Mastering Orthopaedic Trauma: Rehabilitation, External Fixation, and Infection Management

Key Takeaway
Postoperative rehabilitation in orthopaedic trauma requires a delicate balance between early joint mobilization and soft tissue preservation. The use of Ilizarov and spatial external fixators provides optimal biomechanical stability while allowing axial micromotion to promote osteogenesis. Managing postoperative complications, particularly MRSA infections, relies on aggressive debridement and strategic implant retention. Tailored weight-bearing protocols ensure optimal fracture union and functional recovery.
Introduction and Epidemiology
Gait, the complex process of bipedal locomotion, represents a fundamental aspect of human function and independence. From an orthopedic perspective, a comprehensive understanding of normal and pathological gait is paramount for diagnosing musculoskeletal and neurological disorders, planning interventions, and assessing rehabilitation outcomes. This discussion will delve into the intricate biomechanics of gait, the profound impact of amputations and neurological injuries, and the critical role of prostheses and orthoses in restoring function and optimizing patient mobility.
Definitions and Biomechanical Principles of Gait
Gait is an energy-efficient, dynamic process characterized by controlled, reciprocal lower limb movements designed to propel the body while maintaining upright stability. Key parameters define its quantitative characteristics:
1. Walking: An energy-efficient process of controlled, reciprocal lower limb movements used to move the body from one location to another while maintaining upright stability.
2. Coordination: One supporting foot is in contact with the ground at all times (single-limb support), with a period when both limbs are in contact with the ground (double-limb stance support).
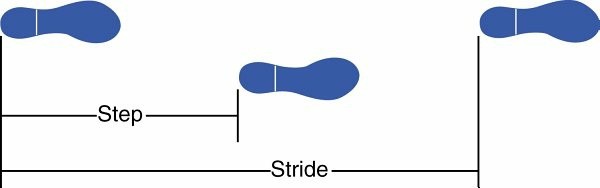
3. Step: The distance between successive initial contact by the two lower limbs.
4. Stride: The distance between successive initial contact by the same lower limb.
5. Velocity: The ratio of distance to time, typically measured in meters per second or feet per second.
6. Cadence: Steps per unit of time, often expressed as steps per minute.
7. Running: Differs from walking in that it precludes double-limb support/stance, incorporating a flight phase where neither limb is in contact with the ground.
Phases of the Gait Cycle
The normal gait cycle, defined as the interval between successive initial contacts of the same foot, is conventionally divided into two primary phases: Stance (60%) and Swing (40%).
Stance Phase
This phase commences when the foot makes initial contact with the ground and concludes when the same foot lifts off. It is further subdivided:
1. Initial Contact (IC): The precise instant the reference foot contacts the ground, typically with the heel.
2. Loading Response (LR): Starts immediately after IC and extends until the initial swing of the contralateral foot, accommodating weight transfer and shock absorption.
3. Midstance (MSt): Begins with initial swing of the advancing foot and concludes when the body's center of gravity (COG) is directly over the supporting forefoot.
4. Terminal Stance (TSt): Initiates with heel rise and persists until the initial contact of the contralateral foot, preparing for propulsion.
5. Preswing (PSw): Begins with IC of the contralateral limb and culminates when the reference stance foot lifts off the ground.
Swing Phase
This phase begins as the foot leaves the ground and ends just before initial contact of the same foot. It is also further subdivided:
1. Initial Swing (ISw): Commences when the foot leaves the ground and concludes when the swinging foot is directly opposite the stance foot.
2. Midswing (MSw): Extends from the end of ISw until the swinging limb is forward with the tibia approximately vertical to the ground.
3. Terminal Swing (TSw): Spans the period from vertical tibia position to the instant of initial ground contact, preparing the limb for weight acceptance.
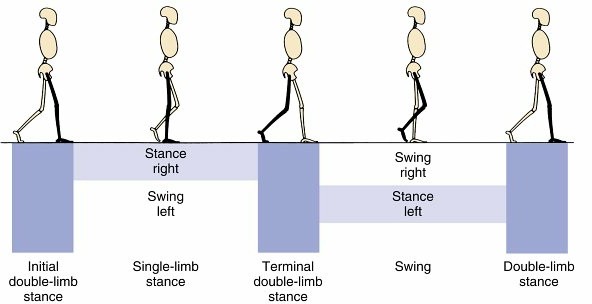
FIG. 10.1: Subdivisions of gait and bilateral limb support patterns are critical for understanding normal and pathological locomotion.
Epidemiology of Gait Disorders and Amputations
Gait abnormalities are prevalent, affecting a significant portion of the population, particularly the elderly and individuals with musculoskeletal or neurological impairments. Common causes include osteoarthritis, peripheral neuropathy, stroke, Parkinson's disease, and traumatic injuries.
Lower limb amputations, while life-saving, represent a profound disruption to gait and function. The epidemiology varies globally, but common etiologies include:
* Vascular Disease: Predominantly diabetes-related complications and peripheral arterial disease, accounting for 70-80% of all non-traumatic lower extremity amputations in developed countries.
* Trauma: Accounts for 10-20% of amputations, often involving younger individuals.
* Malignancy: Primary bone or soft tissue tumors (e.g., osteosarcoma, synovial sarcoma) necessitate amputation in 5-10% of cases.
* Infection: Severe, uncontrolled infections like necrotizing fasciitis or osteomyelitis.
* Congenital Limb Deficiency: A smaller but distinct group requiring prosthetic management from an early age.
The rehabilitation challenges associated with these conditions necessitate a multidisciplinary approach, with orthopedic surgeons playing a pivotal role in optimizing surgical outcomes that facilitate subsequent prosthetic or orthotic management and functional restoration.
Surgical Anatomy and Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the lower limb is indispensable for orthopedic surgeons managing conditions affecting gait, especially in the context of amputation, prosthetic fitting, orthotic prescription, and neurological injury.
Anatomy for Amputation Levels
Each amputation level presents unique anatomical considerations influencing surgical technique, wound healing, prosthetic fit, and rehabilitation potential.
