Barsky Technique for Cleft Hand Closure: A Comprehensive Surgical Guide
Key Takeaway
The Barsky technique for cleft hand closure is a foundational orthopedic procedure designed to restore both function and aesthetics in central ray deficiencies. By utilizing a distally based, diamond-shaped flap and precise metacarpal approximation, surgeons can reconstruct the commissure while minimizing contracture risk. This guide details the step-by-step surgical approach, biomechanical considerations, and postoperative protocols essential for optimal outcomes in pediatric hand reconstruction.
Introduction to Central Ray Deficiency and Cleft Hand
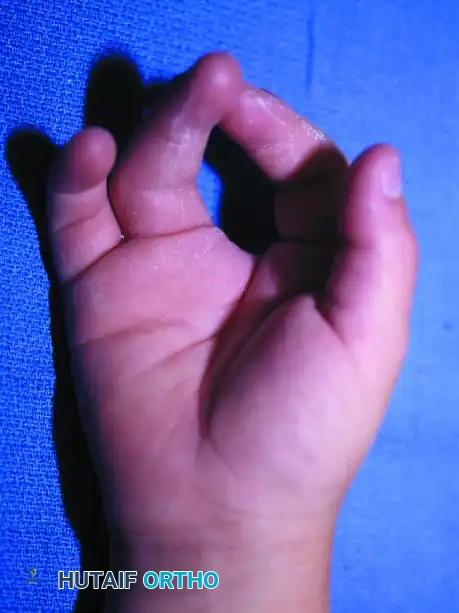
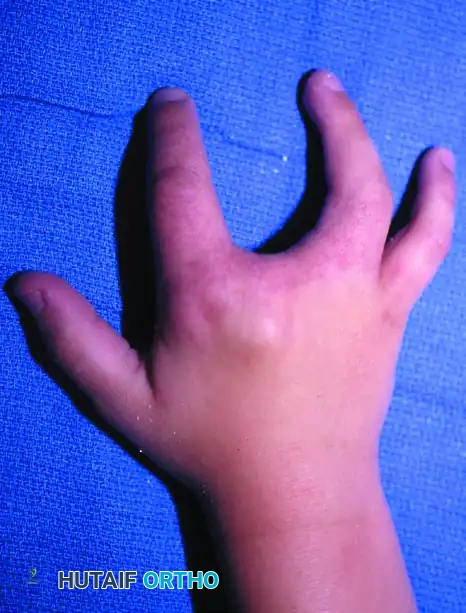
Central ray deficiency, commonly referred to as "cleft hand" or "split hand," is a complex congenital anomaly characterized by the absence of central digits and metacarpals, resulting in a V-shaped cleft. This failure of formation disrupts the normal transverse arch of the hand and eliminates the deep transverse metacarpal ligament, leading to progressive divergence of the adjacent metacarpals.
The primary goals of surgical intervention are to restore functional pinch and grasp, close the central defect, reconstruct a stable commissure, and improve the overall aesthetic appearance of the hand. The Barsky Technique remains a cornerstone in the operative management of typical cleft hands, utilizing a meticulously designed distally based flap to recreate the web space while physically approximating the divergent metacarpals.


Preoperative Evaluation and Classification
Surgical decision-making in cleft hand reconstruction is heavily dictated by the status of the first web space (the thumb web). A narrowed or absent thumb web space severely limits opposition and grasp, taking precedence over the central cleft closure itself.
The Manske and Halikis Classification (1995) is the internationally accepted standard for categorizing central deficiencies based on the thumb web space, guiding the appropriate surgical strategy.
Manske and Halikis Surgical Classification
- Type I: Normal Thumb Web Space
- Characteristics: No narrowing of the first web space.
- Surgical Recommendations: Cleft closure with local tissue reduction of the intermetacarpal space. Techniques include circumferential tendon grafting, local tissue attachment to metacarpal heads (index to middle metacarpal transposition), and excision of polydactylous bony ossicles when present.
- Type IIA: Mildly Narrowed Thumb Web Space
- Characteristics: Mild contracture or narrowing.
- Surgical Recommendations: Local pedicle flaps (e.g., Z-plasty) to widen the first web space, combined with the cleft closure techniques noted in Type I.
- Type IIB: Moderately Narrowed Thumb Web Space
- Characteristics: Moderate contracture requiring more than local Z-plasties.
