Operative Management of Pediatric Pathological and Non-Accidental Fractures

Key Takeaway
Pediatric pathological fractures and non-accidental trauma require specialized orthopedic management. While conservative treatment remains common, operative intervention is increasingly indicated to minimize immobilization-induced osteopenia and morbidity. This guide details the biomechanical principles, surgical indications, and operative techniques for managing pediatric pathological fractures, including osteogenesis imperfecta, bone cysts, and child abuse injuries, emphasizing physeal preservation and anatomical reduction.
PEDIATRIC PATHOLOGICAL FRACTURES
Historically, the majority of pediatric fractures, including pathological variants, were managed non-operatively through closed reduction and casting. However, as complications associated with pediatric anesthesia and surgical site infections have precipitously decreased, the paradigm has shifted. Today, an increasing number of pathological fractures in children are treated operatively. This proactive approach significantly decreases morbidity and minimizes the deleterious effects of prolonged immobilization.
Children with underlying metabolic or genetic bone disorders should not be subjected to extended periods of cast immobilization, as the lack of mechanical loading exacerbates disuse osteopenia, creating a vicious cycle of recurrent fractures. Open reduction and internal fixation (ORIF) or intramedullary stabilization is frequently beneficial, particularly in patients with systemic bone fragility.
Indications for Operative Intervention
Operative management is strongly indicated in several specific pathological entities:
- Osteogenesis Imperfecta (OI): Patients with OI suffer from profound osteopenia and recurrent fractures. Operative intervention, typically utilizing telescoping intramedullary rods (e.g., Fassier-Duval nails), prevents progressive deformity and allows for early mobilization.
- Large Cystic Defects: Fractures through benign bone tumors, such as Unicameral Bone Cysts (UBC) or Aneurysmal Bone Cysts (ABC), often require surgical curettage, bone grafting (autograft, allograft, or synthetic substitutes), and internal fixation to prevent recurrence and ensure structural stability.
- Neurofibromatosis Type 1 (NF1): Congenital anterolateral bowing of the tibia progressing to pseudarthrosis is a hallmark of NF1. These complex non-unions require aggressive surgical resection of the hamartomatous tissue, robust bone grafting, and rigid internal or external fixation.
- Neuromuscular Disorders: Children with myelomeningocele or severe cerebral palsy frequently sustain multiple fractures of the long bones due to osteopenia and joint contractures. Operative fixation facilitates nursing care and rapid return to baseline function.
- Polytrauma and Traumatic Brain Injury (TBI): In children where conservative management is impeded by severe spasticity, head injury, or the need for intensive care access, early operative stabilization of fractures is paramount to reduce systemic inflammatory response and facilitate pulmonary care.
Clinical Pearl: In the management of pathological fractures, the surgeon must treat both the fracture and the underlying pathology. Fixation constructs must span the entire length of the abnormal bone to prevent peri-implant fractures at stress risers.
BIOMECHANICS AND PHYSEAL GROWTH CONTRIBUTIONS
A profound understanding of longitudinal bone growth is mandatory when planning operative interventions in children. The remodeling potential of a pediatric fracture is directly proportional to the age of the child and the distance of the fracture from the most active physis.
The growth contributions of the upper extremity physes are distributed as follows:
- Humerus: Approximately 80% of the longitudinal growth of the humerus occurs at the proximal physis, while only 20% occurs at the distal physis.
- Radius: The proximal physis contributes 25%, whereas the distal physis is responsible for 75% of the bone's length.
- Ulna: The proximal physis contributes 15%, and the distal physis contributes 85%.
When evaluating the total length of the upper extremity, the proximal humerus and the distal radius/ulna are the primary engines of growth. Consequently, fractures near these highly active physes possess massive remodeling potential in the sagittal and coronal planes. Conversely, rotational deformities do not remodel and must be anatomically corrected during surgery.
NON-ACCIDENTAL TRAUMA: FRACTURES CAUSED BY CHILD ABUSE
Non-accidental trauma (NAT), or child abuse, represents a critical diagnostic and legal challenge for the orthopedic surgeon. The highest incidence of child abuse occurs in infants and toddlers between birth and 2 years of age.
Diagnostic Red Flags and Pathognomonic Signs
In any child younger than 2 years old presenting with a significant fracture and a questionable, inconsistent, or delayed history of its occurrence, child abuse must be the primary differential diagnosis.
To rule out or confirm this possibility, a comprehensive skeletal survey (and often a bone scan) is strictly indicated.