Foot Amputations
- Toe Amputations: Preserve metatarsal head. Critical for push-off phase of gait.
- Transmetatarsal Amputations: Preserve significant foot length for better balance and prosthetic toe fillers. Preserve intrinsic muscles if possible.
- Lisfranc (Tarsometatarsal) Amputations: Loss of forefoot, creating significant lever arm disadvantage. Requires robust prosthetic shoe filler.
- Chopart (Talonavicular and Calcaneocuboid) Amputations: More severe loss, often leading to equinus deformity due to unopposed Achilles tendon. Myodesis of anterior tibialis and extensor tendons to talar neck or calcaneus can prevent this.
- Syme Amputation (Ankle Disarticulation): Preserves calcaneal heel pad and distal tibia/fibula articular surfaces, providing excellent weight-bearing surface. Requires careful shaping of malleoli. Main challenge is prosthetic cosmesis and bulk.
Transtibial (Below-Knee) Amputations
This is the most common lower extremity amputation, aiming for residual limb length between 12.5 to 17.5 cm from the knee joint line for optimal prosthetic fit.
* Vascular Supply: Popliteal artery bifurcates into anterior and posterior tibial arteries. Preservation of robust posterior flap often relies on posterior tibial artery perforators.
* Nerves: Common peroneal nerve (superficial and deep branches) and sural nerve, saphenous nerve, tibial nerve. These must be identified, gently stretched, sharply transected high proximally, and allowed to retract into soft tissue to minimize neuroma formation.
* Muscles: Myodesis or myoplasty is critical. The gastrocnemius-soleus complex provides the primary posterior muscle flap. Myodesis of the gastrocnemius to the anterior tibia or fibula creates a stable, well-padded distal stump. Anterior compartment muscles (tibialis anterior, extensors) are typically transected and may be beveled.
* Bone: Tibia and fibula. The tibia requires careful beveling of the anterior crest and smoothing of cut edges. The fibula is typically cut 1-2 cm shorter than the tibia to prevent distal pressure points.

FIG. 10.2: Anatomical considerations for transtibial amputation, highlighting key neurovascular structures and bone cuts.
Transfemoral (Above-Knee) Amputations
- Vascular Supply: Femoral artery and vein, deep femoral artery and vein. Ligation must be secure.
- Nerves: Femoral nerve, obturator nerve, sciatic nerve (largest nerve). All require careful identification, sharp transection, and retraction. The sciatic nerve is particularly prone to neuroma formation due to its size.
- Muscles: Adductor magnus, hamstrings, quadriceps. Myodesis of the adductor magnus to the lateral femur provides critical medial padding and helps prevent abduction contracture. Quadriceps and hamstrings are also managed for optimal muscle balance and prosthetic control.
- Bone: Femur. Optimal length is typically 25-30 cm from the greater trochanter. Beveling of the distal femur is performed.
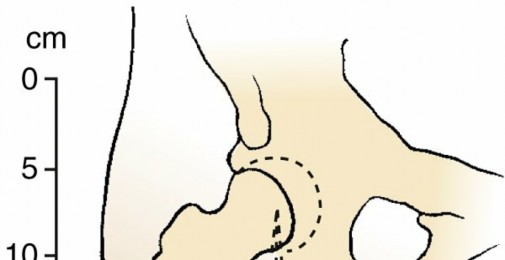
Hip Disarticulation and Hemipelvectomy
These are rare, complex procedures requiring extensive dissection and pose significant challenges for prosthetic ambulation due to loss of major pelvic stabilizers and long lever arms.
Biomechanics of Gait and Pathological Alterations
Normal gait relies on a coordinated interplay of joint motion, muscle activity, and ground reaction forces.
* Kinematics: Describes joint angles and movements (e.g., knee flexion-extension, ankle dorsiflexion-plantarflexion).
* Kinetics: Analyzes forces causing motion (e.g., muscle forces, ground reaction forces).
Key Biomechanical Principles
- Shock Absorption: Achieved primarily through knee flexion and ankle plantarflexion during loading response.
- Stance Stability: Maintained by precise muscle activation (e.g., gluteus medius for pelvic stability, quadriceps for knee stability).
- Propulsion: Generated by ankle plantarflexion (gastrocnemius-soleus) during preswing/terminal stance.
- Limb Clearance: Achieved by knee flexion and ankle dorsiflexion during swing phase.
Pathological Gait Biomechanics
Disruptions to this intricate system, whether from amputation, neurological injury, or orthopedic deformity, lead to compensatory strategies and altered biomechanics.
* Amputee Gait:
* Transtibial: Decreased stance phase on prosthetic limb, increased energy expenditure, potential for prosthetic knee hyperextension, inadequate push-off. Pelvic obliquity, circumduction.
* Transfemoral: Significant energy expenditure increase, reliance on hip musculature for prosthetic control, potential for Trendelenburg gait, vaulting.
* General Amputee: Altered center of gravity, decreased balance, reliance on visual and somatosensory input.
* Neurological Gait (e.g., Stroke, Cerebral Palsy, SCI):
* Spasticity: Equinus foot, knee hyperextension, scissoring gait.
* Weakness: Foot drop (steppage gait), genu recurvatum, Trendelenburg.
* Ataxia: Wide-based, unsteady gait.
* Sensory Deficits: Increased step width, decreased balance.
Understanding these biomechanical alterations is crucial for selecting appropriate surgical interventions, designing effective prostheses and orthoses, and implementing targeted rehabilitation programs.
Indications and Contraindications
The decision-making process for surgical interventions impacting gait, particularly amputation or corrective procedures for neurological injury, is complex and requires careful consideration of indications and contraindications.
Indications
Amputation
- Irreversible Ischemia: Most common indication, typically due to peripheral arterial disease or diabetes with non-healing ulcers or gangrene.
- Unreconstructable Trauma: Severe limb trauma with extensive soft tissue loss, neurovascular compromise, or bone destruction beyond salvage (mangled extremity).
