Orthopaedic Fracture & Soft-Tissue Classification Guide

Key Takeaway
Accurate fracture and soft-tissue classification is the cornerstone of orthopaedic traumatology. It dictates surgical decision-making, predicts prognostic outcomes, and standardizes academic communication. This guide comprehensively details the AO/OTA alphanumeric system, the Gustilo-Anderson criteria for open fractures, and the Tscherne classification, providing evidence-based frameworks for surgical approaches, fixation strategies, and postoperative protocols in complex musculoskeletal trauma.
THE PHILOSOPHY AND UTILITY OF FRACTURE CLASSIFICATION
In the realm of orthopaedic traumatology, the classification of fractures is far more than an academic exercise; it is the foundational blueprint for surgical decision-making. When combined with a rigorous assessment of the surgeon’s capabilities, institutional facilities, available resources, and the patient’s physiological profile, an accurate classification of the fracture and its associated soft-tissue envelope allows for the determination of the optimal treatment algorithm.
Analysis of the fracture pattern reveals the precise amount of kinetic energy imparted to the extremity, predicts the inherent biomechanical stability of the fracture after reduction, and alerts the surgeon to high-risk patterns of injury that may compromise limb salvage. Furthermore, standardized classification systems allow surgeons to monitor longitudinal outcomes, compare treatment efficacies across international cohorts, and provide a validated basis for the evaluation of novel osteosynthesis methods.
Clinical Pearl: A fracture is not merely a "broken bone"; it is a severe soft-tissue injury that happens to involve underlying osseous failure. The soft-tissue envelope dictates the timing, approach, and method of surgical fixation.
The extensive Orthopaedic Trauma Association (OTA) classification correlates the coding of the fracture with expanded diagnostic codes, ensuring standardized documentation. Where applicable, it incorporates historically validated, anatomically specific classification systems, such as the Judet and Letournel classification for acetabular fractures and the Neer classification for proximal humeral injuries.
BIOMECHANICS AND MORPHOLOGY OF FRACTURE PATTERNS
Understanding the morphological characteristics of a fracture provides direct insight into the mechanism of injury and the biomechanical forces required for stable osteosynthesis.
- Transverse Fractures: Result from direct, high-energy bending forces. They possess excellent compressive stability but poor torsional stability.
- Oblique Fractures: Result from combined bending and axial compression. They are inherently unstable under axial loads, prone to shortening and shear.
- Spiral Fractures: Caused by low-energy torsional forces. They often have a large surface area for healing but require neutralization of rotational forces during fixation.
- Comminuted Fractures: Indicate high-energy transfer resulting in multiple fragments (e.g., butterfly fragments). These require load-bearing implants (like intramedullary nails or bridge plates) as the bone cannot share the mechanical load.
- Segmental Fractures: Two distinct fracture lines isolating a diaphyseal segment. The middle segment is highly susceptible to avascular necrosis due to the disruption of both endosteal and periosteal blood supplies.
- Bone Loss: Critical defects requiring advanced reconstructive techniques, such as bone grafting, Masquelet induced-membrane technique, or distraction osteogenesis (Ilizarov).
THE AO/OTA ALPHANUMERIC CLASSIFICATION SYSTEM
The AO (Arbeitsgemeinschaft für Osteosynthesefragen) alphanumeric classification, originally published by Müller et al., is the result of an exhaustive international effort based on data from the AO Documentation Center. It remains the gold standard for diaphyseal and articular fracture classification.
This system is predicated on morphological characteristics and precise anatomical location. It utilizes a standardized grid:
1. Bone: 1 (Humerus), 2 (Radius/Ulna), 3 (Femur), 4 (Tibia/Fibula).
2. Segment: 1 (Proximal), 2 (Diaphyseal), 3 (Distal).
3. Type:
* A: Simple fractures (transverse, oblique, spiral). The bone retains some load-sharing capacity once reduced.
* B: Wedge fractures (intact wedge, fragmentary wedge). There is some cortical contact between the main proximal and distal fragments after reduction.
* C: Complex/Multifragmentary fractures. No contact exists between the main proximal and distal fragments after reduction; the implant must bear the entire mechanical load.
Surgical Warning: While the AO/OTA system is extremely reliable at the primary A, B, and C levels, interobserver and intraobserver reliability significantly decreases when categorizing into the more complex subgroups (e.g., C1 vs. C2 vs. C3).
Swiontkowski et al., in an evaluation of the AO/OTA system, demonstrated that patients with C-type fractures exhibited significantly worse functional performance and higher impairment compared to those with B-type fractures. However, outcomes between B-type and A-type fractures were not always significantly different, suggesting that while the system is morphologically precise, its prognostic value for functional impairment in isolated unilateral lower extremity fractures has limitations.
