Broken Bones & Bone Fractures: Your Guide to Causes, Types & Recovery
Key Takeaway
For anyone wondering about Broken Bones & Bone Fractures: Your Guide to Causes, Types & Recovery, Bone fractures, also known as broken bones, occur when a bone is damaged or broken in at least one place. These injuries are typically caused by traumas such as falls, car accidents, or sports injuries. Medical conditions or repetitive forces can also increase risk. Recovery time depends on the bone, fracture location, and its cause.
Introduction and Epidemiology
Osseous disruptions, clinically defined as bone fractures, represent a fundamental pathology within orthopedic surgery and traumatology. The management of these injuries requires a profound understanding of bone biology, biomechanics, and precise surgical technique. Fracture epidemiology classically demonstrates a bimodal distribution. High-energy trauma, such as motor vehicle collisions and severe falls, predominantly affects the younger demographic, particularly males in their second and third decades of life. Conversely, low-energy fragility fractures secondary to osteopenia and osteoporosis are overwhelmingly prevalent in the geriatric population, with a higher incidence in postmenopausal females.

The clinical evaluation of fractures necessitates rigorous classification to guide treatment and predict outcomes. The AO Foundation and Orthopaedic Trauma Association (AO/OTA) alphanumeric classification system remains the universal standard. This system categorizes fractures based on anatomical location, segment, and morphological characteristics, progressing from simple, low-energy patterns (Type A) to complex, multi-fragmentary, high-energy articular disruptions (Type C). Furthermore, soft tissue assessment is paramount. Closed fractures are evaluated using the Tscherne classification, which grades the extent of soft tissue contusion and degloving, while open fractures are universally stratified using the Gustilo-Anderson classification, dictating the urgency of debridement and appropriate antibiotic prophylaxis.
The distinction between a macroscopic fracture and a microtrabecular injury, often radiographically occult and historically termed a bone contusion, relies on advanced imaging modalities such as Magnetic Resonance Imaging (MRI). Microtrabecular fractures involve localized hemorrhage and edema within the cancellous bone without cortical disruption. While these injuries do not require surgical stabilization, they indicate significant energy transfer and are frequently associated with concomitant ligamentous pathology, necessitating comprehensive joint evaluation.
Surgical Anatomy and Biomechanics
Vascular Anatomy of Bone
A meticulous understanding of osseous vascularity is critical for successful fracture management and the prevention of nonunion or avascular necrosis. Long bones receive their blood supply from three primary sources. The nutrient artery system provides approximately seventy to eighty percent of the arterial supply to the diaphyseal cortex, perfusing the inner two-thirds of the cortical bone via the Haversian and Volkmann canal systems. The periosteal capillary network supplies the outer one-third of the cortex and becomes increasingly vital following trauma, as the nutrient artery is frequently disrupted during the initial fracture event or subsequent intramedullary reaming. Finally, the metaphyseal and epiphyseal vessels supply the cancellous bone ends. Surgical approaches and fixation strategies must prioritize the preservation of periosteal attachments to optimize the biological environment for fracture healing.
Biomechanics of Fracture Patterns
Fracture morphology is directly dictated by the biomechanical forces applied to the bone at the time of injury. Understanding these vectors aids in selecting the appropriate fixation construct to neutralize deforming forces.