Pathognomonic Radiographic Findings:
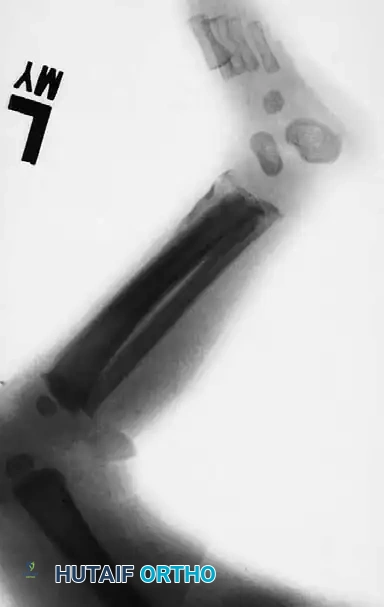
1. Multiple Fractures in Different Stages of Healing: The presence of acute fractures alongside fractures exhibiting mature callus formation almost always indicates repeated episodes of non-accidental trauma.
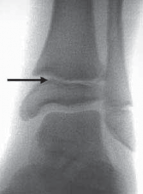
2. Epiphyseal-Metaphyseal ("Corner" or "Bucket-Handle") Fractures: These are highly specific to child abuse. They result from violent pulling, twisting, and shearing forces applied to the infant's limbs, which are rarely replicated in accidental trauma.
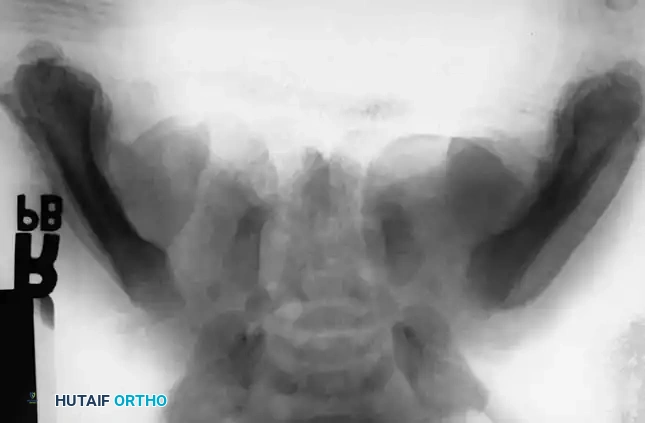
3. Posterior Rib Fractures: Caused by aggressive squeezing of the infant's thorax.
4. Complex Skull Fractures: Especially those crossing suture lines.

Pathognomonic Clinical Findings:
* Multiple areas of large ecchymoses in different stages of resolution (ranging from black and blue to brown and green).
* Associated non-orthopedic injuries: skin burns (cigarette burns, immersion burns), ocular changes (retinal hemorrhages indicative of shaken baby syndrome), hematuria, and intra-abdominal injuries.

The Role of the Orthopedic Surgeon in NAT
The most common sites of fractures caused by child abuse are the diaphyseal regions of the humerus, tibia, and femur.
Every jurisdiction requires physicians to act as mandated reporters of suspected child abuse. Definite knowledge or a confirmed specific diagnosis is not required to make a report; reasonable clinical suspicion is sufficient.
Surgical Warning: It is a tragic reality that few fractures in this demographic strictly require open reduction and internal fixation from a purely biomechanical standpoint. However, admission for surgical management or observation often serves a dual purpose: it provides optimal orthopedic care while simultaneously sheltering the abused child from their abusers until child protective services can intervene.
Regardless of the treatment modality chosen, the orthopedic surgeon's paramount duty is to protect the child. The surgeon must inform the parents or guardians of their legal and ethical responsibility to report the injuries to the appropriate authorities.
GENERAL PRINCIPLES OF OPERATIVE FRACTURE TREATMENT IN CHILDREN
While the threshold for surgery has lowered, it remains true that the majority of pediatric fractures do not require open reduction and internal fixation. When operative intervention is deemed necessary—whether for pathological fractures, polytrauma, or irreducible injuries—the surgeon must adhere to strict, pediatric-specific surgical principles.
1. Do Not Overestimate Remodeling Potential
Do not fall into the trap of assuming that all fractures in children will remodel completely. While sagittal and coronal plane deformities near active physes remodel well, rotational deformities, intra-articular step-offs, and deformities in older children (nearing skeletal maturity) will not. Adequate, anatomical reduction remains the gold standard.
2. Master the Surgical Anatomy of the Physes
The physis is not a simple, flat cartilaginous plate. Each physis is highly undulated, featuring complex mammillary processes that interlock with the metaphysis to provide shear stability. Furthermore, the perichondrial ring (Zone of Ranvier) is critical for latitudinal growth. Surgical approaches must respect these structures to prevent iatrogenic growth arrest.