CLASSIFICATION OF SOFT-TISSUE INJURIES
Just as the osseous injury must be meticulously classified to validate comparative studies, the associated soft-tissue injury must be graded to dictate surgical timing and approach. The soft-tissue envelope is the primary determinant of infection risk, fracture union, and ultimate limb survival.
The Gustilo-Anderson Classification for Open Fractures
Described in 1976 and modified in 1984 based on a review of 1,025 open fractures, the Gustilo-Anderson system remains the most widely utilized grading scheme for open wounds. It provides critical prognostic information regarding the risk of deep infection and osteomyelitis. The classification is based on wound size, degree of soft-tissue damage, periosteal stripping, and vascular compromise.
- Type I: Clean wound less than 1 cm long. Typically a low-energy, inside-out injury. Minimal muscle contusion.
- Type II: Laceration greater than 1 cm long, without extensive soft-tissue damage, skin flaps, or avulsions. Moderate energy.
Fig. 50-2A: Type I open fracture of patella and type II open fracture of tibial shaft, demonstrating localized, relatively clean wounds without massive soft-tissue avulsion.
- Type IIIA: Extensive soft-tissue lacerations or flaps, but maintaining adequate soft-tissue coverage of the fractured bone. This category inherently includes all high-energy traumas (e.g., farm injuries, high-velocity gunshot wounds), segmental fractures, or severely comminuted fractures, regardless of the actual size of the skin wound.

Fig. 50-2B: Type IIIA open fracture with extensive laceration of skin and muscles that involves almost the entire leg, yet local coverage remains viable.

Fig. 50-2C: Type IIIA open tibial fracture with extensive periosteal stripping but without massive environmental contamination.
- Type IIIB: Extensive soft-tissue loss with severe periosteal stripping and bony exposure. These injuries are usually massively contaminated and require a rotational or free muscle flap (e.g., gastrocnemius, soleus, or free latissimus dorsi) for coverage.

Fig. 50-2D: Type IIIB open fracture of the tibia stabilized with external fixation. Note the massive soft-tissue defect requiring subsequent flap coverage.
- Type IIIC: Any open fracture associated with an arterial injury that requires formal vascular repair for limb salvage, regardless of the size of the soft-tissue wound.
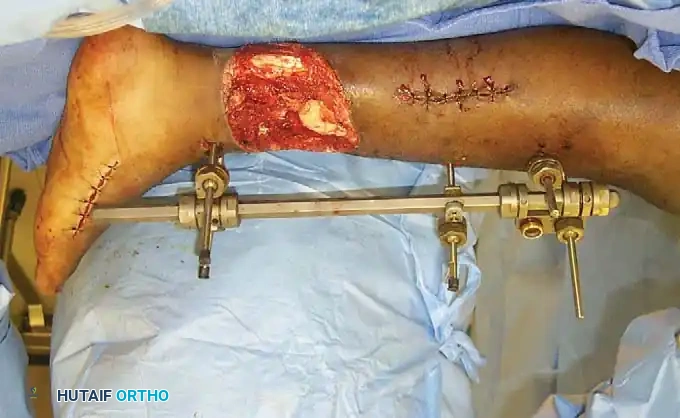
Fig. 50-2E: Type IIIC fracture of the proximal third of the humerus, involving catastrophic soft-tissue and neurovascular disruption.
Pitfall: Multiple studies, including those by Brumback and Jones, and Horn and Rettig, have demonstrated that the Gustilo classification suffers from "moderate to poor" interobserver agreement when assessed in the emergency department. Classification should only be finalized in the operating room after thorough surgical debridement.
The Tscherne Classification
Widely utilized in Europe and adopted by the AO-ASIF group, the Tscherne classification is vital because it addresses the severity of soft-tissue injury in closed fractures—a factor frequently overlooked by other systems.
Tscherne Classification for Closed Fractures:
* Grade 0: Minimal soft-tissue damage. Indirect violence (e.g., simple torsion).
* Grade 1: Superficial abrasion or contusion caused by pressure from within. Mild to moderate fracture severity.
* Grade 2: Deep, contaminated abrasion associated with localized skin or muscle contusion. Impending compartment syndrome may be present.
* Grade 3: Extensive skin contusion or crushing, underlying muscle damage, subcutaneous avulsion (Morel-Lavallée lesion), or established compartment syndrome. Severe fracture comminution.
Tscherne Classification for Open Fractures:
* Grade 1: Skin lacerations caused by a bone fragment from inside; little or no contusion of skin.
* Grade 2: Any type of skin laceration with circumscribed skin or soft-tissue contusion and moderate contamination.
* Grade 3: Severe soft-tissue damage, often with major vessel/nerve injury. Includes all fractures accompanied by ischemia, severe comminution, or compartment syndrome.
* Grade 4: Subtotal and total amputation (separation of all important anatomical structures, especially major vessels with total ischemia).