- Life-Threatening Infection: Fulminant osteomyelitis, necrotizing fasciitis, or uncontrolled sepsis involving the limb.
- Aggressive Malignancy: Primary bone or soft tissue tumors unresponsive to other treatments or with high metastatic potential.
- Intractable Pain: Severe, chronic pain unresponsive to all conservative and less invasive surgical treatments.
- Non-functional Limb: A limb that is a hindrance to function despite maximal reconstructive efforts and has no realistic potential for useful recovery (e.g., severe neurological injury with flail, insensate limb).
- Congenital Limb Deficiency: May necessitate amputation to facilitate prosthetic fitting and function.
Surgical Interventions for Gait Improvement in Neurologic Injury
- Spasticity Management: Tendon lengthenings (e.g., Achilles, hamstrings), tendon transfers (e.g., posterior tibialis to dorsum of foot for equinovarus), selective dorsal rhizotomy, neurolytic blocks, intrathecal baclofen pump insertion.
- Deformity Correction: Osteotomies (e.g., femoral or tibial derotational osteotomies, supracondylar femoral osteotomy for knee flexion contracture), arthrodesis for flail joints.
- Weakness/Paralysis: Tendon transfers (e.g., posterior tibialis to anterior for foot drop), nerve transfers.
- Contracture Release: Soft tissue releases to improve range of motion and facilitate orthotic use or ambulation.
Orthoses and Prostheses Prescription (Non-Operative/Post-Operative)
While typically non-operative interventions, the prescription of these devices is often based on surgical outcomes or anticipated functional deficits.
* Orthoses: To support weak muscles, correct deformities, reduce pain, improve stability (e.g., AFO for foot drop, KAFO for knee instability, spinal orthoses for trunk control).
* Prostheses: To replace a missing limb and restore functional mobility and cosmesis.
Contraindications
Absolute Contraindications to Amputation
- No absolute contraindications if limb salvage is not possible and life is threatened. However, factors influencing the level of amputation or timing can be seen as relative contraindications to a higher level.
- Inadequate Proximal Vascularity: For wound healing at the chosen level. Angiography and transcutaneous oxygen pressure measurements are crucial.
- Uncontrolled Sepsis/Infection: Without source control, a proximal amputation may not resolve the sepsis.
- Severe Comorbidities: Such as unstable cardiac disease or profound coagulopathy, may necessitate temporizing measures over immediate definitive surgery.
Relative Contraindications to Amputation (requiring careful consideration)
- Poor Rehabilitation Potential: Severe cognitive impairment, profound debility, or lack of social support. However, even these patients may benefit from a non-ambulatory amputation to improve hygiene, pain, or ease of care.
- Active Infection Proximal to Proposed Level: Risks wound healing failure.
- Patient Refusal: Unless life-threatening and patient lacks capacity.
Contraindications to Gait-Improving Surgery in Neurologic Injury
- Uncontrolled Spasticity: Without prior medical management or neurolysis, surgical release may be ineffective or lead to recurrence.
- Fixed Deformity: If bone or joint changes are too advanced for soft tissue release alone, an osteotomy may be indicated, but complete correction may be impossible.
- Progressive Neurological Disease: Benefits may be transient.
- Poor Compliance: With post-operative rehabilitation.
- Inadequate Strength: To utilize corrected limb position effectively.
Table of Indications: Operative vs. Non-Operative
The distinction between operative and non-operative indications in rehabilitation-focused orthopedics is often blurred, as surgery often facilitates subsequent non-operative management (e.g., prosthetic fitting).
| Category | Operative Indications | Non-Operative Indications |
|---|---|---|
| Amputation | Irreversible limb ischemia, uncontrollable infection, aggressive malignancy, severe trauma, intractable pain, severe non-functional limb, some congenital deficiencies. | Non-applicable (amputation is inherently operative) |
| Gait Improvement | Tendon contracture release, tendon transfers (for spasticity/weakness), osteotomies (for bony deformity), nerve releases, rhizotomy, intrathecal pump. | Physical therapy (strengthening, stretching, balance), orthotic prescription, oral antispasticity medications, focal botulinum toxin injections. |
| Prosthetics | Creation of an optimal residual limb for prosthetic fitting (e.g., appropriate length, stable muscle envelope, nerve management). | Prosthetic fitting, gait training, socket adjustments, component modifications. |
| Orthotics | Surgical correction of deformity (e.g., osteotomy) to allow for better orthotic fit or function. | Prescription of AFOs, KAFOs, braces for stability, support, or deformity prevention/correction. |
| Neurologic Injury | Tendon lengthening, muscle releases for spasticity, bony realignment, nerve procedures, joint fusion. | PT/OT, splinting, casting, medical management of spasticity, adaptive equipment, bracing. |
Pre Operative Planning and Patient Positioning
Thorough pre-operative planning is crucial for optimizing outcomes in both amputation surgery and corrective procedures for gait disorders. This process involves comprehensive patient evaluation, precise surgical site marking, and careful positioning.
Pre-operative Evaluation
General Assessment
- Medical Optimization: Evaluate and optimize cardiovascular, pulmonary, renal, and nutritional status. Diabetes control is paramount for wound healing. Smoking cessation is strongly encouraged.
- Vascular Assessment (for Amputation): Angiography, Doppler studies, transcutaneous oxygen pressure (TcPO2) measurements, and ankle-brachial index (ABI) are critical to determine the most distal level with adequate perfusion for healing. TcPO2 > 40 mmHg typically predicts good healing, while < 20 mmHg suggests poor healing.
- Infection Control: Obtain cultures from infected wounds; administer appropriate perioperative antibiotics. Debridement may precede definitive amputation.
- Nutritional Status: Malnutrition (albumin < 3.0 g/dL) increases complication rates. Nutritional support may be required pre-operatively.
- Psychological Evaluation: Assess patient's coping mechanisms, expectations, and potential for rehabilitation. Address phantom limb pain education.
