Pediatric Hand and Wrist Fractures: A Masterclass in Surgical Management
Key Takeaway
Operative treatment of closed pediatric hand fractures is rare due to the robust remodeling potential of the immature skeleton. However, physeal fractures, intraarticular displacements, and severe rotational deformities demand precise anatomical reduction. This guide details the indications, biomechanics, and surgical techniques for managing complex phalangeal, metacarpal, and thumb injuries, ensuring optimal functional outcomes and preventing premature physeal closure or degenerative joint disease.
GENERAL PRINCIPLES OF PEDIATRIC HAND AND WRIST FRACTURES
The indications for operative treatment of closed fractures of the hand in adults are relatively stringent, but they are exceedingly rare in the pediatric population. The robust osteogenic potential of the pediatric periosteum and the continuous growth of the physes allow for significant remodeling of angulated bones. However, this remodeling potential is strictly limited to the plane of joint motion (sagittal plane); rotational deformities and severe coronal angulations will not remodel and require precise reduction.
The critical exception to conservative management is a fracture involving the physis. Intraarticular physeal fractures demand absolute anatomical reduction to restore joint congruity and prevent the formation of a physeal bar, which leads to premature growth arrest and subsequent angular deformity.
Clinical Pearl: The timeline of physiological physeal closure must be meticulously noted. Closure generally occurs earlier in the phalanges and metacarpals compared to other physes. The pattern of closure is distal to proximal: phalanges close first, followed by metacarpals, and finally the distal radius. Once the physes have fused, a pediatric fracture must be managed with adult treatment algorithms.
When operative intervention is indicated for physeal fractures, the choice of implant and trajectory is paramount.
If internal fixation is required, smooth Kirschner wires (K-wires) are the gold standard. If threaded pins or cancellous screws must be used for compression, they must be placed parallel to the physis, crossing only the epiphysis or metaphysis, and never traversing the physis itself, to avoid tethering growth.
PHALANGEAL FRACTURES
Phalangeal fractures represent the most frequent hand fractures in children. Epidemiological data, such as that from Crick et al., demonstrates a predilection for the middle phalanx over the distal phalanx. Salter-Harris (SH) type III injuries are the most common (accounting for approximately 51% of physeal phalangeal fractures) and typically occur in older children nearing skeletal maturity (average age 13 years). Salter-Harris type II fractures are the second most common (37%), while type I fractures are relatively rare (12%).
Distal Phalanx Fractures and Mallet Equivalents
Avulsion injuries of the distal phalanx and its physis frequently produce Salter-Harris type I or type III fractures.

Adequate closed reduction of type I fractures generally yields satisfactory functional and radiographic outcomes. However, type III fractures of the distal phalanx produce a pediatric "mallet finger" equivalent.
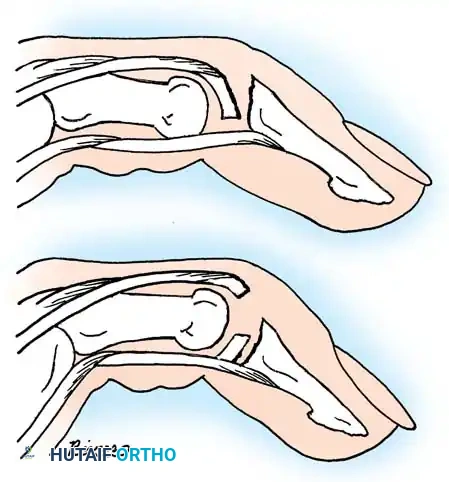
In a young child, an accurate closed reduction followed by extension splinting is usually sufficient. If anatomical reduction cannot be obtained or maintained via closed means, open reduction and internal fixation (ORIF) are strictly indicated to restore the articular surface and terminal extensor tendon continuity.