SURGICAL INSTRUCTIONS: INTEGRATING CLASSIFICATION INTO PRACTICE
The true value of these classification systems lies in their direct application to surgical technique, patient positioning, and postoperative care.
1. Indications and Fixation Strategies
- AO Type A (Simple): Amenable to load-sharing devices. Intramedullary nailing (IMN) is preferred for diaphyseal fractures. Absolute stability (lag screw and neutralization plate) is indicated for articular extensions.
- AO Type C (Complex): Requires load-bearing constructs. Bridge plating techniques (MIPO - Minimally Invasive Plate Osteosynthesis) are utilized to bypass the zone of comminution, preserving the fracture hematoma and periosteal blood supply.
- Gustilo IIIB/IIIC & Tscherne Grade 3 (Closed): Immediate internal fixation is often contraindicated due to the high risk of deep infection and wound breakdown. Damage Control Orthopaedics (DCO) is indicated: rapid application of a spanning external fixator, aggressive serial debridements, and delayed definitive internal fixation once the soft-tissue envelope has stabilized (the "wrinkle sign" appears).
2. Patient Positioning and Fluoroscopy
- Positioning must account for the planned surgical approach, which is dictated by the fracture classification. For example, a Letournel classified posterior-wall acetabular fracture requires the patient in a prone or lateral decubitus position for a Kocher-Langenbeck approach.
- Ensure the radiolucent table allows for unimpeded orthogonal fluoroscopic views. The C-arm must be positioned to visualize the joint above and below the fracture to rule out associated injuries (e.g., a Maisonneuve fracture in the setting of a complex ankle injury).
3. Step-by-Step Surgical Approach Principles
- Incision Planning: For Tscherne Grade 2/3 closed fractures, incisions must avoid zones of severe contusion or fracture blisters. Utilize angiosome-sparing approaches.
- Debridement (Open Fractures): Extend the traumatic wound longitudinally. Systematically debride from superficial to deep: skin, fat, fascia, muscle, and bone. Assess muscle viability using the "4 C's": Color, Consistency, Contractility, and Capacity to bleed.
- Reduction: Utilize indirect reduction techniques (e.g., femoral distractor, traction pins) for AO Type C fractures to avoid stripping the remaining periosteal attachments of comminuted fragments.
- Fixation: Apply the chosen construct. If using a bridge plate, ensure adequate working length (ratio of plate length to fracture length > 3:1 in comminuted fractures) to minimize strain at the fracture site and promote secondary bone healing via callus formation.
4. Postoperative Protocols
- Wound Management: Gustilo IIIB/C wounds require negative pressure wound therapy (NPWT) and planned return to the OR within 48-72 hours for repeat debridement and definitive soft-tissue coverage (flap) within 5 to 7 days.
- Weight-Bearing:
- AO Type A (IMN fixed): Often allowed immediate weight-bearing as tolerated, as the implant shares the load with the cortically reduced bone.
- AO Type C (Bridge Plated): Restricted to non-weight-bearing or touch-down weight-bearing for 6-8 weeks until radiographic evidence of bridging callus is observed, preventing catastrophic implant failure due to fatigue.
- Antibiotic Prophylaxis: Gustilo I/II receive first-generation cephalosporins for 24 hours. Gustilo III injuries require the addition of an aminoglycoside (and penicillin for farm injuries to cover Clostridium) for 72 hours or 24 hours post-soft-tissue coverage.
INJURY SEVERITY SCORING AND POLYTRAUMA
Fracture classification must be contextualized within the patient's overall physiological state. Injury severity scoring systems attempt to quantify the magnitude of multiple injuries to predict survival and guide the timing of orthopaedic interventions (Early Total Care vs. Damage Control Orthopaedics).
- Injury Severity Score (ISS): Calculates severity based on the sum of the squares of the highest Abbreviated Injury Scale (AIS) scores in the three most severely injured body regions. An ISS > 15 indicates major trauma; ISS > 40 is associated with high mortality.
- Revised Trauma Score (RTS): A physiological scoring system based on the Glasgow Coma Scale (GCS), systolic blood pressure, and respiratory rate.
- NISSSA Score: Evaluates Nerve Injury, Ischemia, Soft-Tissue Injury, Skeletal Injury, Shock, and Age. It is highly predictive of the need for amputation in severe lower extremity trauma, often outperforming the traditional MESS (Mangled Extremity Severity Score).
While many of these systems historically treated the musculoskeletal system as a single variable regardless of the number of fractures, modern trauma algorithms recognize that the cumulative inflammatory burden (the "second hit" phenomenon) of multiple long-bone fractures profoundly impacts the incidence of Acute Respiratory Distress Syndrome (ARDS) and Multi-Organ Failure (MOF). Therefore, precise fracture and soft-tissue classification remains the critical first step in navigating the complex resuscitation and reconstruction of the polytraumatized patient.
You Might Also Like
