Cervical Instability in Down Syndrome: Comprehensive Surgical Management
Key Takeaway
Cervical instability in Down syndrome arises from inherent collagen defects causing ligamentous laxity at the atlantoaxial and atlantooccipital joints. While often asymptomatic, progressive instability can lead to severe neurological compromise. Diagnosis relies on precise radiographic measurements, including the atlantodens interval and Powers ratio. Operative management is indicated for significant instability or neurological deficits, requiring meticulous surgical technique, rigid fixation, and prolonged postoperative immobilization to mitigate high rates of graft resorption.
PATHOPHYSIOLOGY AND BIOMECHANICS
Cervical instability in patients with Down syndrome (Trisomy 21) represents a complex intersection of genetic collagen abnormalities, generalized ligamentous laxity, and unique osteocartilaginous morphology. The underlying structural defect primarily involves Type VI collagen, which compromises the tensile strength and viscoelastic properties of the critical stabilizing ligaments of the upper cervical spine—most notably the transverse atlantal ligament, the alar ligaments, and the tectorial membrane.
This intrinsic laxity predisposes these patients to both atlantoaxial instability (AAI) and atlantooccipital instability (AOI). Furthermore, Pueschel et al. (1990) demonstrated a high prevalence of concurrent osseous anomalies in the upper cervical spine, reporting that 45 of 78 evaluated patients with Down syndrome exhibited structural cervical spine defects. These osseous anomalies are statistically more prevalent in patients with documented atlantoaxial instability. The academic debate remains ongoing regarding whether these osseous anomalies are the primary etiology of the instability or a secondary adaptive response to chronic ligamentous laxity and abnormal biomechanical stress.
Clinical Pearl: When evaluating a patient with Down syndrome, never assume the instability is purely ligamentous. Always maintain a high index of suspicion for concurrent osseous anomalies, such as os odontoideum, odontoid hypoplasia, or assimilation of the atlas, which fundamentally alter the surgical approach and fixation strategy.
NEUROLOGICAL EVALUATION
Despite the high radiographic prevalence of cervical instability, clinically significant neurological symptoms manifest in only 1% to 2.6% of patients. Consequently, instability is most frequently identified incidentally during routine radiographic screening or during evaluations for unrelated conditions.
When progressive instability leads to neurological compromise, it is most frequently observed in males older than 10.5 years of age, as noted by Burke et al. The clinical presentation is typically insidious, driven by repetitive microtrauma to the spinal cord or acute dynamic compression.
Signs and Symptoms
Involvement of the pyramidal tracts is the hallmark of myelopathy in this population. Clinical manifestations include:
* Gait Abnormalities: Often the first noticeable sign, presenting as a broad-based, spastic, or unsteady gait.
* Hyperreflexia: Exaggerated deep tendon reflexes, sustained clonus, and positive Babinski or Hoffmann signs.
* Motor Weakness: Progressive loss of motor milestones or declining physical endurance.
* Cervical Symptoms: Torticollis, neck pain, and severe occipital headaches.
Surgical Warning: Detailed neurological examination is notoriously difficult in patients with Down syndrome due to varying degrees of intellectual disability and communication barriers. Subtle signs of myelopathy can easily be missed or misattributed to baseline developmental delays.
To overcome these diagnostic challenges, Pueschel et al. strongly recommend the utilization of Somatosensory Evoked Potentials (SSEPs) to objectively document subclinical neurological involvement and monitor spinal cord integrity.
RADIOGRAPHIC DIAGNOSIS AND MEASUREMENTS
A rigorous, standardized radiographic protocol is mandatory for all patients with Down syndrome suspected of having cervical instability. The standard series must include high-quality anteroposterior (AP), open-mouth odontoid, and dynamic (flexion-extension) lateral radiographs.
Atlantoaxial Instability (AAI)
The primary metric for evaluating AAI is the Atlantodens Interval (ADI), measured from the posterior margin of the anterior ring of C1 to the anterior cortex of the odontoid process.
* Normal: < 3 mm in adults; < 4 mm in children.
