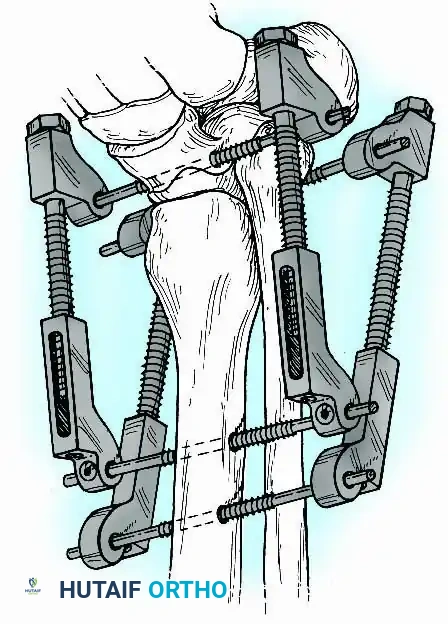
Modern iterations, such as the Calandruccio II compression device, offer greater latitude in pin placement to avoid compromised skin. Ring or circular external fixators (Ilizarov, Taylor Spatial Frame) are the gold standard for salvage situations, including active infection, massive bone loss, or failed TAA, as they allow for simultaneous compression, deformity correction, and early weight-bearing.
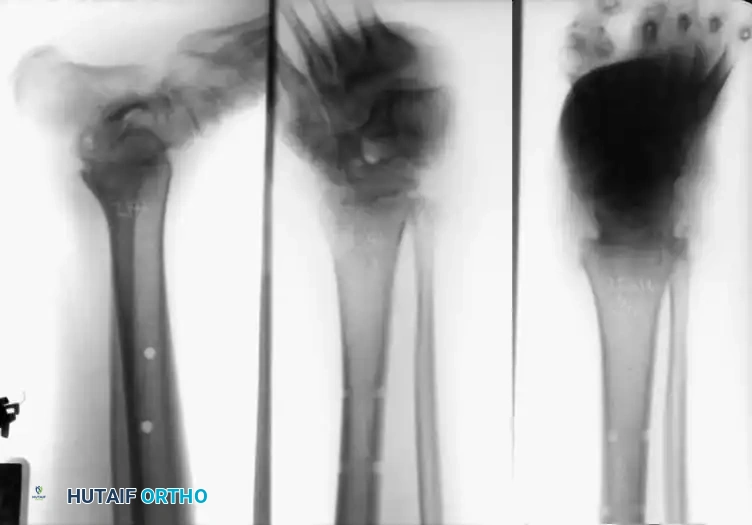
Internal Fixation
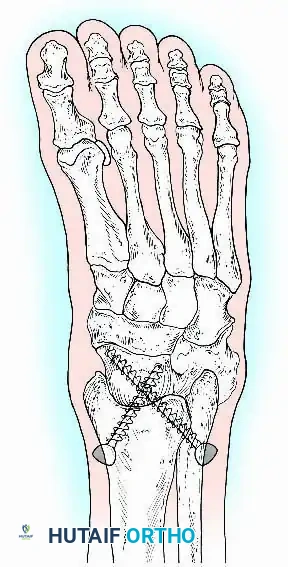