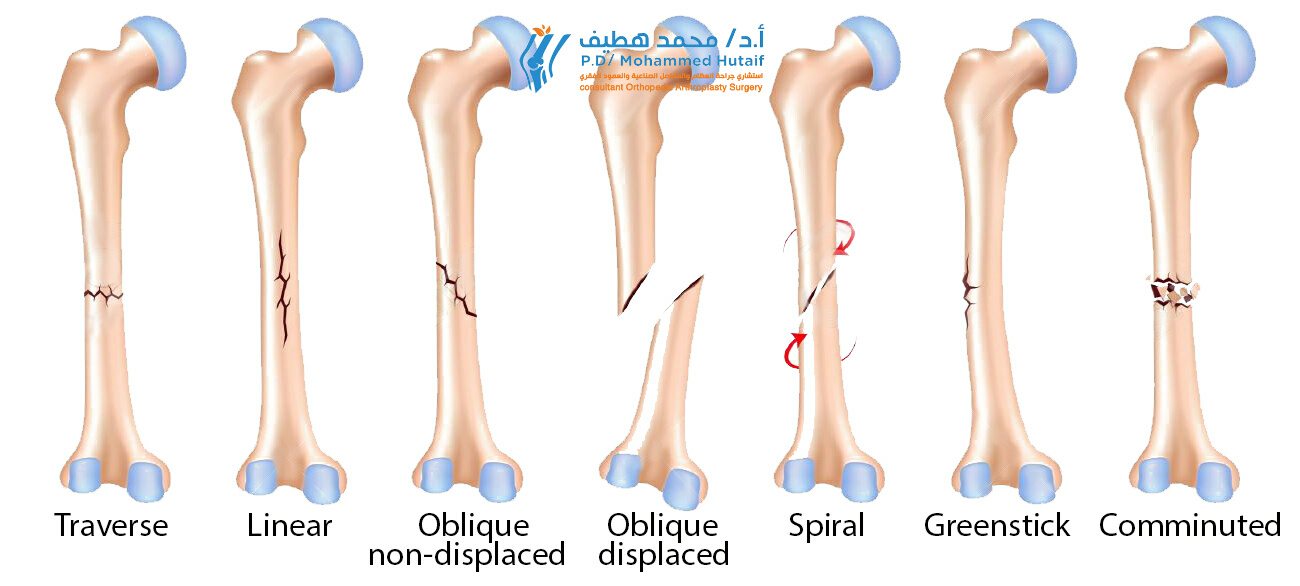
- Tension Forces result in transverse fracture patterns. The bone fails under distraction, and the resulting fracture line is perpendicular to the long axis of the bone.
- Compression Forces typically produce oblique fractures. As the bone is compressed, it fails along a shear plane, usually at a forty-five-degree angle to the applied load.
- Torsional Forces generate spiral fractures. Rotational stress causes the bone to fail in tension along a helical path.
- Bending Forces create butterfly or wedge-shaped fragments. The convex side of the bone fails in tension, while the concave side fails in compression, resulting in a distinct triangular fragment.
Principles of Bone Healing
Fracture healing occurs via two distinct biological pathways, dictated by the mechanical stability of the fixation construct as described by Perren’s strain theory.
Primary bone healing, or direct healing, occurs under conditions of absolute stability with interfragmentary strain less than two percent. This environment is typically achieved through anatomic reduction and interfragmentary compression using lag screws and compression plates. In this scenario, there is no callus formation. Osteoclasts form cutting cones across the fracture site, followed immediately by osteoblasts depositing new lamellar bone (contact healing) or filling small gaps with woven bone that is subsequently remodeled (gap healing).
Secondary bone healing, or indirect healing, occurs under conditions of relative stability with interfragmentary strain between two and ten percent. This is the physiological mechanism of bone repair and is facilitated by constructs such as intramedullary nails, bridge plates, and external fixators. Secondary healing progresses through distinct phases including hematoma formation, inflammatory response, soft callus (cartilaginous) formation, hard callus (woven bone) formation, and eventual remodeling into lamellar bone according to Wolff's Law.
Indications and Contraindications
The decision to pursue operative intervention for a fracture depends on patient-specific physiological factors, the mechanical demands of the affected extremity, and the inherent stability of the fracture pattern. The overarching goal of orthopedic trauma surgery is to restore functional anatomy, permit early mobilization, and prevent the sequelae of prolonged immobilization.