Diagnostic Pitfall: Do not mistake a Kirner congenital deformity for a distal phalangeal fracture. Kirner deformity presents as a palmar and radial curvature of the distal phalanx, typically of the small finger. Radiographs of the contralateral hand will frequently confirm the bilateral nature of this congenital anomaly.
Middle and Proximal Phalangeal Physeal Fractures
A significant percentage of physeal separations occur at the bases of the middle and proximal phalanges. The vast majority are Salter-Harris type II injuries.
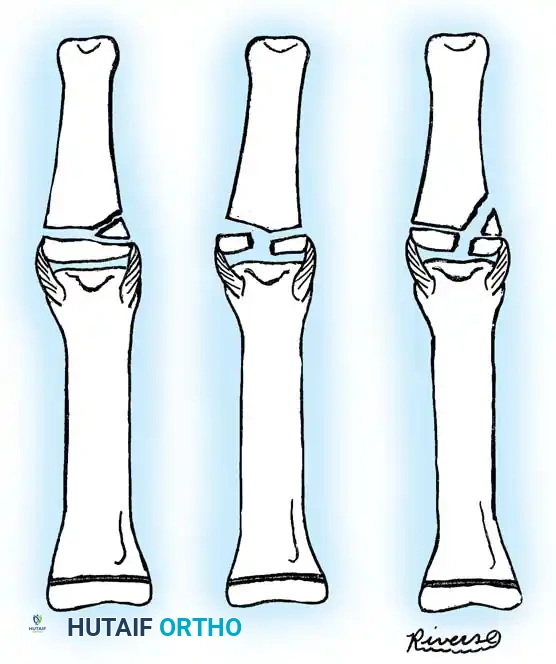
Most type II fractures can be managed successfully with closed reduction and immobilization. The intact periosteal hinge aids in reduction and provides stability. Conversely, Salter-Harris type III and the exceedingly rare type IV fractures require absolute anatomical reduction due to their intraarticular nature.

If closed reduction of a type III or IV fracture is imperfect, ORIF is mandatory. The surgical approach typically involves a mid-axial or dorsal incision, careful elevation of the extensor mechanism, and direct visualization of the articular surface. Fixation is achieved using fine, smooth K-wires (0.028 or 0.035 inch) driven parallel to the joint surface or obliquely across the fracture, minimizing physeal trauma.
Diaphyseal Phalangeal Fractures
Diaphyseal fractures of the phalanges are common and usually amenable to closed reduction and splinting (e.g., buddy taping or an intrinsic-plus splint). However, in older children or in cases of severe instability, reduction cannot be maintained, necessitating internal fixation.
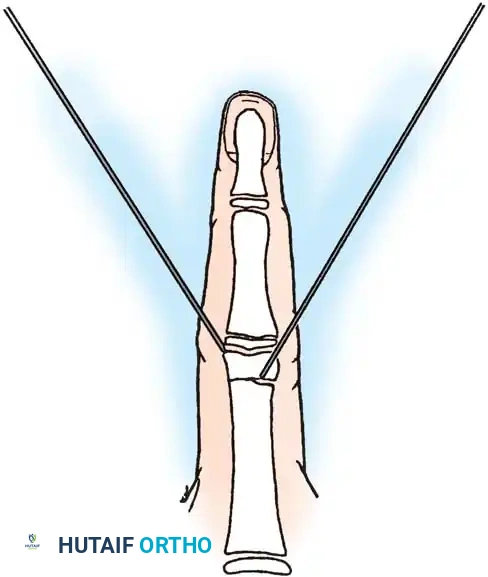
Percutaneous Pinning Technique:
1. The short distal fracture fragment is clinically aligned with the middle phalanx by gentle hyperextension of the proximal interphalangeal (PIP) joint.
2. A K-wire is aligned clinically with the middle phalanx on the lateral side and drilled into the distal fragment.
3. A second K-wire is inserted on the contralateral side at a 45-degree angle to the proximal phalanx.
4. With both K-wires secured in the distal fragment, the fracture is reduced by bringing the PIP joint into slight flexion.
