Sacral Fractures and Lumbosacral Dislocation: Comprehensive Surgical Management
Key Takeaway
Sacral fractures and lumbosacral dislocations represent complex, high-energy injuries often associated with pelvic ring disruptions. Due to a high initial miss rate, a rigorous clinical index of suspicion is required. Management hinges on accurate classification, such as the Denis and Aihara systems, to dictate operative versus nonoperative care. Surgical intervention is primarily indicated for progressive neurological deficits, unstable fracture-dislocations, and severe sacropelvic deformity, utilizing advanced techniques like triangular osteosynthesis and lumbosacral pedicle screw fixation.
INTRODUCTION AND EPIDEMIOLOGY
Sacral fractures and lumbosacral dislocations are severe, high-energy injuries that constitute approximately 1% of all spinal fractures. Because of the complex regional anatomy and the frequently distracting nature of concomitant polytrauma, these injuries are notoriously difficult to diagnose upon initial presentation. Historically, Lafollete, Levine, and McNiesh noted that up to 60% of sacral fractures are missed during the primary trauma survey.
More than 90% of indirect sacral fractures are associated with pelvic ring disruptions. The most common mechanisms of injury include high-velocity motor vehicle collisions, motorcycle accidents, and falls from significant heights. Given the intimate relationship between the sacrum and the lumbosacral plexus, 25% to 50% of these fractures present with an accompanying neurological deficit.
Clinical Pearl: A high index of suspicion is mandatory in any polytrauma patient presenting with a pelvic fracture. A meticulous neurological examination must be performed, specifically assessing for sacral root dysfunction. Key indicators include decreased perianal sensation, rectal sphincter disturbance, diminished or absent ankle jerk reflexes, and the absence of the bulbocavernosus reflex.
CLASSIFICATION SYSTEMS
Accurate classification of sacral fractures and lumbosacral dislocations is paramount for determining structural stability, predicting neurological compromise, and guiding surgical intervention.
The Schmidek Classification (Mechanism of Injury)
Schmidek et al. broadly categorized sacral fractures based on the mechanism of injury into direct and indirect trauma.
Direct Trauma:
* Penetrating Injuries: Gunshot wounds are the most common cause of direct sacral trauma. While structurally stable in most cases, they carry a high risk of localized nerve root injury and infection.
* Comminuted Fractures: Resulting from direct, severe, blunt trauma. These are frequently accompanied by significant sacral nerve root injuries.
* Low Transverse Fractures: Typically caused by a direct blow to the coccyx, resulting in the forward displacement of the sacrococcygeal fragment.
Indirect Trauma:
Most sacral fractures fall into this category and are intimately linked to pelvic ring disruptions. Types include:
* High transverse fractures
* Vertical fractures
* Lateral mass and juxtaarticular fractures
* Cleaving and avulsion fractures
The Denis Classification (Anatomic Zones)
Denis devised a universally adopted classification system that divides the sacrum into three distinct vertical zones based on the location of the fracture line. This system is highly predictive of neurological injury.
- Zone I (Region of the Ala): Fractures occur lateral to the sacral foramina. These are the most common but carry the lowest risk of neurological deficit (approximately 5.9%). When deficits occur, they typically involve the L5 nerve root due to compression by the displaced sacral ala.
- Zone II (Region of the Sacral Foramina): Fractures involve one or more sacral foramina but do not extend into the central canal. Bonnin identified the foramen as the weakest structural part of the sacrum. The incidence of neurological deficit in Zone II fractures is 28%, frequently presenting as unilateral radiculopathy (sciatica-like symptoms).
- Zone III (Region of the Central Sacral Canal): Fractures involve the central sacral canal. These are the most severe, with an 87% incidence of neurological deficits. Patients frequently present with cauda equina syndrome, characterized by profound bowel, bladder, and sexual dysfunction.