* Instability: An ADI of > 4 to 5 mm indicates definitive ligamentous laxity and instability.
* Critical Threshold: If the ADI exceeds 6 to 7 mm, dynamic MRI or CT in flexion and extension is strictly indicated to evaluate the Space Available for the Cord (SAC), also known as the Posterior Atlantodens Interval (PADI). A SAC of < 14 mm is highly predictive of neurological compromise.
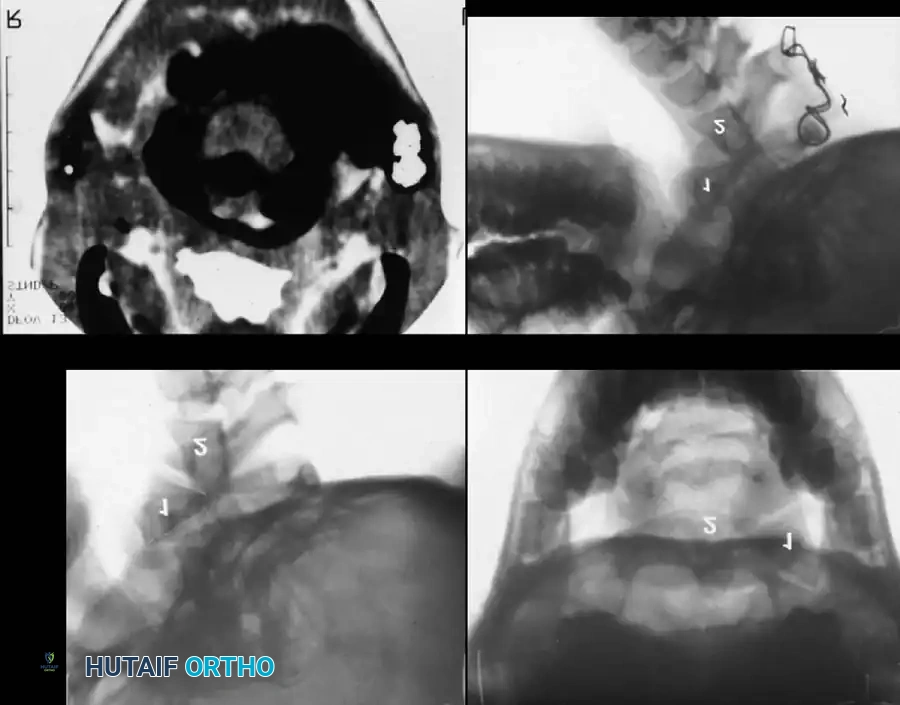
Fig. 37-33 Atlantoaxial rotatory fixation. A, Lateral radiograph shows wedge-shaped mass anterior to odontoid. B, Open-mouth odontoid view. C, CT scan. D, After C1-2 in situ fusion.
Atlantooccipital Instability (AOI)
Radiographic evidence of AOI is inherently more complex to define than AAI. However, several validated measurement techniques are essential for the orthopedic surgeon to master.
1. Wackenheim Clivus-Canal Line
This line evaluates the relationship between the cranium and the cervical canal. A line is drawn along the posterior aspect of the clivus and extended inferiorly into the cervical spinal canal. In a normal spine, this line should pass perfectly tangential to, or just posterior to, the tip of the odontoid process. Intersection with the odontoid indicates cranial settling or abnormal translation.
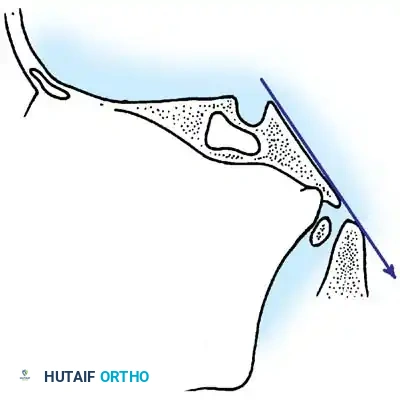
Fig. 37-34 Drawing of Wackenheim clivus-canal line. This line is drawn along the clivus into the cervical spinal canal and should pass just posterior to the tip of the odontoid.