- Rehabilitation Potential: Multidisciplinary team assessment (physiatrist, physical therapist, occupational therapist, prosthetist/orthotist, social worker) to gauge potential for ambulation and functional independence.
Specific Pre-operative Planning for Amputation
- Level Determination: The most distal level that will heal, considering patient's comorbidities and rehabilitation potential. Preserve maximal length while ensuring a healthy residual limb.
- Skin Flap Design: Typically anterior-posterior or sagittal flaps, designed to place the scar away from primary weight-bearing areas. The length of the flaps should be sufficient to close without tension.
- Muscle Management: Plan for myodesis (muscle-to-bone attachment) or myoplasty (muscle-to-muscle attachment) to stabilize the residual limb, provide padding, and allow for muscle control of the prosthesis.
- Nerve Management: Identify major nerves, gently retract, sharply transect with a scalpel, and allow them to retract proximally into soft tissue to minimize neuroma formation. Avoid cautery on nerve ends.
- Bone Management: Plan for smooth, beveled bone ends to prevent sharp edges from irritating soft tissue or prosthetic socket.
Specific Pre-operative Planning for Gait-Improving Surgery
- Detailed Gait Analysis: 3D motion analysis, video gait analysis, and electromyography (EMG) are invaluable for identifying specific gait deviations, muscle activity patterns, and kinematic/kinetic abnormalities.
- Physical Examination: Assess range of motion, muscle strength, spasticity (Modified Ashworth Scale), presence of contractures, and bony deformities.
- Imaging: X-rays, CT, or MRI as needed to assess bony deformities, joint health, and neurological structures.
- Multidisciplinary Team Meeting: Discuss surgical goals, expected outcomes, and post-operative rehabilitation plan with physiatrists, therapists, and orthotists.
Patient Positioning
Patient positioning depends on the planned procedure and the level of amputation or surgical correction. General principles apply:
* Sterile Field: Ensure adequate exposure of the surgical site and ability to extend the field if necessary.
* Pressure Point Padding: Protect bony prominences to prevent nerve compression or skin breakdown.
* Hemostasis: A tourniquet is typically used for lower limb amputations (unless contraindicated by vascular disease) to ensure a bloodless field and facilitate precise dissection. It should be applied high on the thigh.
* Anatomical Alignment: Position the limb to allow for natural alignment and ease of access to all aspects of the surgical field.
Positioning for Common Procedures
- Transtibial Amputation: Supine position, with the affected leg slightly abducted and externally rotated, often with a bump under the ipsilateral buttock. The leg is prepped from toes to mid-thigh.
- Transfemoral Amputation: Supine position, often with the affected leg slightly abducted. A bump under the ipsilateral buttock can facilitate hip adduction.
- Foot Amputations: Supine, with the foot elevated and possibly draped free to allow full range of motion during assessment.
- Tendon Transfers/Osteotomies: Supine, prone, or lateral decubitus depending on the specific muscle or bone being addressed. Careful attention to nerve protection during these procedures.
Detailed Surgical Approach and Technique
This section will primarily detail the surgical technique for lower limb amputations, as this is a foundational orthopedic procedure leading to extensive rehabilitation needs involving prosthetics and gait training. We will also briefly touch upon other surgical interventions aimed at improving gait secondary to neurological injury.
Principles of Amputation Surgery
The overarching goals of amputation surgery are to create a well-vascularized, pain-free, functionally optimal residual limb (stump) that can tolerate prosthetic fitting, while addressing the underlying pathology and preserving life.
- Preservation of Length: Maximize residual limb length consistent with healthy tissues and good prosthetic function.
- Healthy Skin Flaps: Design flaps to provide adequate soft tissue coverage without tension, with the scar located away from primary weight-bearing areas.
- Vascular Supply: Ensure robust blood supply to the skin and muscle flaps.
- Nerve Management: Identify major nerves, gently pull distally, sharply transect at the most proximal possible level with a new scalpel blade, and allow them to retract into soft tissue to minimize neuroma formation. Avoid crushing or cauterizing nerve ends.
- Muscle Stabilization (Myodesis/Myoplasty): Secure muscle groups to bone (myodesis) or to each other (myoplasty) to create a stable, conical, padded residual limb. This provides proprioception, improves prosthetic control, and minimizes muscle atrophy.
- Bone Management: Smooth, rounded, beveled bone ends prevent distal irritation and pressure points.
- Hemostasis: Meticulous hemostasis to prevent hematoma formation, which can compromise wound healing and increase infection risk.
- Wound Closure: Tension-free, multi-layered closure. Drains may be used selectively.
Surgical Technique: Transtibial Amputation (Below-Knee Amputation)
The transtibial amputation is the most common and often functionally superior lower extremity amputation due to preservation of the knee joint.
1. Incision Design and Dissection
- Marking: Identify tibial tuberosity, outline desired bone cut (typically 12.5-17.5 cm distal to medial tibial plateau, allowing 10-12 cm residual tibia).
- Skin Flaps:
- Long Posterior Flap: Most common. An anterior transverse incision is made at the level of the tibial bone cut. Two vertical limbs extend distally for 10-12 cm, joining with a transverse posterior incision. This provides a generous, well-vascularized posterior flap containing gastrocnemius-soleus musculature.
- Sagittal Flaps: Equal anterior and posterior flaps. Useful in trauma or when local tissue viability dictates.
- Initial Dissection: Incise skin and subcutaneous tissue. Identify and ligate the anterior tibial artery and vein in the anterior compartment.
- Anterior Compartment: Transect tibialis anterior, extensor digitorum longus, extensor hallucis longus. Identify and sharply transect the deep peroneal nerve high.
- Lateral Compartment: Transect peroneus longus and brevis. Identify and sharply transect the superficial peroneal nerve high.
2. Bone Section
- Periosteum: Incise periosteum at the level of the planned tibial and fibular bone cuts.
- Fibular Osteotomy: The fibula is cut first, typically 1-2 cm shorter than the tibia, to prevent distal pressure. Use an oscillating saw. Smooth the edges.