5. The wires are then advanced across the fracture site to emerge at the mid-diaphysis of the proximal segment, ensuring rigid, crossed-wire stability.
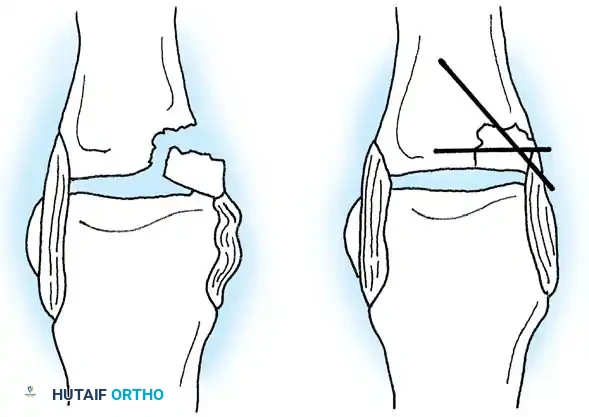
For complex Salter-Harris type III and IV avulsion fractures, Stahl and Jupiter described a highly effective figure-of-eight tension band wiring technique.
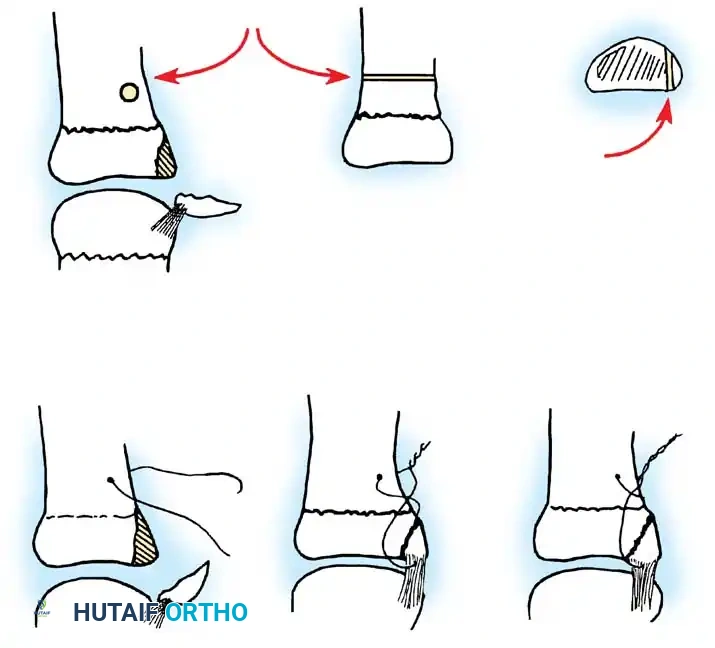
By passing a small-gauge wire through the insertion of the collateral ligament into the fracture fragment and anchoring it to the metaphysis, accurate reduction and dynamic stability are achieved. This technique allows for early mobilization while completely avoiding physeal penetration.
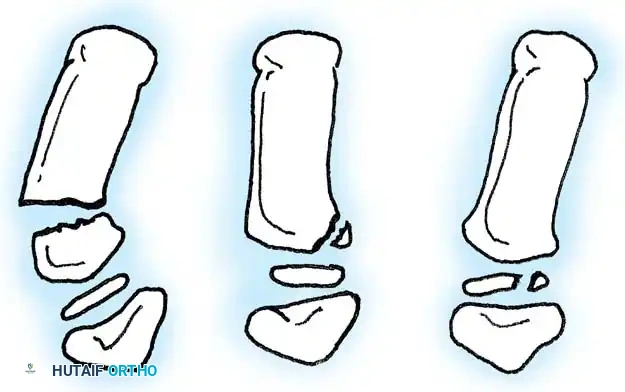
Phalangeal Neck Fractures
Phalangeal neck fractures are notorious for complications, including malunion and loss of motion. While some remodeling occurs in very young children, persistent angular deformity in an older child requires intervention. Al-Qattan classified these fractures based on the degree of displacement to guide treatment.