Operative Versus Non Operative Management
| Clinical Scenario | Operative Management Indications | Non Operative Management Indications |
|---|---|---|
| Articular Involvement | Intra-articular step-off greater than 2mm | Nondisplaced or extra-articular fractures with stable morphology |
| Soft Tissue Status | Open fractures requiring debridement and stabilization | Intact soft tissue envelope with acceptable alignment |
| Polytrauma | Need for early mobilization to prevent ARDS and DVT | Isolated injury in a patient compliant with weight-bearing restrictions |
| Fracture Stability | Unstable patterns (e.g. segmental, highly comminuted) | Stable patterns (e.g. transverse diaphyseal with adequate cortical contact) |
| Neurovascular Status | Vascular compromise requiring repair and skeletal stabilization | Intact neurovascular examination |
| Special Considerations | Pathological fractures, impending compartment syndrome | Severe medical comorbidities precluding anesthesia |
Absolute and Relative Contraindications
Absolute contraindications to immediate internal fixation include active, untreated infection at the surgical site and severe physiological instability. In polytraumatized patients presenting with the lethal triad of hypothermia, coagulopathy, and acidosis, prolonged definitive surgical procedures are contraindicated. These patients require Damage Control Orthopedics (DCO), utilizing rapid external fixation to stabilize skeletal injuries, minimize hemorrhage, and reduce the systemic inflammatory response until physiological optimization is achieved.
Relative contraindications include severe peripheral vascular disease, profound osteopenia that compromises implant purchase, and non-ambulatory baseline functional status where the risks of surgery outweigh the benefits of anatomic restoration.
Pre Operative Planning and Patient Positioning
Imaging and Templating
Comprehensive preoperative planning is the cornerstone of successful osteosynthesis. Standard orthogonal radiographs (anteroposterior and lateral views) of the injured segment, incorporating the joints above and below the fracture, are mandatory. For periarticular fractures, highly comminuted patterns, or fractures involving complex anatomy such as the pelvis and acetabulum, thin-slice Computed Tomography (CT) with two-dimensional and three-dimensional reconstructions is essential to delineate articular step-offs and occult fracture lines.
Digital templating must be performed routinely. This involves superimposing digital templates of various implants over the scaled preoperative radiographs to determine the optimal implant size, screw lengths, and anticipated reduction trajectory. Templating also aids in anticipating the required surgical inventory, including specialized reduction clamps, bone graft substitutes, and backup fixation options.
Patient Positioning and Fluoroscopy
Optimal patient positioning facilitates surgical exposure, fracture reduction, and unhindered fluoroscopic imaging. The choice of table (radiolucent flat table versus fracture table with traction capabilities) depends on the specific fracture and planned intervention.
For intramedullary nailing of diaphyseal femur or tibia fractures, a fracture table allows for skeletal traction to assist with indirect reduction and maintenance of length during reaming and nail insertion. Alternatively, a flat radiolucent table may be utilized with manual traction or a femoral distractor.
The fluoroscopy unit (C-arm) must be positioned to allow orthogonal imaging of the entire bone without moving the patient or compromising the sterile field. The surgeon, assistant, and scrub technician must coordinate the placement of the C-arm base and monitors to ensure ergonomic workflow and clear visualization throughout the procedure.
Detailed Surgical Approach and Technique
The surgical management of fractures is broadly divided into techniques providing absolute stability for articular fractures and techniques providing relative stability for diaphyseal fractures. The following sections detail the principles and execution of these distinct approaches.
Soft Tissue Management and Internervous Planes
Surgical approaches must respect the soft tissue envelope and utilize internervous planes to minimize denervation and devascularization of the musculature. For example, the anterior approach to the humerus (Henry approach) exploits the internervous plane between the brachialis (musculocutaneous and radial nerves) and the biceps brachii (musculocutaneous nerve) proximally, and the brachialis and brachioradialis (radial nerve) distally. Meticulous handling of the periosteum is critical. Only the periosteum necessary for fracture reduction and implant placement should be elevated, preserving the vital blood supply to the cortical bone.
Techniques for Absolute Stability
Absolute stability is mandatory for intra-articular fractures to prevent post-traumatic osteoarthritis and for simple diaphyseal fractures (e.g., transverse forearm fractures) where secondary healing via callus formation would tether adjacent structures and limit rotation.