- Tibial Osteotomy: Cut the tibia using an oscillating saw. The anterior tibial crest is carefully beveled at a 45-60 degree angle to remove the sharp anterior edge, preventing skin breakdown in the prosthesis. Smooth all bone edges.
- Interosseous Membrane: Transect the interosseous membrane.
3. Posterior Compartment and Muscle Management
- Identification: Retract the tibia and fibula anteriorly. Identify the posterior tibial artery/vein and peroneal artery/vein bundles. Ligate these securely.
- Tibial Nerve: Identify the tibial nerve, gently pull distally, sharply transect high, and allow it to retract.
- Sural Nerve: Identify the sural nerve (posterior-lateral aspect), transect and allow to retract.
- Myodesis/Myoplasty:
- Gastrocnemius-Soleus Flap: The muscle belly is beveled to avoid bulk. It is then securely sutured to the anterior periosteum and fascia of the tibia. This provides distal padding, stabilizes the tibia, and allows for better proprioception. This can be achieved via drill holes in the tibia for direct myodesis or by suturing the posterior deep fascia to the anterior deep fascia (myoplasty). The Ertl procedure involves creating a tibiofibular bone bridge and securing the muscle to it, but is less commonly performed.
- Anterior Muscles: The cut ends of the anterior compartment muscles can be sutured to the gastrocnemius muscle mass.
4. Wound Closure
- Hemostasis: Thoroughly irrigate the wound and achieve meticulous hemostasis.
- Drains: A suction drain may be placed superficially, particularly if there's concern for hematoma.
- Fascial Closure: Close deep fascia over the muscle mass.
- Skin Closure: Close skin with interrupted sutures, avoiding tension. A soft dressing is applied, avoiding circumferential wraps that could cause tourniquet effect.
- Rigid Removable Dressing (RRD) or IPOP: A plaster or fiberglass cast may be applied as an Immediate Post-Operative Prosthesis (IPOP) or a Rigid Removable Dressing (RRD) to control edema, protect the wound, and aid in pain control.
FIG. 10.3: Surgical field during transtibial amputation, illustrating bone cuts and muscle flap management.
Surgical Technique: Transfemoral Amputation (Above-Knee Amputation)
1. Incision Design and Dissection
- Marking: Identify desired femoral bone cut (typically 25-30 cm distal to greater trochanter). Similar to transtibial, the goal is to create a conical shape.
- Skin Flaps: Usually equal anterior and posterior flaps or a long anterior flap for maximum soft tissue coverage over the distal femur.
- Muscle Dissection: Incise through skin, subcutaneous tissue. Transect quadriceps muscles anteriorly, hamstrings posteriorly, and adductor muscles medially. Identify and ligate perforating vessels.
2. Neurovascular Management
- Femoral Artery/Vein: Ligate these robustly.
- Sciatic Nerve: Identify the large sciatic nerve. Gently pull distally, sharply transect at the highest possible level, and allow it to retract into the gluteal musculature.
- Femoral Nerve: Identify and transect the femoral nerve.
- Obturator Nerve: Identify and transect the obturator nerve.
3. Bone Section
- Femoral Osteotomy: Periosteum is incised circumferentially. The femur is cut with an oscillating saw. The distal end is typically beveled or rounded to avoid sharp edges.
4. Muscle Stabilization
- Adductor Myodesis: The adductor magnus is critical. It is detached from its femoral insertion, brought laterally, and sutured to the distal lateral femur. This provides medial padding and helps prevent abduction contracture of the hip.
- Quadriceps/Hamstring Myoplasty: The remaining quadriceps and hamstring muscles are often sutured together over the distal femur or to remaining periosteum to create a stable, functional muscle mass.
5. Wound Closure
- Meticulous hemostasis, drain placement, multi-layered tension-free closure.
Other Surgical Interventions for Gait Improvement
These procedures are often performed in patients with neurological conditions (e.g., Cerebral Palsy, Stroke, Spinal Cord Injury) to address spasticity, contractures, or muscle imbalance affecting gait.
- Tendon Lengthening: For fixed contractures (e.g., Achilles tendon lengthening for equinus deformity, hamstring lengthening for knee flexion contracture). Z-plasty or fractional lengthening techniques are common.
- Tendon Transfer: To rebalance muscle forces. E.g., Posterior Tibialis Tendon Transfer (PTTT) to the dorsum of the foot for foot drop or severe equinovarus. This aims to convert a strong plantarflexor/invertor into a dorsiflexor/evertor.
- Osteotomies: For fixed bony deformities that cannot be corrected by soft tissue procedures (e.g., femoral derotational osteotomy for excessive femoral anteversion, supracondylar femoral osteotomy for knee flexion deformity).
- Selective Dorsal Rhizotomy (SDR): A neurosurgical procedure involving selective cutting of sensory nerve rootlets in the spinal cord to reduce spasticity, primarily in cerebral palsy. While a neurosurgical procedure, orthopedic surgeons often work in conjunction to manage resultant skeletal changes.
- Nerve Releases: For specific nerve entrapments causing weakness or pain that contributes to gait dysfunction.
The success of these interventions relies heavily on meticulous surgical technique, precise anatomical understanding, and a robust post-operative rehabilitation program.
Complications and Management
Complications following orthopedic procedures that impact gait can significantly impede rehabilitation and functional recovery. These can range from immediate surgical issues to long-term prosthetic or orthotic challenges.
Amputation-Specific Complications
1. Wound Healing Complications
- Incidence: High, especially in patients with vascular disease (15-30%).
- Manifestations: Wound dehiscence, necrosis of skin flaps, infection.
- Management:
- Minor Dehiscence/Superficial Necrosis: Local wound care, serial debridement, negative pressure wound therapy (NPWT).
- Major Dehiscence/Deep Infection: Requires surgical debridement, IV antibiotics, potential revision amputation, or muscle flap coverage.
- Non-healing: Often indicates inadequate vascular supply; revascularization attempts or revision to a higher amputation level may be necessary.
