Complex Forearm Reconstruction: Radial Shaft Resection and Malunion Osteotomy

Key Takeaway
Forearm malunions significantly impair pronation and supination, often requiring corrective osteotomy and compression plating. Resection of the proximal radial shaft is a specialized technique utilized for proximal radioulnar synostosis. This comprehensive guide details the biomechanical principles, surgical indications, step-by-step Kocher approach, and rigorous postoperative rehabilitation protocols necessary to restore optimal forearm kinematics and grip strength in adult patients.
INTRODUCTION TO COMPLEX FOREARM RECONSTRUCTION
The human forearm functions as a highly complex, articulated ring, relying on the precise anatomical relationship between the radius and the ulna to facilitate fluid pronation and supination. The radius must rotate seamlessly around the stationary ulna, a mechanical action heavily dependent on the preservation of the interosseous space and the anatomical magnitude of the radial bow.
When this delicate biomechanical relationship is disrupted—either through the formation of a proximal radioulnar synostosis or via the malunion of diaphyseal fractures—patients experience profound functional deficits. Loss of rotational motion, compromised grip strength, and secondary arthrosis of the distal radioulnar joint (DRUJ) or proximal radioulnar joint (PRUJ) are common sequelae.
This comprehensive surgical guide details two advanced reconstructive procedures: the resection of the proximal radial shaft for the treatment of synostosis (as described by Kamineni et al.), and the corrective osteotomy and compression plating of adult forearm malunions.
PART I: RESECTION OF THE PROXIMAL PART OF THE RADIAL SHAFT
Proximal radioulnar synostosis is a debilitating complication that completely abolishes forearm rotation. It may occur congenitally or secondary to severe trauma, such as Monteggia fractures, radial head fractures with associated ulnar shaft fractures, or aggressive surgical dissection that breaches the interosseous membrane. Resection of a segment of the proximal radial shaft is a salvage procedure designed to restore rotation by physically uncoupling the radius from the ulna and interposing biological barriers to prevent recurrence.
Surgical Anatomy and Biomechanics
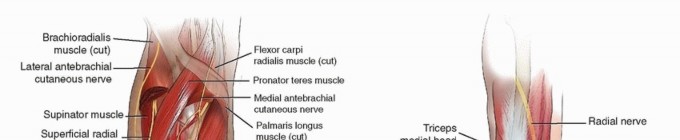
The surgical approach to the proximal radius requires navigating the interval between the anconeus and the extensor carpi ulnaris (ECU)—the classic Kocher approach. The primary anatomical hazard during this dissection is the posterior interosseous nerve (PIN), which courses through the supinator muscle. Elevating the supinator directly off the radius from ulnar to radial is critical to protecting the PIN.
⚠️ Surgical Warning: Posterior Interosseous Nerve (PIN)
The PIN is highly vulnerable during proximal radial exposures. Never place retractors blindly into the supinator muscle belly. Always elevate the supinator subperiosteally from the bone, reflecting it radially to keep the nerve safely encased within the muscle substance.
Patient Positioning and Setup
- Anesthesia: Administer general anesthesia to ensure complete muscle relaxation, which is vital for assessing intraoperative range of motion (ROM) after resection.
- Positioning: Place the patient in the supine position.
- Tourniquet: Apply a well-padded pneumatic tourniquet high on the brachium. Exsanguinate the limb and inflate the tourniquet to the appropriate pressure.
- Arm Placement: Bring the affected arm across the patient’s chest. This internally rotates the shoulder and presents the posterolateral aspect of the elbow and proximal forearm directly to the surgeon. Have a dedicated assistant stabilize the arm firmly in this position.
Step-by-Step Surgical Technique (Kamineni et al.)
- Incision and Approach: Make a standard Kocher approach to the proximal radius. Incise the skin obliquely from the lateral epicondyle extending distally over the posterolateral forearm.
- Deep Dissection: Identify the fascial interval between the anconeus (innervated by the radial nerve) and the extensor carpi ulnaris (innervated by the PIN).
- Exposure of the Synostosis: Once the interval is entered, direct the deep dissection toward the ulnar shaft and the site of the radioulnar synostosis.
- Supinator Elevation: Follow the synostosis to its distal margin. Carefully elevate the supinator muscle off the radius to expose the shaft while protecting the PIN.
- Bone Resection: Utilize an oscillating power saw under continuous saline irrigation to resect a precise 1-cm section of the radial shaft. The resection should be performed either proximal or distal to the bicipital tuberosity, dictated strictly by the anatomical extent of the synostosis.
- Kinematic Assessment: Following the resection, physically examine the range of motion of the forearm. If residual soft tissue contractures limit rotation, gently manipulate the forearm to break up minor adhesions.
- Biological Barrier Placement: To prevent the recurrence of heterotopic ossification and cross-union, cover the newly transected bone ends meticulously with bone wax. Bridge the 1-cm interval between the bone ends with an absorbable gelatin sponge (e.g., Gelfoam; Upjohn, Kalamazoo, MI).