The primary technique for achieving absolute stability is interfragmentary compression utilizing lag screws. A lag screw is not a specific type of screw, but rather a technique. A glide hole (equal to the outer diameter of the screw threads) is drilled in the near cortex, and a thread hole (equal to the core diameter of the screw) is drilled in the far cortex. As the screw is tightened, the head engages the near cortex, and the threads engage the far cortex, compressing the fracture fragments together.
Following interfragmentary compression, a neutralization plate is typically applied to protect the lag screw from torsional, bending, and shear forces. The plate is contoured to the anatomy of the bone and secured with bicortical screws. In transverse fractures, absolute stability can be achieved using a dynamic compression plate (DCP) or locking compression plate (LCP). By placing screws eccentrically in the specialized plate holes, the screw heads slide down the incline of the hole as they are tightened, translating the bone fragment and generating axial compression across the fracture site.
Techniques for Relative Stability
Relative stability is indicated for highly comminuted diaphyseal and metaphyseal fractures where attempting anatomic reduction of every fragment would cause catastrophic devascularization. The goal is to restore length, alignment, and rotation (LAR) while preserving the biology of the fracture hematoma to promote robust secondary callus formation.
Intramedullary Nailing (IMN) is the gold standard for diaphyseal fractures of the femur and tibia. The technique involves establishing a starting point (e.g., piriformis fossa or greater trochanter for the femur), passing a guide wire across the fracture site under fluoroscopic guidance, and sequentially reaming the medullary canal. Reaming generates autologous bone graft and increases the contact area between the nail and the endosteum. A statically locked intramedullary nail is then inserted, acting as an internal splint that resists bending and torsional forces while allowing micro-motion at the fracture site to stimulate callus formation.
Minimally Invasive Plate Osteosynthesis (MIPO) is another technique for relative stability, frequently used in metaphyseal fractures. A bridge plate is slid submuscularly across the fracture zone and secured to the proximal and distal main fragments. The comminuted fracture zone is left undisturbed, preserving the periosteal blood supply and fracture hematoma.
Complications and Management
Orthopedic trauma surgery carries inherent risks. Anticipation, early recognition, and aggressive management of complications are critical to preserving limb function and preventing catastrophic outcomes.
Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Pathophysiology and Clinical Presentation | Salvage Strategy and Management |
|---|---|---|---|
| Nonunion | 5 to 10 percent | Failure of the fracture to heal within the expected timeframe. Hypertrophic (adequate biology, inadequate stability) vs. Atrophic (inadequate biology). | Hypertrophic requires revision fixation for increased stability. Atrophic requires debridement, bone grafting (autograft or orthobiologics), and revision fixation. |
| Malunion | Varies by fracture | Healing of the bone in an unacceptable anatomical position (angular, rotational, or length discrepancy). | Corrective osteotomy, realignment, and rigid internal fixation. May require structural bone grafting. |
| Deep Infection | 1 to 5 percent (higher in open fractures) | Bacterial colonization of the fracture site and hardware, leading to osteomyelitis. Presents with pain, erythema, drainage, and elevated inflammatory markers. | Aggressive surgical debridement, hardware removal (if fracture is healed or hardware is loose), placement of antibiotic spacers, and prolonged culture-directed intravenous antibiotics. |
| Hardware Failure | 2 to 5 percent | Implant breakage or screw pullout secondary to nonunion (fatigue failure) or poor bone quality (osteoporosis). | Revision osteosynthesis utilizing longer plates, locking technology, intramedullary devices, or bone cement augmentation. |
| Compartment Syndrome | 1 to 9 percent (highest in tibial shaft fractures) | Increased pressure within a closed fascial space compromising tissue perfusion. Presents with pain out of proportion, pain with passive stretch, and tense compartments. | Emergent surgical fasciotomy of all involved compartments. Delayed primary closure or split-thickness skin grafting once swelling resolves. |
Management of Post Traumatic Osteoarthritis
Intra-articular fractures, even when anatomically reduced, carry a significant risk of post-traumatic osteoarthritis due to the initial chondrocyte apoptosis caused by the impact energy. Management begins with conservative measures including non-steroidal anti-inflammatory drugs, physical therapy, and intra-articular corticosteroid or hyaluronic acid injections. When conservative measures fail and the patient experiences debilitating pain and functional limitation, surgical salvage procedures such as joint arthrodesis (fusion) or total joint arthroplasty are indicated.