2. Infection
- Incidence: Varies, but can be up to 20% in high-risk patients.
- Manifestations: Cellulitis, abscess, osteomyelitis of the residual bone.
- Management: Culture-directed antibiotics, incision and drainage, debridement. Osteomyelitis may require bone resection or revision.
3. Phantom Limb Pain (PLP)
- Incidence: Up to 80% of amputees experience PLP.
- Manifestations: Perceived pain in the missing limb, described as burning, cramping, shooting, or crushing.
- Management: Multimodal approach including pharmacotherapy (gabapentin, pregabalin, tricyclic antidepressants, opioids), regional nerve blocks, TENS, mirror therapy, psychological counseling. Surgical neurectomy is rarely effective and can exacerbate symptoms.
4. Residual Limb Pain
- Incidence: Common, distinct from PLP.
- Manifestations: Pain in the remaining limb, often localized to neuromas, heterotopic ossification, bone spurs, or poor prosthetic fit.
- Management:
- Neuroma: Local steroid injection, targeted resection, or chemical neurolysis. Relocation of the neuroma away from pressure points (targeted muscle reinnervation TMR) can be considered.
- Heterotopic Ossification: Surgical excision if it causes pain or impedes prosthetic fit. Prophylaxis with NSAIDs or radiation therapy can be considered.
- Bone Spurs: Surgical removal.
- Prosthetic Issues: Adjustments to socket, liner, or suspension.
5. Contractures
- Incidence: Common, especially hip flexion contractures in transfemoral amputees and knee flexion contractures in transtibial amputees.
- Management: Aggressive physical therapy, stretching, prone lying, splinting, appropriate positioning. Surgical release or manipulation under anesthesia may be required for severe, fixed contractures.
6. DVT and PE
- Incidence: Significant risk in surgical patients.
- Management: Prophylaxis with pharmacologic agents (LMWH) and mechanical methods (compression stockings, IPC devices). Surveillance for symptoms.
Prosthetic and Orthotic-Specific Complications
1. Skin Breakdown and Ulceration
- Incidence: Very common.
- Causes: Poor prosthetic/orthotic fit, excessive pressure, friction, inadequate hygiene, decreased sensation.
- Management: Immediate removal of device, wound care, device adjustments by prosthetist/orthotist, pressure relief, re-evaluation of residual limb shape, patient education.
2. Poor Fit and Discomfort
- Causes: Volume changes in residual limb, inadequate socket design, improper alignment, weight changes.
- Management: Socket modification (padding, build-ups, reliefs), liner changes, suspension system adjustments, prosthetic alignment modification.
3. Mechanical Failure of Device
- Causes: Component breakage (pylon, foot, knee unit), wear and tear, improper use.
- Management: Repair or replacement of components by prosthetist/orthotist.
Complications of Gait-Improving Surgery in Neurologic Injury
1. Recurrence of Deformity/Spasticity
- Causes: Incomplete release, progression of neurological disease, inadequate post-operative therapy.
- Management: Revision surgery, further chemodenervation (Botox), re-evaluation of medical management (e.g., baclofen pump settings), intensive rehabilitation.
2. Overcorrection/New Deformity
- Causes: Excessive lengthening or transfer.
- Management: Orthotic management, further surgery (e.g., tendon transfer reversal, osteotomy).
3. Nerve Injury
- Causes: Iatrogenic injury during dissection or excessive traction.
- Management: Conservative management for neuropraxia, exploration and repair/grafting for neurotmesis.
Table of Common Complications and Management Strategies
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Wound Dehiscence/Necrosis | 15-30% | Surgical debridement, local wound care, NPWT, IV antibiotics, muscle flaps, revision amputation (for severe cases). |
| Infection (Amputation) | 5-20% | Culture-directed antibiotics, incision & drainage, surgical debridement, bone resection, revision amputation. |
| Phantom Limb Pain | 50-80% | Multimodal analgesia (gabapentinoids, TCAs, opioids), regional blocks, TENS, mirror therapy, psychological support. |
| Neuroma | 5-30% | Steroid injections, surgical excision/relocation (TMR), chemical neurolysis. |
| Contracture (Hip/Knee) | 20-40% | Aggressive PT, stretching, prone lying, splinting, serial casting, surgical release/manipulation under anesthesia. |
| Heterotopic Ossification | 10-30% | Surgical excision if symptomatic or interferes with prosthetic fit. Prophylactic NSAIDs/radiation. |
| Skin Breakdown (Prosthesis/Orthosis) | Very common | Device removal, wound care, immediate prosthetic/orthotic adjustment, patient education, pressure relief, review of liner/interface. |
| Poor Prosthetic/Orthotic Fit | Very common | Socket adjustments, liner changes, suspension modifications, prosthetic alignment changes, residual limb volume management (shrinkers). |
| Mechanical Failure of Device | Variable | Repair or replacement of components by prosthetist/orthotist. |
| Recurrence of Deformity (Neurologic Surgery) | 10-30% | Revision surgery, further chemodenervation (Botox), optimization of medical therapy, intensified rehabilitation, orthotic management. |
| Nerve Injury (Iatrogenic) | <5% | Conservative management (neuropraxia), exploration and direct repair/graft for neurotmesis. |
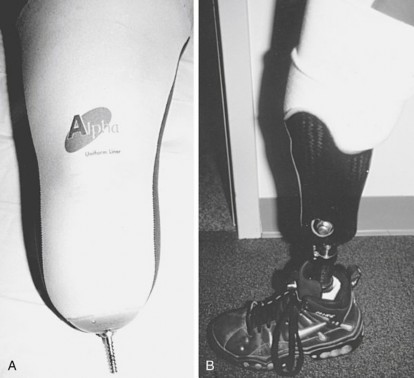
FIG. 10.4: Common skin complications in amputees include pressure ulcers, often requiring prosthetic adjustments and diligent wound care.