- Closure: Deflate the tourniquet and secure meticulous hemostasis. Hematoma formation is a potent stimulus for recurrent synostosis. Close the deep fascia, subcutaneous tissue, and skin in anatomical layers over a single closed-suction drain.
Postoperative Rehabilitation Protocol
The success of a proximal radial resection relies heavily on aggressive, highly structured postoperative rehabilitation. Kamineni et al. developed a rigorous protocol utilizing continuous passive motion (CPM) and a specialized two-component splint.
- Immediate Postoperative Phase (0-48 Hours): Continuous passive motion (CPM) therapy is initiated immediately and utilized for the first 48 hours to prevent initial hematoma organization and adhesion formation.
- Splint Design: The patient is fitted with a custom two-component splint designed for static progressive pronation-supination. The first component spans from the upper arm to the forearm. The second component is an inner shell that wraps the distal forearm and wrist like a gauntlet. A Velcro strap connects the two, allowing the therapist or patient to dial in maximal attainable pronation or supination.
- Weeks 1 to 3 (The Intensive Phase):
- Night: Splint locked in full supination.
- Morning (Rising): Active and passive motion exercises for 1 hour.
- Morning to Noon: Splint locked in full pronation.
- Lunch: Splint removed for 1 hour of active use/exercises.
- Afternoon to Dinner: Splint locked in full supination.
- Dinner: Splint removed for 1 hour.
- Evening: Splint locked in full pronation.
- Pre-bedtime: Splint removed for 1 hour.
- Week 3 and Beyond: The periods during which the splint is removed are progressively increased based on clinical evaluation every 3 weeks.
- Long-Term Management: If maximal motion is not achieved by 3 months, the splint is worn exclusively at night in the position of greatest deficit (usually supination) until no further progress is documented.
PART II: SHAFTS OF THE RADIUS AND ULNA IN ADULTS (MALUNION CORRECTION)
Malunion of both-bone forearm fractures frequently results in functional deficits severe enough to warrant complex surgical correction. The forearm's ability to rotate is highly sensitive to angular deformities, malrotation, and the loss of the normal radial bow.
Pathoanatomy and Biomechanics of Forearm Malunion
The interosseous space between the radius and ulna must remain unobstructed to allow the radial tuberosity to clear the ulna during pronation.
- Angular Deformity: Cadaveric biomechanical studies demonstrate that a 10-degree angular deformity results in an insignificant reduction in forearm rotation. However, a 20-degree angulation predictably results in a severe loss of both pronation and supination.
- Total Deformity: When the total deformity across all planes reaches 15 degrees, overall forearm motion is reduced by more than 27% (with the exception of isolated distal-third fractures, which are slightly more forgiving).
- Radial Bow: The radius possesses a natural lateral bow that maximizes the interosseous space. Failure to restore the proper magnitude and location of the radial bow during initial fracture management directly correlates with reduced forearm rotation and diminished grip strength.
- Joint Arthrosis: Long-standing malunions alter the load-bearing mechanics of the forearm. Over time, this leads to disturbances of the distal radioulnar joint (DRUJ) and, in cases of long-standing malunion (>20 years), progressive osteoarthritis of the proximal radioulnar joint (PRUJ).
Clinical Evaluation and Indications for Surgery
The decision to perform a corrective osteotomy should never be based solely on the degree of radiographic deformity. It must be driven by the patient's functional limitations and physical demands.
Primary Indications for Corrective Osteotomy:
1. Clinically significant loss of pronation or supination that impairs activities of daily living.
2. Instability or painful impingement of the distal radioulnar joint (DRUJ).
3. Unacceptable cosmetic deformity (less common, but valid in severe cases).
💡 Clinical Pearl: Soft Tissue vs. Bony Block
Before indicating a patient for osteotomy, the surgeon must differentiate between a bony block (due to malunion) and soft tissue contracture (due to prolonged immobilization). Restoring proper skeletal alignment will not improve functional deficits caused primarily by severe interosseous membrane contracture.
Surgical Timing and Prognostic Factors
The timing of surgical intervention is the single most critical prognostic factor for functional recovery.
Operative treatment of forearm malunions is significantly more likely to improve forearm motion if performed within the first year after the initial injury. After 12 months, chronic soft tissue contractures, scarring of the interosseous membrane, and capsular contractures of the DRUJ/PRUJ severely limit the amount of motion that can be salvaged, even with perfect skeletal realignment.
In a landmark retrospective review by Trousdale and Linscheid of 27 patients treated at the Mayo Clinic:
* Early Intervention (< 12 months): Patients gained an average of 79 degrees of total rotation (range, 20 to 160 degrees). Complications were minimal (mild wrist pain, one superficial infection).