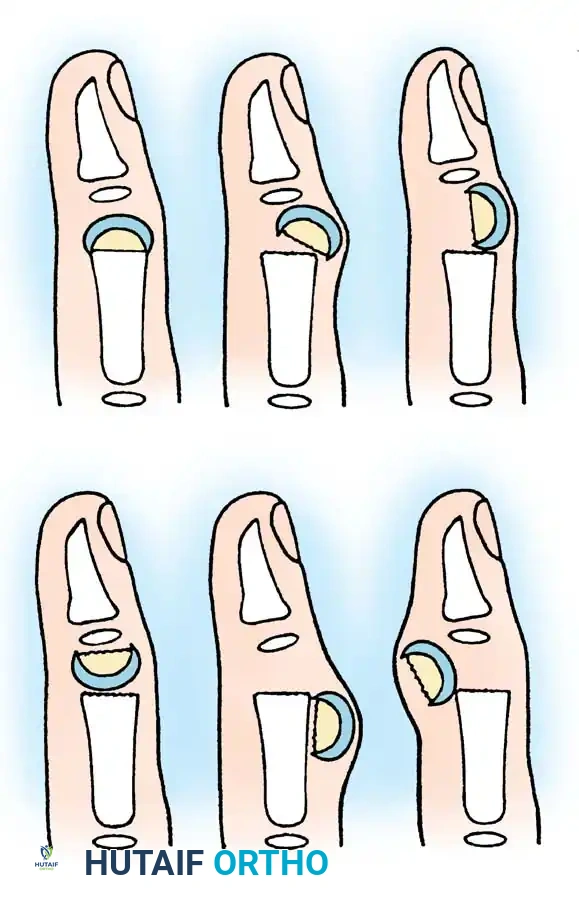
- Type I: Nondisplaced.
- Type II: Displaced but maintaining some bone-to-bone contact.
- Type III: Complete loss of bone-to-bone contact.
Displaced Type II and III fractures that cannot be adequately aligned require closed or open reduction and K-wire fixation. A critical complication, as noted by Wood and Moon, is the interposition of the volar plate.
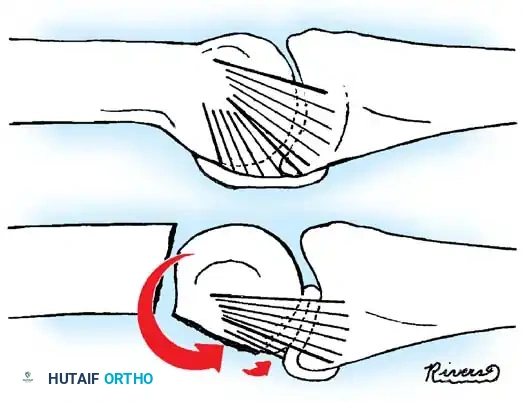
When the distal head fragment rotates and angulates dorsally, the volar plate can become entrapped between the fracture fragments, rendering closed reduction impossible. Open reduction via a mid-axial approach is required to extract the volar plate and reduce the condyles.
Intraarticular Condylar Fractures
Intraarticular fractures of the phalanges present as single condylar, T-condylar (bicondylar), or osteochondral fractures.