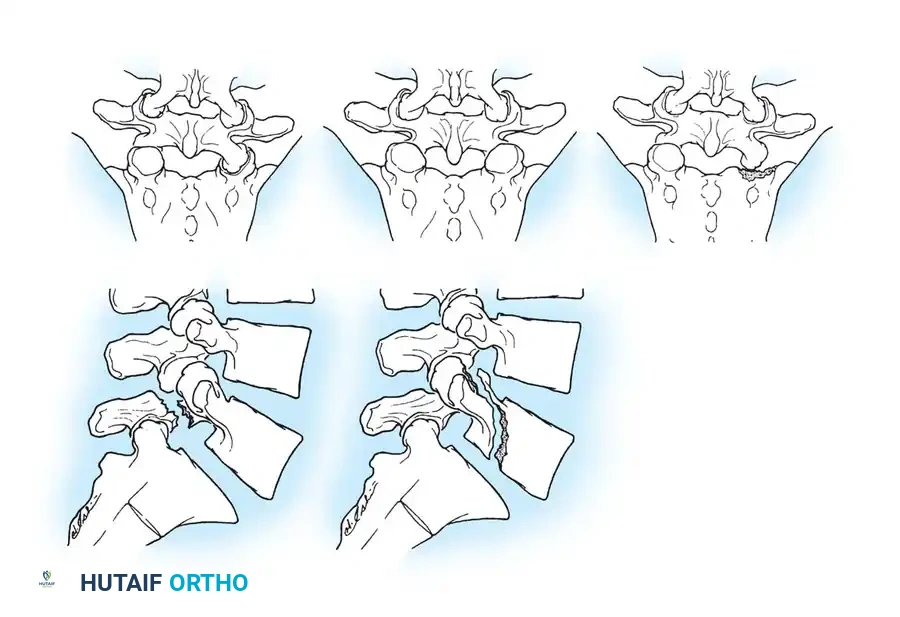
The Aihara Classification for Lumbosacral Dislocation
Aihara et al. proposed a comprehensive classification system for fracture-dislocations of the lumbosacral junction (L5-S1). After reviewing 50 reported cases, they concluded that conservative treatment is generally ineffective due to the inherent instability of the injury.
The Aihara classification includes:
* Type 1: Unilateral lumbosacral facet dislocation with or without facet fracture.
* Type 2: Bilateral lumbosacral facet dislocation with or without facet fracture.
* Type 3: Unilateral lumbosacral facet dislocation combined with a contralateral lumbosacral facet fracture.
* Type 4: Dislocation of the body of L5 with bilateral fractures of the pars interarticularis.
* Type 5: Dislocation of the body of L5 with a fracture of the vertebral body or pedicle, with or without injury to the lamina or facet.
INDICATIONS FOR MANAGEMENT
The management of sacral fractures and lumbosacral dislocations remains challenging, requiring a highly individualized approach based on fracture morphology, pelvic stability, and neurological status.
Nonoperative Management
Conservative treatment is reserved for structurally stable, non-displaced fractures without neurological deficits.
* Protocol: Strict bed rest for 8 to 12 weeks.
* Immobilization: The successful use of a hip spica cast has been reported in select cases to limit lumbosacral motion, though patient compliance and skin complications must be closely monitored.
Operative Indications
Surgical intervention is strictly indicated in the presence of:
1. Progressive neurological impairment.
2. Confirmed neural compression from retropulsed fracture fragments or disc herniation.
3. Severe sacral deformity (e.g., highly displaced U-shaped sacral kyphosis).
4. Intractable, chronic pain secondary to instability or nonunion.
5. Concomitant unstable pelvic ring disruptions requiring spinopelvic fixation.
Surgical Warning: Delayed neurological injury is a common complication in nonoperatively managed patients. This typically results from the progressive entrapment of sacral nerve roots by fracture deformity, settling, or exuberant callus formation.
SURGICAL APPROACHES AND TECHNIQUES
Operative management is technically demanding, heavily dependent on the patient's bone quality, and should be performed by experienced spinal or pelvic trauma surgeons.
Anterior Decompression and Strut Graft Fusion
For complex burst fractures or fracture-dislocations at the thoracolumbar or upper lumbar spine extending toward the lumbosacral junction, an anterior retroperitoneal approach may be utilized for direct decompression of the thecal sac.
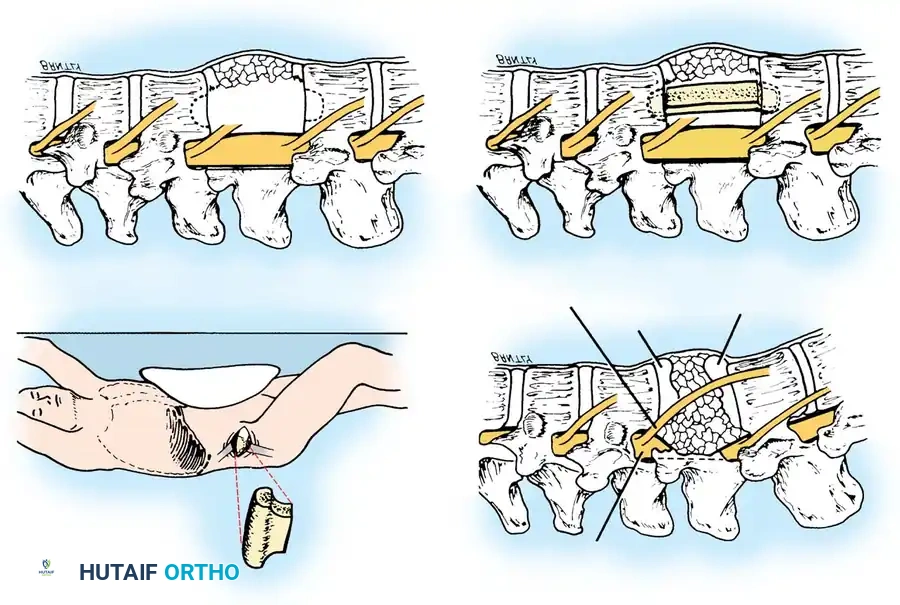
Surgical Steps:
1. Positioning: The patient is placed in the lateral decubitus position.
2. Exposure: A retroperitoneal approach is utilized. Orientation is facilitated by identifying the psoas muscle and tracing the course of the 12th intercostal nerve.
3. Corpectomy and Decompression: After the removal of the ipsilateral pedicle and the fractured vertebral body, retropulsed fragments compressing the thecal sac are visualized. These fragments are meticulously removed using a high-speed burr and curettes until the base of the opposite pedicle is exposed and the dura is fully decompressed.
4. Reconstruction: An iliac crest tricortical strut graft is harvested. The graft is locked into place using bone tamps, with each end carefully countersunk into the intact vertebral bodies above and below the resection site to ensure biomechanical stability.
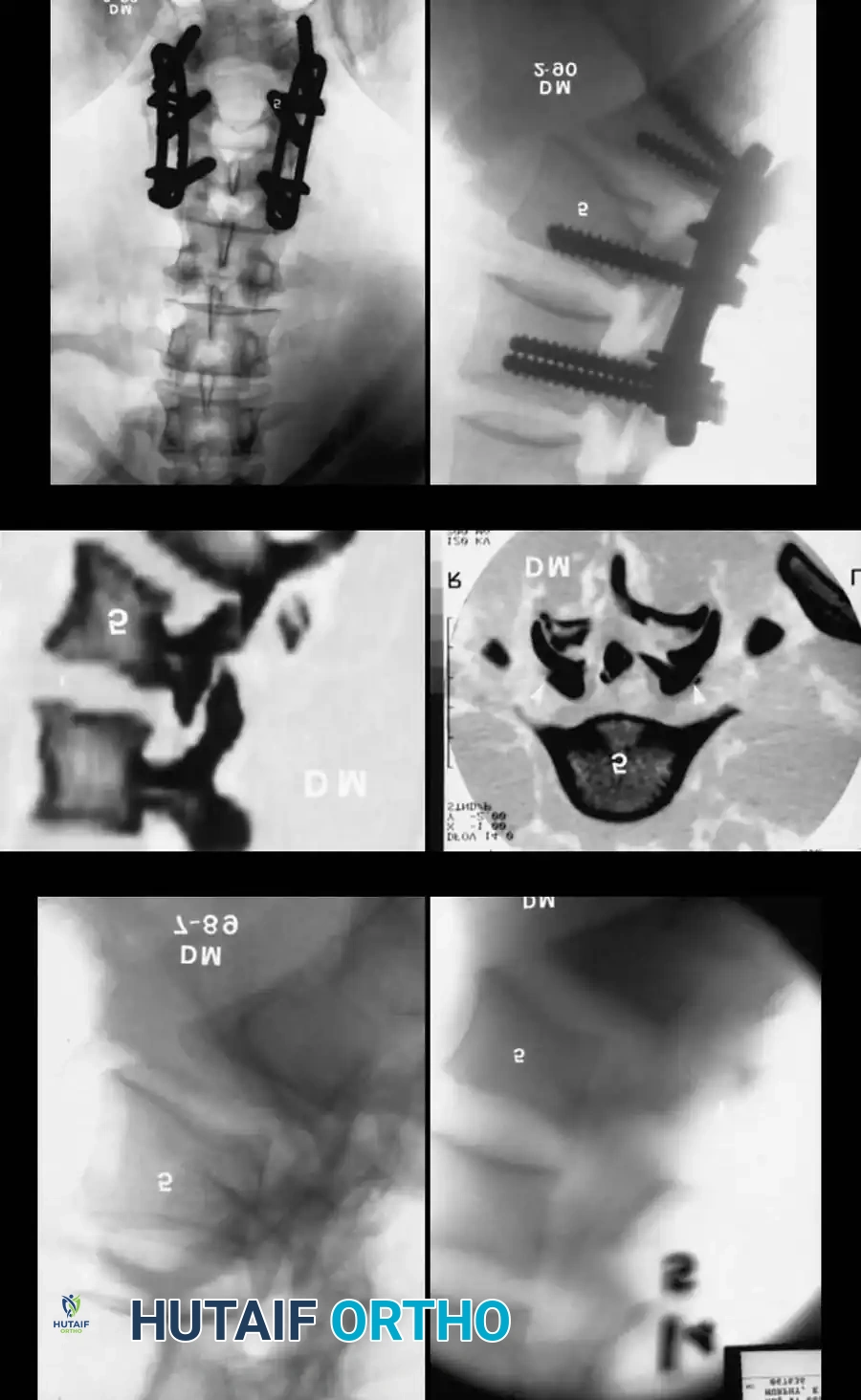
Posterior Lumbosacral Decompression and Pedicle Screw Fixation
Lumbosacral dislocations (Aihara Types 1-5) and highly unstable sacral fractures are most effectively stabilized using posterior instrumentation.