* Late Intervention (> 12 months): Patients gained an average of only 30 degrees of additional rotation (range, 25 to 95 degrees). Furthermore, the complication rate skyrocketed to 48%, including loss of motion, heterotopic ossification, delayed union, ulnar head subluxation, and refracture.
Similarly, Nagy et al. reported on 17 patients undergoing symptomatic malunion correction, noting that while all patients improved, those with a primary supination deficit experienced a much greater overall improvement range than those with a pronation deficit.
Surgical Technique: Corrective Osteotomy and Plating
Correction of a forearm malunion requires meticulous preoperative templating, precise osteotomies of one or both bones, correction of the deformity in all three planes (coronal, sagittal, and axial rotation), rigid compression plating, and autologous bone grafting.
Preoperative Radiographic Assessment
Figure A: Preoperative anteroposterior and lateral radiographs demonstrating a severe malunion of the radial shaft and a hypertrophic nonunion of the ulnar shaft. Note the complete loss of the radial bow and the encroachment upon the interosseous space.
Operative Steps
- Surgical Approach:
- For the radius: Utilize a volar Henry approach for middle and distal third malunions, or a dorsal Thompson/Kocher approach for proximal third malunions.
- For the ulna: Utilize a direct subcutaneous approach along the ulnar crest.
- Exposure and Release: Expose the malunion site subperiosteally. Release contracted soft tissues, taking care to preserve the vascularity of the surrounding periosteum.
- Osteotomy: Perform the osteotomy at the apex of the deformity using an oscillating saw. Depending on the preoperative template, an opening wedge, closing wedge, or step-cut osteotomy may be utilized to correct angulation and restore length.
- Restoring the Radial Bow: The radius must be rotated and angulated to recreate the anatomical lateral bow. This is often the most technically demanding portion of the procedure.
- Internal Fixation: Apply heavy-duty 3.5mm dynamic compression plates (LC-DCP) or locking compression plates (LCP). The plates must be pre-contoured to match the restored anatomy of the radius and ulna. Achieve absolute stability through axial compression.
- Bone Grafting: Because corrective osteotomies often create structural gaps (especially opening wedge corrections), autologous cancellous or corticocancellous bone graft harvested from the iliac crest is mandatory to stimulate osteogenesis and prevent delayed union.
Postoperative Radiographic Assessment
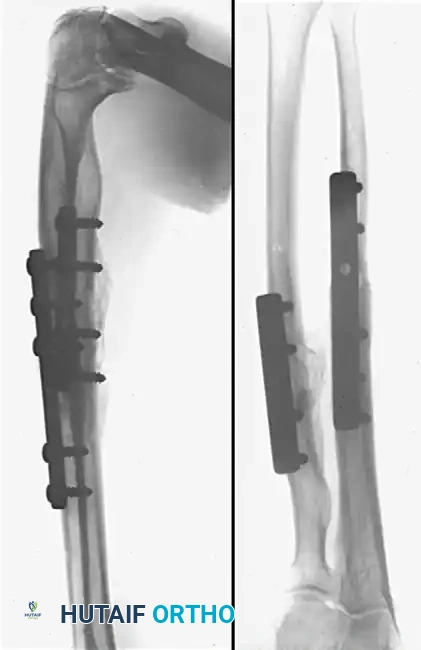
Figure B: Postoperative radiographs taken 6 months after corrective osteotomy. Solid union has been achieved with normal skeletal alignment. The radius and ulna have been rigidly fixed with 3.5mm compression plates, and the structural defects were successfully managed with autologous iliac crest bone grafts. The interosseous space and radial bow are fully restored.
Complications of Malunion Surgery
Patients must be thoroughly counseled regarding the high-risk nature of forearm reconstructive surgery. Potential complications include:
* Delayed Union and Nonunion: The diaphyseal bone of the forearm has a tenuous blood supply, exacerbated by previous trauma and secondary surgical stripping.
* Infection: Deep surgical site infections require aggressive debridement and potential hardware removal.
* Neurological Injury: Radial nerve (PIN) paresthesias or palsies can occur during radial exposures.
* Hardware Prominence: Plates on the subcutaneous border of the ulna or the distal radius may cause tendinopathy or require eventual removal.
* Persistent DRUJ Instability: If the malunion is long-standing, restoring diaphyseal anatomy may not resolve chronic ligamentous laxity at the DRUJ, necessitating secondary procedures such as ulnar shortening osteotomy or ligament reconstruction.
CONCLUSION
The management of complex forearm pathology, whether it be a proximal radioulnar synostosis or a diaphyseal malunion, requires a profound understanding of forearm kinematics. Resection of the proximal radial shaft combined with aggressive, protocol-driven splinting offers a viable salvage pathway for synostosis. Conversely, corrective osteotomy for forearm malunion is a highly effective procedure for restoring rotation and grip strength, provided it is executed with rigid compression plating, autologous bone grafting, and crucially, performed within the first year following the initial injury.
You Might Also Like