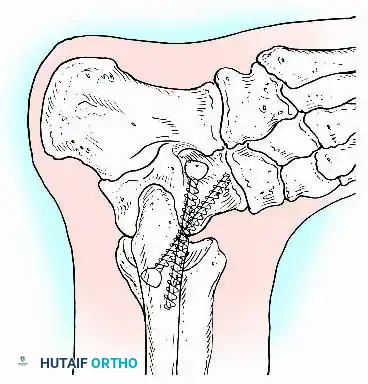
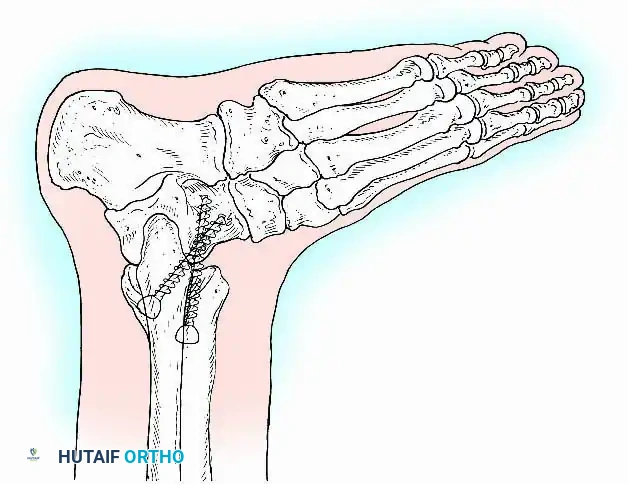
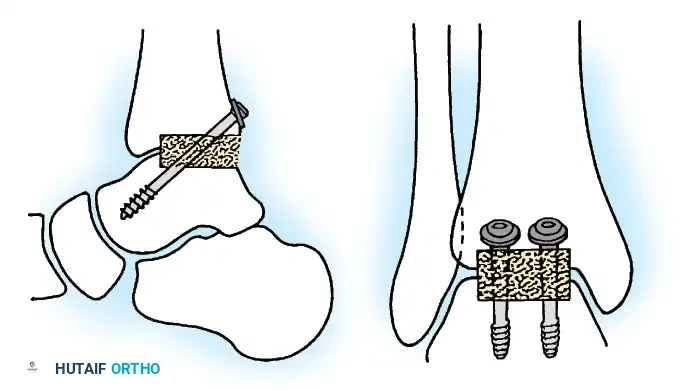
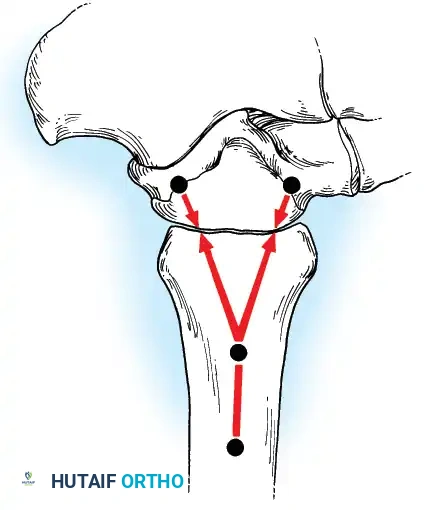
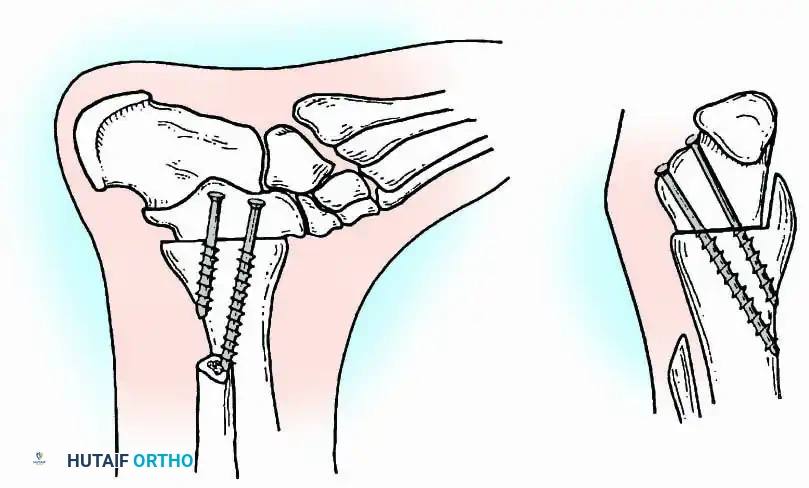
Internal fixation is currently the preferred method for uncomplicated ankle arthrodesis due to higher union rates, superior patient comfort, and the elimination of pin-tract infections. Biomechanical studies demonstrate that crossed, large-diameter (6.5 mm or 7.3 mm) cannulated cancellous screws provide exceptional resistance to shear and torsional forces.