Surgical Steps:
1. Positioning: The patient is positioned prone on a radiolucent Jackson table, ensuring the abdomen is free to reduce venous pressure and epidural bleeding.
2. Exposure: A standard midline incision is made, followed by subperiosteal dissection to expose the posterior elements of L4, L5, and the sacrum.
3. Decompression (Sacral Laminectomy): A wide laminectomy is performed to allow exploration of the lower lumbar and sacral nerve roots. This step is critical for the evacuation of epidural hematomas, removal of compressive bone fragments from the spinal canal, and direct visualization of the neural elements during reduction maneuvers.
4. Instrumentation: Pedicle screws are placed into the lower lumbar vertebrae (L4, L5). For sacral fixation, S1 and S2 pedicle screws or iliac/sacropelvic screws are utilized depending on the degree of instability.
5. Reduction: Gentle reduction of the lumbosacral dislocation is performed. In cases of traumatic spondylolisthesis (e.g., L5 on S1), reduction must be done under direct visualization of the L5 and S1 nerve roots to prevent iatrogenic traction injuries.
Biomechanics Pearl: Schildhauer et al. demonstrated in cadaveric biomechanical studies that for highly unstable sacral fractures, triangular osteosynthesis (combining lumbopelvic fixation with transverse iliosacral screws) provides significantly greater multiplanar stability compared to simple iliosacral screws alone.
Percutaneous Iliosacral Screw Fixation
For specific fracture patterns, such as U-shaped sacral fractures associated with pelvic ring disruptions, minimally invasive techniques can be employed.
Nork et al. described the stabilization of U-shaped sacral fractures using percutaneous iliosacral screws inserted under strict fluoroscopic guidance.
* Technique: This technique is generally limited to patients with acceptable sacral kyphotic deformities, allowing for in situ fixation without formal open reduction.
* Limitations: Direct sacral neurological decompression is not performed. While all fractures in Nork's series healed with minimal change in kyphosis, patients with preoperative neurological abnormalities may experience residual deficits.
POSTOPERATIVE PROTOCOLS AND OUTCOMES
Rehabilitation and Mobilization
The postoperative protocol is dictated by the rigidity of the surgical construct.
* Patients treated with robust internal fixation (e.g., triangular osteosynthesis, transiliac screws, or transsacral plating) benefit from earlier mobilization.
* Progression to full weight-bearing is typically delayed until radiographic evidence of bridging callus is observed, usually between 8 to 12 weeks postoperatively.
* Patients managed nonoperatively or with less rigid constructs require prolonged bed rest and strict adherence to non-weight-bearing precautions to prevent fracture displacement.
Neurological Prognosis
The prognosis for neurological recovery in sacral fractures is highly variable and depends heavily on the initial mechanism of nerve injury (direct root compression vs. stretching vs. complete laceration).
- Motor and Sensory Recovery: Radicular symptoms (e.g., L5 or S1 distribution) often improve following adequate surgical decompression and stabilization.
- Autonomic Function: The return of bowel, bladder, and sexual function is notoriously poor, regardless of the treatment modality chosen. Lower sacral nerve roots (S2-S4), which control genital, anal, and rectal functions, are highly sensitive to trauma. Even with meticulous sacral laminectomy and decompression, long-term autonomic deficits are common and should be discussed extensively with the patient during preoperative counseling.
CONCLUSION
Sacral fractures and lumbosacral dislocations are formidable injuries that demand a multidisciplinary approach. A thorough clinical examination and advanced imaging are required to prevent missed diagnoses. Treatment must be highly individualized. While conservative management may suffice for stable injuries, operative intervention—ranging from percutaneous iliosacral screws to complex open lumbopelvic reconstruction and sacral laminectomy—is essential for unstable fracture-dislocations and cases with progressive neurological decline. Despite advances in surgical techniques that allow for earlier mobilization and reliable osseous union, surgeons must maintain realistic expectations regarding the recovery of bowel and bladder function.
You Might Also Like