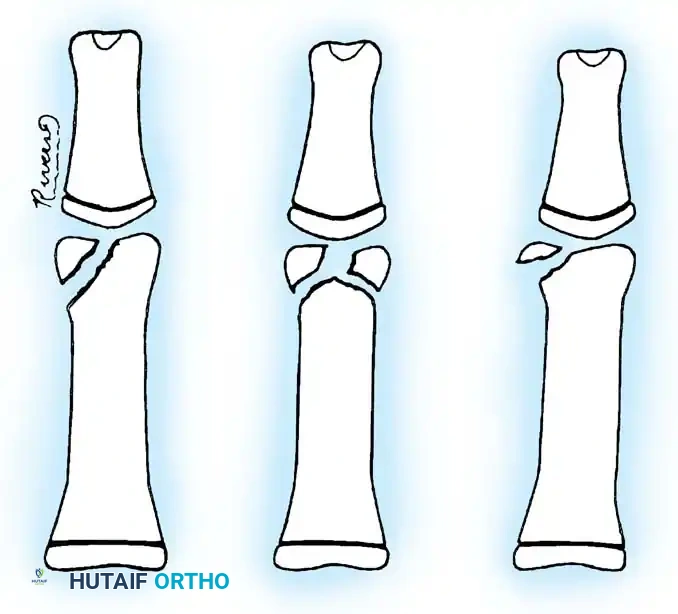
These injuries are highly unstable. If the intraarticular component is displaced and large enough to accept fixation, ORIF is indicated.

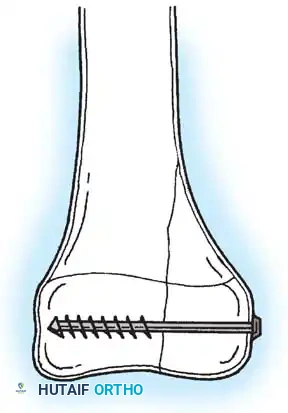
The approach is typically dorsal, splitting or elevating the extensor mechanism. The articular surface is anatomically reduced under direct vision and secured with transverse smooth K-wires or, in older adolescents, miniature headless compression screws.
METACARPAL FRACTURES
The vast majority of metacarpal base and shaft fractures in children are treated successfully with closed reduction and observation. The periosteal sleeve is thick, providing excellent stability once gross alignment is restored.
Clinical Assessment of Rotation:
Normal rotation must be confirmed clinically. When the fingers are flexed into the palm, all fingertips should point toward the scaphoid tubercle. If troublesome malrotation persists, it will not remodel. In such cases, open reduction and internal fixation are indicated. Furthermore, multiple metacarpal shaft fractures may require operative stabilization to restore the longitudinal and transverse arches of the hand.
THUMB METACARPAL FRACTURES AND DISLOCATIONS
The thumb metacarpal is unique; its primary physis is located at the base, unlike the other metacarpals where the physis is at the head. (Rarely, a pseudo-epiphysis may be present at the distal end).
Base of Thumb Fractures
Most fractures at the base of the thumb metacarpal are Salter-Harris type II injuries. These can almost universally be treated by closed reduction and immobilization in a thumb spica cast without risk of physeal arrest.
However, pediatric Bennett fractures do occur and represent Salter-Harris type III intraarticular injuries.
A Bennett fracture in a child, much like a gamekeeper's thumb equivalent, involves the avulsion of the volar ulnar base by the anterior oblique ligament. If left displaced, it will result in joint incongruity and a high risk of a bony physeal bridge. Closed reduction and percutaneous pinning (CRPP) or ORIF with smooth pins is mandatory.
In older children nearing skeletal maturity, a fracture of the base of the first metacarpal that does not involve the physis (a Rolando-type fracture) can occur.

These Y- or T-shaped intraarticular fractures can often be satisfactorily reduced with longitudinal traction and percutaneously pinned under image intensification.
🚨 SURGICAL WARNING: C-Arm Safety 🚨
When utilizing image intensification for percutaneous pinning, never use the radiolucent surface plate of the C-arm as an operating table. As reported by Waseem, Kenny, and Matthews, inadvertent penetration of the X-ray tube housing by drill bits or K-wires can result in catastrophic electrocution of both the surgeon and the patient. Always use a dedicated radiolucent hand table.
Complex Dislocations of the Thumb
While simple dislocations of the metacarpophalangeal (MCP) joint can be reduced closed, complex dislocations require open intervention.