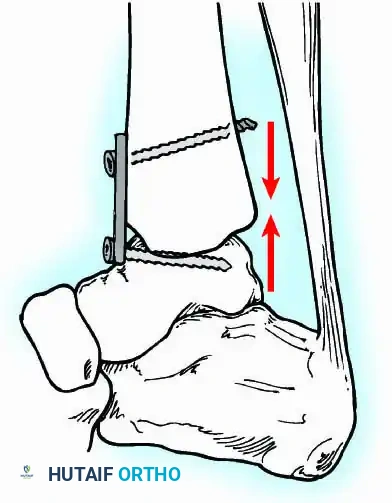
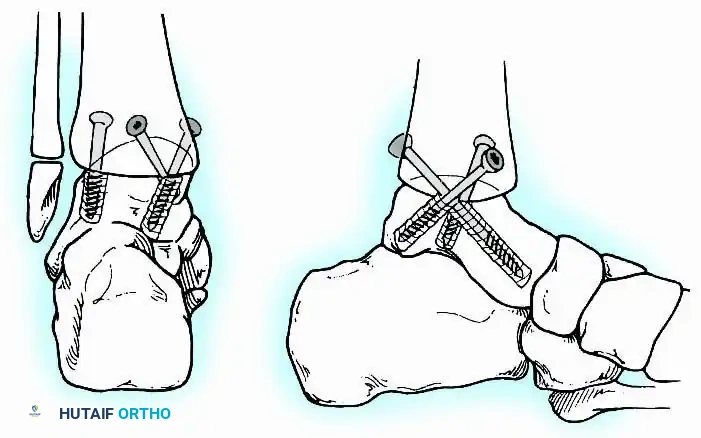
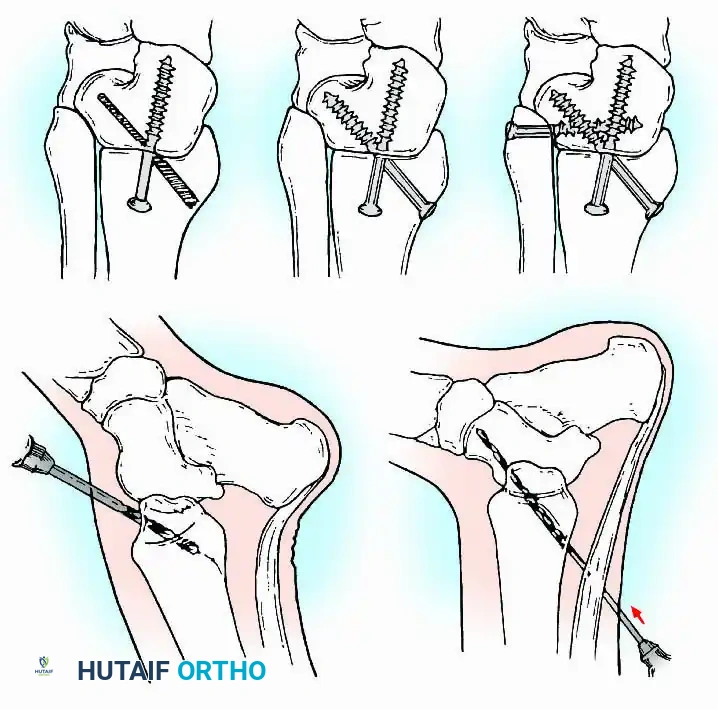
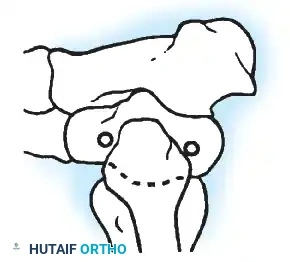
A standard construct involves two or three screws:
1. A "home run" screw directed from the posterior malleolus into the anterior neck of the talus.
2. A screw from the medial malleolus into the lateral body of the talus.
3. A screw from the anterolateral tibia into the medial talar body.
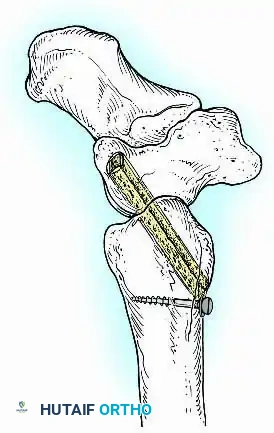
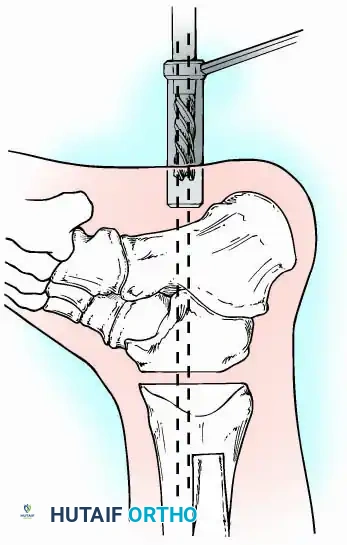
In cases of severe osteopenia or when extending the fusion to the subtalar joint (Tibiotalocalcaneal Arthrodesis), retrograde intramedullary nailing provides a load-sharing construct with superior bending stiffness.

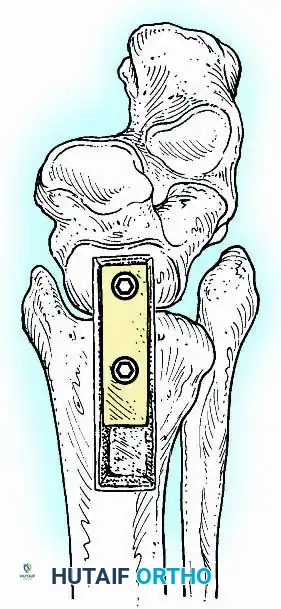
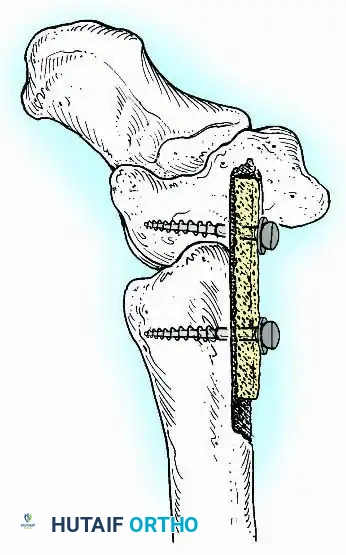
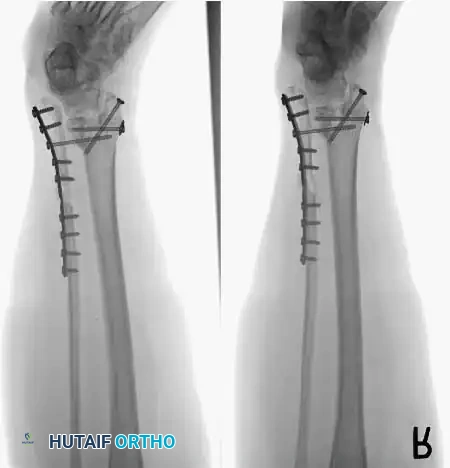
For complex hindfoot reconstructions, specialized plating systems, including anterior or lateral locking plates, can be utilized to supplement screw fixation, particularly when structural allografts are required to restore limb length.



Knee Arthrodesis
While total knee arthroplasty (TKA) is the definitive treatment for knee osteoarthritis, knee arthrodesis remains a critical salvage procedure. The primary indications are a chronically infected TKA that has failed two-stage revision, massive extensor mechanism disruption, severe neuropathic arthropathy, and tumor resection.
Positioning and Technique
The optimal position for knee arthrodesis is 10 to 15 degrees of flexion and 5 to 7 degrees of valgus. This slight flexion assists in foot clearance during the swing phase of gait and makes sitting in confined spaces more manageable. A perfectly straight (0 degrees) knee is cosmetically awkward and functionally detrimental, causing a vaulting gait pattern.



📚 Medical References
- joint arthrodesis utilizing anterior compression plate fi xation, J Arthroplasty 9:171, 1994.
- Brittain HA: Ischiofemoral arthrodesis, Br J Surg 29:93, 1941.
- Brittain HA: Ischio-femoral arthrodesis, J Bone Joint Surg 30B:642, 1948.
- Callaghan JJ, Brand RA, Pedersen DR: Hip arthrodesis: a longterm follow-up, J Bone Joint Surg 67A:1328, 1985.
- Carnesale PG: Arthrodesis of the hip: a long-term study, Orthop Digest 4:12, 1976.