Post Operative Rehabilitation Protocols
Post-operative rehabilitation is a cornerstone of recovery following amputation or surgical intervention for gait impairment. A multidisciplinary team approach involving physical therapists, occupational therapists, prosthetists, orthotists, and physiatrists is essential for maximizing functional outcomes.
Phase 1: Acute Post-Surgical Management (Days 1-14)
Goals
- Wound healing and infection prevention.
- Pain and edema control.
- Preservation of joint range of motion (ROM).
- Prevention of contractures.
- Early mobilization and strengthening of intact musculature.
- Patient and family education.
Key Interventions
- Wound Care: Meticulous dressing changes, monitoring for signs of infection or dehiscence.
- Edema Control: Compression therapy is paramount using elastic bandages, shrinkers, or rigid removable dressings (RRD) as soon as wound healing permits. This shapes the residual limb for prosthetic fitting.
- Pain Management: Multimodal analgesia, including regional blocks, oral medications, and non-pharmacologic strategies for phantom limb pain (e.g., mirror therapy).
- Positioning: Avoid positions that promote contractures (e.g., prolonged hip flexion in transfemoral, knee flexion in transtibial). Prone lying for transfemoral amputees helps prevent hip flexion contractures.
- Early ROM and Strengthening: Gentle active and passive ROM exercises for adjacent joints (e.g., hip in transtibial, hip/knee in contralateral limb). Isometrics for residual limb muscles once pain subsides.
- Mobility: Bed mobility, transfers to chair, and early wheelchair training. Initiate upper body strengthening for transfer independence.
Phase 2: Pre-Prosthetic Training (Weeks 2-12)
Goals
- Residual limb maturation and shaping.
- Maximizing strength and endurance.
- Achieving full ROM in all relevant joints.
- Improving balance and proprioception.
- Education on prosthetic components and care.
Key Interventions
- Residual Limb Shaping: Consistent use of shrinkers or RRD to achieve a conical, stable residual limb.
- Strength Training: Progressive resistive exercises for all major muscle groups, particularly hip extensors/abductors for transfemoral and knee extensors/flexors for transtibial. Core strengthening.
- ROM Maintenance: Continue stretching and positioning to prevent contractures.
- Balance Training: Seated and standing balance exercises (single limb stance on intact limb).
- Functional Mobility: Continued transfer training, wheelchair mobility, and progression to crutch or walker training (if appropriate) for short distances on the intact limb.
- Patient Education: Discuss prosthetic options, hygiene, skin care, and realistic expectations.
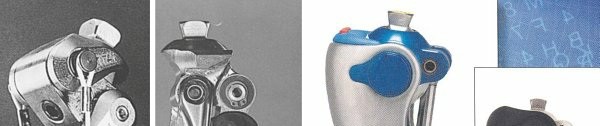
FIG. 10.5: Post-operative residual limb shaping with an elastic shrinker is critical for preparing for prosthetic fitting.
Phase 3: Prosthetic Prescription and Training (Weeks 12+)
Goals
- Optimal prosthetic fitting.
- Achieving independent and efficient prosthetic gait.
- Mastering advanced mobility skills and ADLs.
- Long-term limb health and prosthetic maintenance.
Key Interventions
- Prosthetic Prescription:
- Evaluation: The physiatrist and prosthetist collaborate to determine the most appropriate components based on patient's activity level, functional goals, residual limb characteristics, and financial considerations.
- Socket Design: Critical for comfort, stability, and control. Types include total surface bearing, patellar tendon bearing (PTB) for transtibial, and ischial containment (IC) or quadrilateral sockets for transfemoral.
- Suspension Systems: Suction, sleeve, pin/lock, vacuum, or anatomical suspension.
- Components: Different prosthetic feet (SACH, energy-storing, microprocessor), knee units (single axis, polycentric, hydraulic, microprocessor), and pylons are selected.

FIG. 10.6: Example of a transtibial prosthesis with various components: socket, pylon, and prosthetic foot.
- Prosthetic Training:
- Donning and Doffing: Patients must master independent application and removal.
- Weight Bearing and Balance: Initial standing balance with parallel bars, progressing to dynamic weight shifts.
- Gait Training: Focus on proper prosthetic alignment, smooth weight transfer, equal step length, and minimization of compensatory gait deviations (e.g., vaulting, circumduction). Progression from parallel bars to walker, crutches, and eventually cane or independent ambulation.
- Stairs, Ramps, Uneven Terrain: Training for diverse environments.
- Falls Prevention: Strategies and recovery techniques.
- ADL Training: Integration of prosthesis into daily activities.
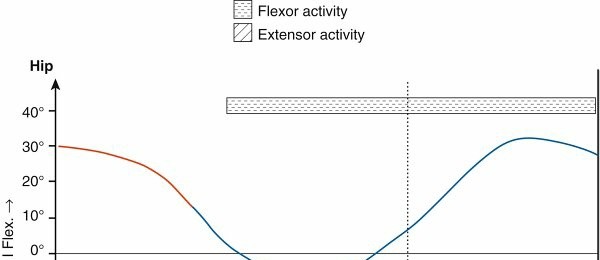
FIG. 10.7: Gait training with a prosthesis in a rehabilitation setting.
- Long-Term Management: Regular follow-up with the prosthetist for adjustments, skin checks, and component maintenance. Education on skin hygiene and signs of complications.
Rehabilitation for Neurologic Injury (Orthoses Focus)
For patients with neurological injury (e.g., stroke, spinal cord injury, cerebral palsy), rehabilitation focuses on optimizing residual function and often involves significant orthotic intervention.
Goals
- Maximize motor control and strength.
- Manage spasticity and prevent contractures.
- Improve balance and coordination.
- Optimize energy efficiency of gait.
- Restore functional mobility with appropriate orthoses.
Key Interventions
- Spasticity Management: Oral medications, intrathecal baclofen, botulinum toxin injections, serial casting, stretching.
- Strength and Motor Control Training: Neuromuscular re-education, task-specific training, functional electrical stimulation (FES).
- Balance and Coordination: Proprioceptive training, balance boards, functional activities.