2. Wiesel and Rothman Measurement
This technique quantifies dynamic occipitoatlantal translation. Lines are drawn on both flexion and extension lateral radiographs. The "atlantal line" joins the anterior and posterior arches of C1. A perpendicular line is drawn at the posterior margin of the anterior arch. The distance from the basion to this perpendicular line is measured in both flexion and extension. A difference (translation) of more than 1 mm is diagnostic of AOI.
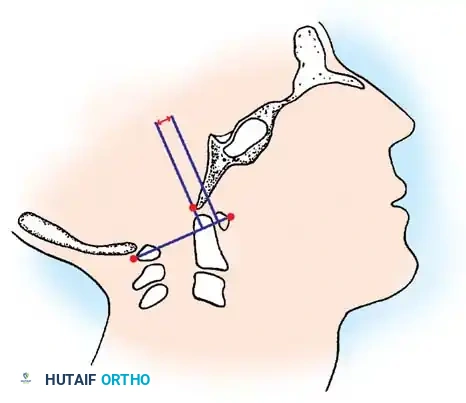
Fig. 37-35 Method of measuring atlantooccipital instability according to Wiesel and Rothman. Translation should be no more than 1 mm.
3. Powers Ratio
The Powers ratio is the most widely utilized metric for diagnosing anterior or posterior atlantooccipital translation. It is calculated by drawing two lines:
1. Line BC: From the Basion (B) to the posterior arch of the atlas (C).
2. Line OA: From the Opisthion (O) to the anterior arch of the atlas (A).
The length of line BC is divided by the length of line OA (BC/OA).
* Normal: ~0.77
* Anterior Translation: A ratio > 1.0 is diagnostic of abnormal anterior translation of the occiput.
* Posterior Translation: According to Parfenchuck et al., a ratio < 0.55 indicates abnormal posterior translation.
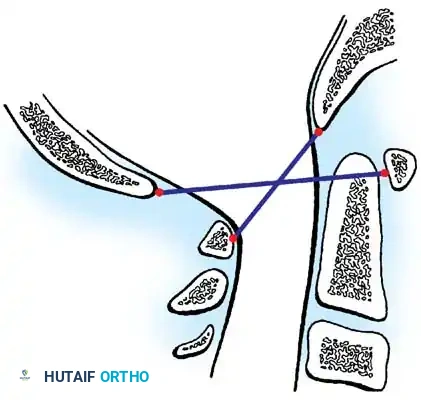
Fig. 37-36 Powers ratio. A ratio greater than 1 is diagnostic of anterior atlantooccipital translation, and a ratio less than 0.55 is diagnostic of posterior translation.
TREATMENT ALGORITHM
The management of cervical instability in Down syndrome must be highly individualized, balancing the risk of catastrophic neurological injury against the notoriously high complication rates of cervical arthrodesis in this specific patient population.
Non-Operative Management
- ADI 4 to 5 mm (Asymptomatic): Restriction of high-risk activities (e.g., gymnastics, diving, contact sports, trampoline use) is usually sufficient. Routine clinical and radiographic surveillance every 12 to 24 months is recommended.
- ADI 6 to 7 mm (Asymptomatic): This is a critical gray zone. MRI or CT must be utilized to evaluate the SAC and the presence of any subclinical cord signal changes (myelomalacia). If the SAC is preserved (>14 mm) and the cord is normal, strict activity restriction and close observation may continue, though some surgeons may advocate for prophylactic fusion depending on patient compliance and dynamic hypermobility.
Operative Management Indications
Surgical intervention (posterior cervical fusion) is strictly indicated under the following conditions:
1. Absolute: Presence of any neurological symptoms attributable to cervical instability, regardless of the absolute ADI measurement.
2. Absolute: An ADI of 10 mm or greater, as the biomechanical failure of the transverse and alar ligaments is complete, and the risk of sudden neurological compromise is unacceptably high.