- Chandler FA: Hip-fusion operation, J Bone Joint Surg 15:947, 1933.
- Charnley J: Stabilisation of the hip by central dislocation. In Proceedings of the British Orthopaedic Association, May 1955, J Bone Joint Surg 37B:514, 1955 (abstract). Davis JB: The muscle-pedicle bone graft in hip fusion, J Bone Joint Surg 36A:790, 1954.
- Davis JB, Fagan TE, Beals RK: Follow-up notes on articles previously published in the journal: muscle-pedicle bone graft in hip fusion, J Bone Joint Surg 53A:1645, 1971.
- Duncan CP, Spahgehl M, Beauchamp C, et al: Hip arthrodesis: an important option for advanced disease in the young adult, Can J Surg 38(suppl 1):39, 1995.
- Freiberg JA: Experiences with the Brittain ischio-femoral arthrodesis, J Bone Joint Surg 28:501, 1946.
- Ghormley RK: Use of the anterior superior spine and crest of ilium in surgery of the hip joint, J Bone Joint Surg 13:784, 1931.
- Gill AB: Arthrodesis for ununited fracture of the neck of the femur, J Bone Joint Surg 21:710, 1939.
- Girdlestone GR: Arthrodesis and other operations for tuberculosis of the hip. In Robert Jones Birthday Volume, London, 1928, Oxford University Press. Greiss MD, Thomas RJ, Freeman MA: Sequelae of arthrodesis of the hip, J Roy Soc Med 73:497, 1980.
- Heusner: Resektion in einem Fall von angeborener Hüftluxation, Zentralbl Chir vol 45, 1884.
- Hibbs RA: A preliminary report of twenty cases of hip joint tuberculosis treated by an operation devised to eliminate motion by fusing the joint, J Bone Joint Surg 8:522, 1926.
- King D: Arthrodesis of the adult nontuberculous hip, Stanford Med Bull 13:381, 1955.
- Kirkaldy-Willis WH: Ischio-femoral arthrodesis of the hip in tuberculosis: an anterior approach, J Bone Joint Surg 32B:187, 1950.
- Kirkaldy-Willis WH, Chaudhri MR, Anderson RJD: Arthrodesis of the hip with staple fi xation, J Bone Joint Surg 40A:114, 1958.
- Klemme WR, James P, Skinner SR: Results of hip arthrodesis in adolescents by using the cobra-head plate for internal fi xation, J Pediatr Orthop 18:648, 1998.
- Kocher T: Textbook of operative surgery , London, 1911, A&C Black. Kostuik J, Alexander D: Arthrodesis for failed hip arthroplasty, Clin Orthop Relat Res 188:173, 1984.
- Kreder HJ, Williams JI, Jaglal S, et al: A population study in the province of Ontario of the complications after conversion of hip or knee arthrodesis to total joint replacement, Can J Surg 42:433, 1999.
- Küntscher G: Practice of intramedullary nailing, Springfi eld, Ill, 1967, Charles C Thomas. Maragliano D: Nuovi punti di appoggio chirurgico nelle lussazione vere da coxite, Chir Organi Mov 5:225, 1921.
- Mayer L: Critique of Brittain operation for fusion of the hip, Bull Hosp Jt Dis 9:4, 1948.
- McKee GK: Arthrodesis of the hip with a lagscrew, J Bone Joint Surg 39B:477, 1957.
- Moore AT: Orthopaedic Correspondence Club Letter, May 1948.
- Morris JB: Charnley compression arthrodesis of the hip, J Bone Joint Surg 48B:260, 1966.
- Mowery CA, Houkom JA, Roach JW, et al: A simple method of hip arthrodesis, J Pediatr Orthop 6:7, 1986.
- Murrell GA, Fitch RD: Hip fusion in young adults, using a medial displacement osteotomy and cobra plate, Clin Orthop Relat Res 300:147, 1994.
- Pagnano MW, Cabanela ME: The hip: arthrodesis. In Morrey BF, ed: Reconstructive surgery of the joints , 2nd ed, New York, 1996, Churchill Livingstone. Perugia L, Santori FS, Mancini A, et al: Conversion of the arthrodesed hip to a
You Might Also Like