- Surgical Recommendations: Dorsal/volar pedicle flaps mobilized from the cleft skin to reconstruct the thumb web, supplemented with skin grafts as needed, alongside standard cleft closure.
- Type III: Severely Narrowed Thumb Web Space
- Characteristics: Severe syndactyly or contracture of the first web.
- Surgical Recommendations: Syndactyly release utilizing skin grafts and dorsal/volar pedicle flaps from the cleft. Alternatively, excision of the index bony elements may be required to create a functional first web space.
- Type IV: Merged Web and Cleft
- Characteristics: The thumb web space is obliterated, and the cleft functions as the primary web space.
- Surgical Recommendations: No formal cleft closure is performed, as the cleft serves as the functional web. Tissue reduction with metacarpophalangeal (MCP) stabilization may be considered.
- Type V: Absent Thumb Web Space
- Characteristics: Complete absence of the thumb web, often with severe hypoplasia.
- Surgical Recommendations: Cleft closure is contraindicated. Consider toe-to-hand transfer or metacarpal lengthening to restore fundamental grasp mechanics.
💡 Clinical Pearl: The Deforming Force
In cleft hand anomalies, the absence of the deep transverse metacarpal ligament allows the intrinsic muscles and mechanical forces of use to splay the border digits. Identifying and excising anomalous transverse bones (cross-bones) or tight fibrous bands within the cleft is critical before attempting metacarpal approximation.
Surgical Technique: The Barsky Cleft Closure
The Barsky technique is highly effective for Type I and mild Type II anomalies. It relies on a distally based diamond flap to create a natural, sloping commissure that resists dorsal migration (web creep) over time.
1. Patient Positioning and Preparation
The procedure is performed under general anesthesia. The patient is positioned supine with the affected extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the upper arm. Exsanguination is achieved via elevation or an Esmarch bandage, and the tourniquet is inflated to an age- and weight-appropriate pressure (typically 200-250 mmHg). Loupe magnification (2.5x to 3.5x) is highly recommended for meticulous dissection of the neurovascular bundles.
2. Flap Design and Incision
Precise preoperative marking is the most critical step in preventing postoperative contractures.
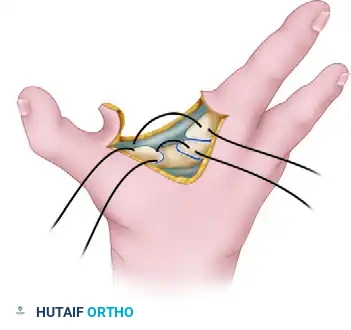
- The Diamond Flap: Mark a distally based, diamond-shaped flap on one side of the opposing surfaces of the involved fingers (typically the more mobile or redundant side).
- Positioning: Place the flap slightly dorsally. This dorsal bias is essential to allow for a gentle, natural volar slope of the reconstructed commissure.
- Dimensions: The base of the flap should be approximately 1 cm wide, and the length should be 1.5 times longer than the width.
Under tourniquet control, sharply elevate the flap.
⚠️ Surgical Warning: Defatting the Flap
The flap must be defatted down to the subdermal vascular plexus. Failure to defat the flap will result in a bulky, unnatural web space. However, aggressive defatting that violates the subdermal plexus will lead to partial or complete flap necrosis. Maintain a meticulous plane just deep to the dermis.
Once the flap is elevated, make a continuous incision from the free end of the flap proximally along the opposing surfaces of the V-shaped cleft, extending toward the apex.
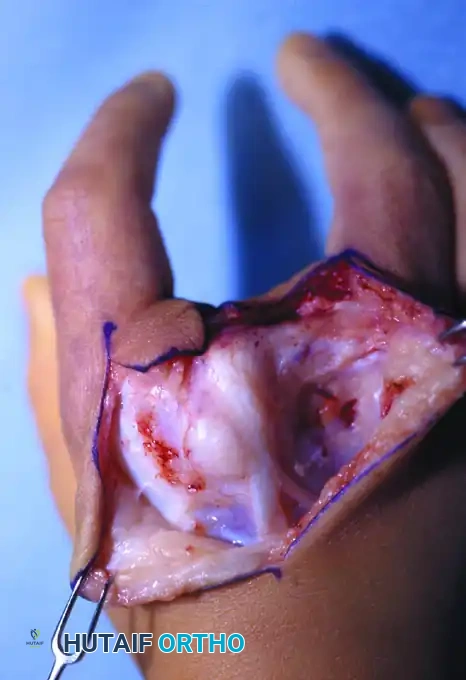
3. Deep Exposure and Extraperiosteal Dissection
Deepen the incision through the subcutaneous tissues, carefully identifying and protecting the digital neurovascular bundles. The neurovascular structures in cleft hands often exhibit anomalous branching patterns; trace them proximally to ensure they are not tethered or at risk during metacarpal approximation.