- Orthotic Prescription:
- Ankle-Foot Orthoses (AFOs): Most common. Used for foot drop, ankle instability, or to control equinus/varus/valgus deformities. Can be solid, hinged, or posterior leaf spring (PLS) design.
- Knee-Ankle-Foot Orthoses (KAFOs): For knee instability (e.g., quadriceps weakness, genu recurvatum) in addition to ankle control.
- Hip-Knee-Ankle-Foot Orthoses (HKAFOs): For extensive lower limb weakness or paralysis, often in spinal cord injury. Provides trunk and hip stability.
- Spinal Orthoses: For trunk instability or scoliosis associated with neurological conditions.

FIG. 10.8: A typical ankle-foot orthosis (AFO) used to manage foot drop and ankle instability in neurologic conditions.
- Gait Training with Orthoses: Learning to ambulate with the orthosis, optimizing stride length, velocity, and energy efficiency. Compensatory strategies may be taught to improve functional mobility.
- Assistive Devices: Walkers, crutches, canes.
The continuum of rehabilitation, from acute care to lifelong prosthetic or orthotic management, demands a collaborative and individualized approach to achieve the highest possible functional independence for each patient.
Summary of Key Literature and Guidelines
The comprehensive management of patients requiring rehabilitation for gait, amputations, prostheses, orthoses, and neurologic injury is guided by a robust body of literature and established clinical guidelines. These frameworks emphasize evidence-based practice, multidisciplinary collaboration, and patient-centered care.
Amputation Surgery and Post-Operative Management
- Surgical Techniques: The literature consistently supports meticulous surgical technique in amputation to achieve optimal residual limb shape, prevent neuromas, and ensure adequate vascularity for wound healing. Myodesis and myoplasty are favored for their ability to stabilize muscles, improve proprioception, and enhance prosthetic control. Contemporary texts like "Orthopaedic Knowledge Update: Trauma" and "Campbell's Operative Orthopaedics" provide detailed surgical approaches.
- Wound Care and Edema Control: Early application of rigid removable dressings (RRD) or immediate post-operative prostheses (IPOP) is advocated by several studies for edema control, pain reduction, and faster residual limb maturation compared to soft dressings alone. Consensus guidelines from the American Academy of Orthotists and Prosthetists (AAOP) support this.
- Phantom Limb Pain: Multimodal pain management strategies are standard. Reviews published in journals like Pain and Anesthesiology highlight the efficacy of gabapentinoids, tricyclic antidepressants, and non-pharmacological interventions like mirror therapy. The Veterans Health Administration (VA) has specific guidelines for chronic pain management in amputees.
Prosthetic and Orthotic Management
- Prosthetic Prescription: Guidelines from organizations such as the International Society for Prosthetics and Orthotics (ISPO) and AAOP provide frameworks for appropriate prosthetic component selection based on patient activity levels, functional goals, and residual limb characteristics. Literature in journals like Prosthetics and Orthotics International frequently discusses advancements in microprocessor knees, energy-storing feet, and osseointegration.
- Gait Training: Evidence-based rehabilitation protocols emphasize progressive gait training, starting with weight bearing and balance, progressing to functional mobility on varied terrains. Studies in Archives of Physical Medicine and Rehabilitation and Physical Therapy demonstrate the importance of task-specific training and strength conditioning to reduce energy expenditure and improve gait efficiency in amputees.
- Orthotic Use in Neurologic Injury: The efficacy of various orthoses (e.g., AFOs for foot drop) in improving gait kinematics, kinetics, and energy efficiency is well-documented. Clinical practice guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the American Physical Therapy Association (APTA) often address orthotic intervention for specific neurological conditions (e.g., post-stroke gait deficits, cerebral palsy). Research in Developmental Medicine & Child Neurology frequently explores orthotic interventions in pediatric populations.
Rehabilitation for Neurologic Injury
- Spasticity Management: Comprehensive guidelines from the American Academy of Neurology (AAN) address the use of oral antispasticity medications, chemodenervation (botulinum toxin), intrathecal baclofen, and surgical interventions like selective dorsal rhizotomy. Orthopedic involvement focuses on managing secondary musculoskeletal sequelae such as contractures and deformities.
- Surgical Interventions: The literature supports tendon lengthenings, transfers, and osteotomies for addressing fixed deformities and muscle imbalances caused by spasticity or weakness. Outcomes are often reported in Journal of Bone and Joint Surgery and Clinical Orthopaedics and Related Research, emphasizing the importance of precise patient selection and aggressive post-operative rehabilitation.
- Multidisciplinary Approach: Consensus statements across various medical specialties (orthopedics, physiatry, neurology, physical therapy) underscore the necessity of a multidisciplinary team for optimal outcomes in complex neurologic gait disorders.
Key Literature and Ongoing Research
- Gait Analysis: Advanced 3D gait analysis remains the gold standard for objective assessment of gait deviations, informing surgical planning and rehabilitation strategies. Research continues to refine normative data and pathological patterns.
- Osseointegration: This emerging field in prosthetics, involving direct bone attachment of prosthetic components, is a subject of intense research, with ongoing clinical trials exploring its long-term benefits in terms of stability, proprioception, and quality of life for amputees.
- Neuromodulation: Techniques like transcranial magnetic stimulation (TMS) and deep brain stimulation (DBS) are being explored for spasticity and gait disorders, particularly in conditions like Parkinson's disease.
- Advanced Prosthetic Technology: Development of powered prostheses, brain-computer interfaces, and targeted muscle reinnervation (TMR) for improved prosthetic control and sensory feedback represents the cutting edge of research.
In summary, the field of rehabilitation for gait disorders, amputations, prostheses, orthoses, and neurologic injury is dynamic, continually evolving with technological advancements and deepening biomechanical understanding. Adherence to established guidelines and engagement with ongoing research ensures that orthopedic surgeons and their rehabilitation teams provide the most effective, evidence-based care to restore function and improve the quality of life for these patients.
Clinical & Radiographic Imaging




You Might Also Like