3. Anatomical Reduction at the Physis is Mandatory
If an open reduction is necessary for a physeal injury (e.g., Salter-Harris III or IV), the fragments must be repositioned as anatomically as possible. The cartilaginous fragment must be perfectly aligned; otherwise, the resulting step-off will lead to the formation of a transphyseal bony bridge (bar) and subsequent joint incongruity or angular deformity.
4. Optimize Fixation: Adequate but Minimal
Use adequate fixation to achieve stability, but do not use more hardware than is absolutely necessary. The goal is to provide enough stability to allow for early mobilization, but excessive periosteal stripping or bulky implants can compromise the delicate pediatric blood supply and complicate future hardware removal.
5. Plan for Hardware Removal
Unlike in adults, where hardware is often left in situ permanently, pediatric implants frequently require removal to prevent tethering of growth or interference with future bone development. Use fixation devices that can be removed readily and plan your initial incisions with future removal in mind.
6. Utilize Smooth Pins
When crossing or operating near a physis, strictly use smooth Kirschner wires (K-wires) or Steinmann pins rather than threaded pins. Threaded pins cause significant mechanical damage to the resting zone of the physeal cartilage upon insertion and removal, drastically increasing the risk of premature physeal closure.
7. Trajectory: Parallel the Physis or Pin the Metaphysis
Whenever biomechanically feasible, try not to cross the physis with fixation.
* For epiphyseal fractures, place screws or pins parallel to the physis entirely within the epiphysis.
* For metaphyseal fractures, confine the fixation to the metaphysis.
* If crossing the physis is unavoidable (e.g., supracondylar humerus fractures or slipped capital femoral epiphysis), use the smallest diameter smooth pins possible, cross the physis at a 90-degree angle to minimize the cross-sectional area of damage, and remove the pins as soon as clinical union is achieved.
8. Avoid Unnecessary Drill Holes
Pediatric bone, particularly in pathological states like osteogenesis imperfecta or cystic lesions, is highly susceptible to stress risers. Avoid unnecessary drill holes or multiple passes with K-wires, as these cortical defects can easily become the epicenter of iatrogenically created pathological fractures during the postoperative rehabilitation phase.
9. Prevent Intra-Articular Pin Penetration
Meticulous fluoroscopic evaluation in multiple orthogonal planes is required to ensure that pins and screws do not penetrate the joint space. Intra-articular hardware leads to chondrolysis, septic arthritis, and devastating early-onset osteoarthritis.
10. Meticulous Soft Tissue Handling and Closure
Pediatric skin and soft tissues are delicate. Use a plastic surgery-type closure utilizing buried, absorbable sutures (e.g., Monocryl or Vicryl) for the dermal and epidermal layers. This eliminates the anxiety and trauma associated with suture or staple removal in the clinic for a young child.
11. Anticipate Noncompliance
A young child cannot be expected to adhere to weight-bearing restrictions or activity modifications. The surgical construct, combined with postoperative casting (e.g., a well-molded spica cast or long-leg cast), must be robust enough to immobilize a noncompliant child adequately.
12. Vigilant Neurovascular Monitoring
During the acute convalescent period, pediatric patients are at a high risk for compartment syndrome, particularly following tibial or supracondylar humerus fractures. Watch for neurovascular insufficiency meticulously. Increasing analgesic requirements in a previously comfortable child is the earliest and most reliable sign of impending compartment syndrome.
13. Comprehensive Parental Counseling
Manage expectations proactively. Warn parents about early operative complications (infection, loss of reduction, compartment syndrome) and late complications (bony bridge formation, angular deformity, limb length discrepancy, and osteonecrosis) before they develop. Document these discussions thoroughly. A parent informed preoperatively is an ally; a parent informed postoperatively is an adversary.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative management of pediatric pathological and non-accidental fractures requires a multidisciplinary approach.
- Immobilization: Depending on the stability of the internal fixation, supplemental casting is often utilized for 3 to 6 weeks. In cases of flexible intramedullary nailing (ESIN) for diaphyseal fractures, early mobilization may be permitted if the construct is rotationally stable.
- Medical Management: For pathological fractures related to metabolic bone disease (e.g., OI), coordination with pediatric endocrinology for bisphosphonate therapy (e.g., pamidronate or zoledronic acid) is crucial to increase bone mineral density and reduce future fracture risk.
- Social Services: In cases of NAT, the child must not be discharged until a formal safety plan is established by child protective services and the hospital's child abuse pediatrics team.
- Long-Term Surveillance: Pediatric patients with physeal injuries or pathological fractures require long-term radiographic follow-up (often until skeletal maturity) to monitor for growth arrest, hardware migration, or recurrent deformity. Scanograms or orthoroentgenograms should be utilized to track limb length discrepancies.
===CONTENT===
You Might Also Like