Expose the divergent metacarpals extraperiosteally.
- Why Extraperiosteal? In pediatric patients, stripping the periosteum can damage the physis or lead to unpredictable bony overgrowth and synostosis. Maintaining an extraperiosteal plane preserves the vascular supply to the bone and protects future growth potential.
- Tissue Excision: Radically excise any excess soft tissue, anomalous intrinsic muscle bellies, fibrous bands, or polydactylous bony elements (transverse ossicles) that reside within the cleft. These elements act as a mechanical block; if they are not removed, apposing the metacarpals will be impossible or will place undue tension on the repair.
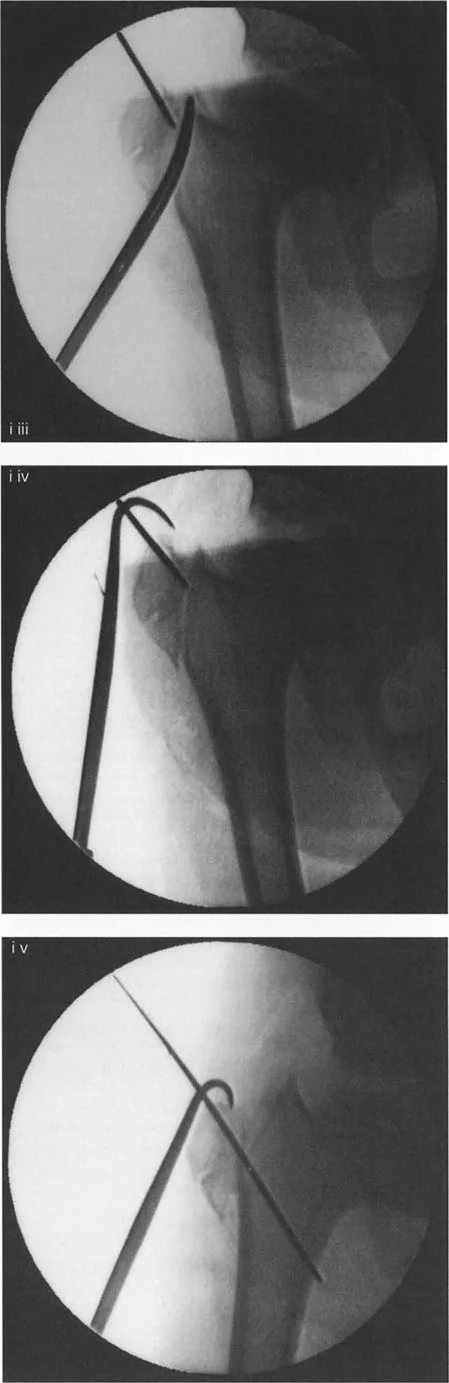
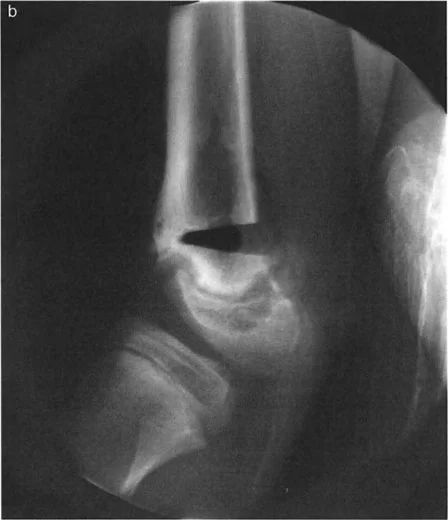
4. Metacarpal Approximation
To restore the transverse metacarpal arch, the divergent metacarpals must be physically tethered.
- Using a fine K-wire or a small drill bit, drill two holes in each of the opposing metacarpals just proximal to the metacarpal heads.