3. Relative: Progressive instability on serial radiographs with a declining SAC approaching 14 mm.
SURGICAL TECHNIQUE: POSTERIOR C1-C2 ARTHRODESIS
Performing a cervical fusion in a patient with Down syndrome is fraught with unique challenges, including abnormal bone quality, anomalous vascular anatomy, and a high propensity for graft failure.
1. Preoperative Planning and Reduction
Before any surgical incision is made, the unstable C1-C2 joint must be addressed. Preoperative or intraoperative cranial traction (using Gardner-Wells tongs or a halo ring) is applied to attempt a closed reduction of the atlantoaxial subluxation.
Pitfall: Never forcefully reduce a chronic atlantoaxial subluxation. If reduction cannot be obtained safely via traction, an in situ fusion is mandatory. Attempting an intraoperative structural reduction by pulling the C1 arch posteriorly toward C2 can cause catastrophic neurological compromise if the wires or instruments are passed through a critically narrowed space available for the spinal cord.
2. Anesthesia and Positioning
- Intubation: Fiberoptic awake intubation or video laryngoscopy with manual in-line stabilization is critical. Avoid any hyperextension of the neck during airway management.
- Positioning: The patient is placed prone. The head is secured in a Mayfield skull clamp or a halo ring. The neck must be maintained in a neutral position. Neuro-monitoring (SSEPs and MEPs) should be established prior to positioning and monitored continuously.
3. Surgical Approach
- A standard posterior midline incision is made from the inion to the spinous process of C3.
- Meticulous subperiosteal dissection is performed to expose the posterior arch of C1 and the lamina and spinous process of C2.
- Vascular Warning: Dissection along the superior margin of the C1 posterior arch must not extend more than 1.5 cm lateral to the midline to avoid catastrophic iatrogenic injury to the vertebral artery as it courses through the sulcus arteriosus.
4. Instrumentation and Fusion Techniques
While modern techniques increasingly utilize rigid screw-rod constructs (e.g., C1 lateral mass screws combined with C2 pedicle or pars screws) to increase biomechanical stability, traditional wiring techniques (Gallie or Brooks-Jenkins constructs) remain highly relevant, particularly in pediatric patients with small osseous dimensions.
- Wiring Technique: If utilizing sublaminar wires, extreme caution must be exercised. The ligamentum flavum is carefully opened. Contoured titanium or stainless steel cables are passed beneath the posterior arch of C1 and the lamina of C2.
- In Situ Fusion: If the joint is irreducible, the wires are passed carefully, and structural tricortical iliac crest bone graft is fashioned to fit the existing deformity without attempting to pull the spine into anatomic alignment.
- Bone Grafting: The posterior arches of C1 and C2 are aggressively decorticated using a high-speed burr. Copious amounts of autologous cancellous bone graft (harvested from the posterior superior iliac spine) are packed laterally over the decorticated facet joints and interlaminar spaces.
POSTOPERATIVE PROTOCOL AND COMPLICATIONS
The postoperative management of Down syndrome patients requires extreme vigilance. Complications are significantly more common in this cohort compared to the general pediatric population.
Immobilization
Due to the inherent collagen defects and altered inflammatory responses in Down syndrome, bone healing is notoriously delayed. Postoperative immobilization in a rigid halo-cast or halo-vest must be continued for a minimum of 6 months. Standard rigid cervical collars are insufficient.
Complications
- Graft Resorption and Pseudarthrosis: Segal et al. reported an alarmingly high rate of graft resorption following posterior fusions in this population. They postulated that the underlying collagen defects (Type VI) and an inadequate local inflammatory response severely impair osteogenesis. Prolonged halo immobilization is the primary defense against this complication.
- Adjacent Segment Instability: Msall et al. documented the frequent development of new-onset instability at the segments immediately above (occipitoatlantal) and below (C2-C3) the fused C1-C2 segment. This occurs due to the transfer of biomechanical stress to adjacent hypermobile, ligamentously lax joints. Long-term radiographic surveillance is mandatory even after a successful arthrodesis.
- Infection and Wound Breakdown: The altered immune profile in Down syndrome increases the risk of surgical site infections, necessitating meticulous soft tissue handling and optimized postoperative nutritional support.
You Might Also Like