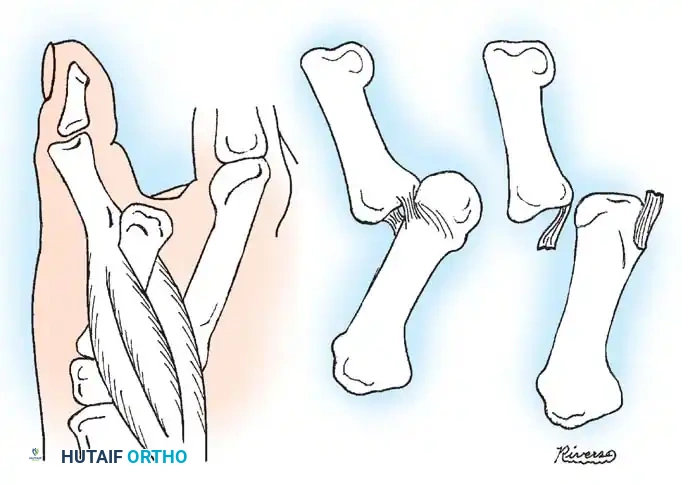
As described by Farabeuf, McLaughlin, and Green, a complex dislocation occurs when the volar plate ruptures proximally and becomes interposed in the joint space. The metacarpal head is driven volarly and becomes trapped in a tight soft-tissue noose. This noose is formed by the volar plate dorsally, the flexor pollicis brevis (FPB) radially, the adductor pollicis ulnarly, and the displaced flexor pollicis longus (FPL) tendon.
Traction exacerbates the noose effect. Open reduction, typically via a volar approach, is required to incise the A1 pulley, retract the tendons, and extract the volar plate from the joint space, allowing the metacarpal head to be reduced.
Additionally, O’Brien described a pediatric "gamekeeper thumb" variant resulting in ulnar instability of the thumb MCP joint. This can be due to a true mid-substance rupture of the ulnar collateral ligament (UCL) or, more commonly in children, a Salter-Harris type I or III physeal fracture of the proximal phalanx base.
ADVANCED CARPAL AND WRIST CONSIDERATIONS
While phalangeal and metacarpal injuries dominate pediatric hand trauma, high-energy mechanisms can occasionally result in complex carpal injuries or fracture-dislocations.

In the rare event of pediatric carpal fractures (such as scaphoid fractures in older adolescents) or severe fracture-dislocations requiring rigid fixation, the principles of adult osteosynthesis begin to apply. Headless compression screws or precise K-wire constructs must be utilized to restore carpal kinematics while respecting any remaining open physes in the distal radius or ulna.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative management of pediatric hand fractures requires a delicate balance between protecting the surgical fixation and preventing joint stiffness.
- Immobilization: Following CRPP or ORIF, the hand is typically immobilized in a bulky, non-compressive dressing reinforced with a plaster or fiberglass splint. The wrist is placed in 20-30 degrees of extension, MCP joints in 70-90 degrees of flexion, and IP joints in full extension (the intrinsic-plus or "safe" position).
- Pin Management: Smooth K-wires left protruding through the skin should be capped and kept meticulously clean to prevent pin-tract infections.
- Hardware Removal: Because pediatric bone heals rapidly, K-wires can typically be removed in the clinic at 3 to 4 weeks postoperatively, once clinical and radiographic union is evident.
- Rehabilitation: Children generally regain motion rapidly through normal play and daily activities once pins are removed. Formal occupational therapy is reserved for cases of severe intraarticular trauma, prolonged immobilization, or persistent stiffness.
By adhering to strict biomechanical principles, respecting the physis, and recognizing the specific injury patterns unique to the pediatric hand, the orthopedic surgeon can consistently achieve excellent functional outcomes and avoid lifelong deformity.
You Might Also Like