- Pass a heavy, non-absorbable suture (e.g., 0 or 2-0 braided polyester or polypropylene, depending on the child's size) through the holes in a figure-of-eight or horizontal mattress configuration.
- Manually approximate the metacarpals to close the cleft space. While holding the bones in their reduced position, tie the heavy suture securely. This step effectively substitutes for the absent deep transverse metacarpal ligament.
💡 Clinical Pearl: Augmenting the Repair
In older children or cases with severe divergence, a simple heavy suture may eventually cut through the bone or stretch. In such instances, consider augmenting the closure with a circumferential tendon graft (e.g., using a slip of the extensor carpi radialis longus or palmaris longus) woven through the metacarpal necks.
5. Soft Tissue Reconstruction and Closure
With the skeletal architecture restored, attention is turned to the soft tissue envelope. Closing a linear incision in the web space is strictly contraindicated, as it will inevitably lead to a longitudinal scar contracture and recurrent web creep.
- Interdigitating Flaps: Close the dorsal and palmar skin incisions from proximal to distal. As you proceed distally, excise excess skin in a geometric pattern to create interdigitating flaps (Z-plasties or W-plasties) along both the dorsal and palmar surfaces. This breaks up the linear scar line.

- Commissure Inset: Bring the distally based diamond finger flap across the newly approximated space and inset it into the commissure.
- Managing Redundancy: Because the cleft has been closed, there will be redundant skin. Crucial Step: Before suturing the flap into its final position, excise any excess skin from the dorsum of the hand, rather than trimming the flap itself. Trimming the flap risks compromising its precise dimensions and delicate vascular supply.


Ensure all skin edges are approximated with fine absorbable sutures (e.g., 5-0 or 6-0 chromic gut or fast-absorbing plain gut) to avoid the need for suture removal in a pediatric patient.
Postoperative Care and Rehabilitation
The success of the Barsky cleft closure relies heavily on strict postoperative immobilization to allow the heavy metacarpal sutures and soft tissues to heal without tension.
Casting Protocol
- Immediately postoperatively, apply a sterile, non-adherent dressing with a minimal amount of bulky bandages to avoid excessive pressure on the flaps.
- Apply a well-molded, long-arm cast extending to the level of the metacarpal heads.
- Rationale for Long-Arm: In pediatric patients, a short-arm cast is easily slipped off or allows for excessive pronation/supination, which can translate forces to the healing metacarpals. A long-arm cast with the elbow at 90 degrees ensures absolute compliance and immobilization.
Timeline and Monitoring
- The initial cast is worn continuously for 3 to 4 weeks.
- At the 3-to-4-week mark, the cast is removed in the clinic, and the hand is carefully inspected.
- Assessing Stability: Evaluate the stability of the metacarpal approximation. If the thumb or border digits tend to separate excessively upon cast removal, the healing is insufficient. In this scenario, apply another well-molded cast for an additional 2 to 3 weeks.
- Once clinical stability is confirmed, the cast is discontinued, and the patient is allowed to resume regular use of the hand.
Rehabilitation
Due to the high adaptability of pediatric patients, formal occupational therapy or specialized hand therapy is usually not required following a standard Barsky closure. The child will naturally incorporate the reconstructed hand into daily play and activities, which serves as the best form of functional rehabilitation. However, parents should be instructed to perform gentle scar massage once the incisions are fully healed to optimize tissue pliability.
Complications and Pitfalls
While the Barsky technique is highly reliable, surgeons must be vigilant regarding potential complications:
- Flap Necrosis: Usually results from overly aggressive defatting that damages the subdermal plexus, or from excessive tension during inset. If superficial epidermolysis occurs, it can be managed with local wound care. Full-thickness necrosis may require secondary grafting.
- Recurrent Clefting (Divergence): Can occur if the heavy metacarpal suture breaks, cuts through osteopenic bone, or if anomalous transverse bony elements were left intact during the initial dissection.
- Web Creep: Distal migration of the commissure over time. This is mitigated by ensuring the diamond flap is placed slightly dorsally and by strictly avoiding straight-line longitudinal closures across the web space.
- First Web Space Contracture: If a Manske Type II or III deficiency is misdiagnosed as a Type I and the thumb web is not addressed simultaneously, the patient will have a cosmetically closed cleft but a functionally poor hand due to lack of opposition. Always prioritize the thumb web space.
You Might Also Like