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is as critical as the surgical intervention itself. Protocols must be tailored to the specific fracture pattern, the stability of the surgical construct, and the patient's physiological capacity. The overarching goals are to prevent stiffness, restore muscle strength, and safely return the patient to their pre-injury level of function.
Weight Bearing Status
Weight-bearing restrictions are dictated by the mechanism of fixation.
* Non-Weight Bearing (NWB): Typically required for articular fractures treated with absolute stability (e.g., tibial plateau fractures) to prevent hardware subsidence and loss of reduction before early bone healing occurs.
* Toe-Touch Weight Bearing (TTWB): Allows the patient to rest the foot on the ground for balance only (approximately 10 to 15 pounds of force).
* Weight Bearing As Tolerated (WBAT): Generally permitted immediately for diaphyseal fractures treated with statically locked intramedullary nails, as the implant acts as a load-sharing device. Early weight-bearing stimulates secondary bone healing via micromotion.
Phases of Rehabilitation
- Phase One (Immediate Postoperative): Focuses on edema control, pain management, and early passive and active-assisted range of motion (ROM) of adjacent joints to prevent capsular contracture. Deep Vein Thrombosis (DVT) prophylaxis (chemical and mechanical) is initiated.
- Phase Two (Early Healing, 2 to 6 weeks): Once early radiographic callus is visible or soft tissues have healed, progression to active ROM and isometric strengthening begins. Proprioceptive training is initiated for lower extremity injuries.
- Phase Three (Advanced Healing, 6 to 12 weeks): Progressive resistance training and functional closed-kinetic-chain exercises are introduced. Weight-bearing status is advanced based on radiographic evidence of bridging bone.
- Phase Four (Return to Function, 3 to 6 months): Focuses on sports-specific or work-specific functional conditioning, plyometrics, and maximizing muscular endurance and power.
Summary of Key Literature and Guidelines
The modern practice of orthopedic traumatology is heavily evidence-based, relying on landmark studies and established clinical guidelines.
The foundational principles of fracture fixation were established by the AO Foundation. Perren's Strain Theory remains the definitive biomechanical model explaining the relationship between mechanical stability and the biological pathway of bone healing (primary versus secondary).
For open fractures, the Gustilo-Anderson classification, originally published in 1976 and modified in 1984, remains the standard for categorizing soft tissue injury and guiding antibiotic administration. Current guidelines dictate that intravenous antibiotics (typically a first-generation cephalosporin, with the addition of an aminoglycoside for high-grade injuries) should be administered as soon as possible, ideally within one hour of injury.
The Lower Extremity Assessment Project (LEAP) study revolutionized the approach to severe lower extremity trauma. This multicenter prospective study demonstrated that in severe, limb-threatening injuries, there is no significant difference in long-term functional outcomes between successful limb salvage and early amputation, highlighting the importance of shared decision-making and managing patient expectations.
Clinical practice guidelines, such as those published by the American Academy of Orthopaedic Surgeons (AAOS) and the British Orthopaedic Association Standards for Trauma (BOAST), provide evidence-based recommendations for the management of specific injuries, including the timing of surgery for hip fractures (ideally within 48 hours to reduce mortality) and the indications for operative intervention in clavicle fractures. Adherence to these guidelines ensures standardized, high-quality care and optimizes surgical outcomes in the management of osseous disruptions.
Clinical & Radiographic Imaging
You Might Also Like

