Operative Management of Patellar and Femoral Malunions: A Comprehensive Surgical Guide

Key Takeaway
Malunited fractures of the patella and distal femur present complex reconstructive challenges, often resulting in severe articular incongruity, altered biomechanics, and progressive post-traumatic arthropathy. Successful management requires meticulous preoperative planning, precise osteotomy execution, and rigid internal fixation. This guide details the surgical approaches, reduction techniques, and postoperative protocols essential for restoring lower extremity alignment and joint kinematics in complex patellofemoral and femoral shaft malunions.
INTRODUCTION TO EXTENSOR MECHANISM AND FEMORAL MALUNIONS
The management of malunited fractures of the patella and femur represents a formidable challenge in reconstructive orthopaedic surgery. Malunions in these critical weight-bearing and force-transmitting structures lead to profound biomechanical derangements, accelerated articular cartilage degradation, and significant functional disability. The primary objectives of surgical intervention are the restoration of the mechanical axis, the recreation of joint congruity, and the re-establishment of normal soft-tissue tension. This comprehensive guide delineates the evidence-based surgical strategies for addressing malunions of the patella, femoral condyles, and femoral diaphysis.
MANAGEMENT OF PATELLAR MALUNIONS
Pathophysiology and Biomechanics
The patella functions as a critical fulcrum, increasing the mechanical advantage of the quadriceps muscle by displacing the extensor mechanism anteriorly from the center of rotation of the knee. A malunited fracture of the patella disrupts this delicate biomechanical balance. The clinical presentation of a patellar malunion is virtually indistinguishable from advanced chondromalacia patellae or severe patellofemoral osteoarthritis.
Disability is directly proportionate to two factors:
1. The degree of step-off or irregularity of the articular surface of the patella.
2. The resultant roughening and eburnation of the contiguous articular surface of the femoral trochlea.
Altered patellofemoral tracking leads to focal areas of exponentially increased contact stress, rapidly degrading the articular cartilage.
Surgical Indications and Decision Making
In cases of intra-articular malunion with significant step-off (>2 mm) that present late, the articular cartilage is often irreversibly damaged. While intra-articular osteotomy and realignment may be considered in highly selected, very recent malunions in young patients, the procedure of choice for established, symptomatic patellar malunion is typically patellectomy (either partial or total, depending on the extent of the malunion and cartilage loss).
Clinical Pearl: When performing a patellectomy for malunion, meticulous repair of the extensor retinaculum and centralization of the quadriceps tendon are paramount to prevent postoperative extensor lag and patellar tracking instability.
MANAGEMENT OF DISTAL FEMORAL CONDYLE MALUNIONS
Biomechanics of Condylar Malunion
Malunion of one or both femoral condyles severely distorts the articular surface of the knee joint. Biomechanically, a femoral condyle malunion frequently produces a much more severe and rapid functional disability than a corresponding tibial plateau malunion due to the complex, multi-axial rolling and gliding kinematics of the distal femur.
Deformity patterns are highly predictable based on the affected condyle:
* Lateral Femoral Condyle Malunion: Typically results in a combined deformity of external rotation, flexion, and valgus angulation of the knee.
* Medial Femoral Condyle Malunion: Typically results in a combined deformity of internal rotation, flexion, and varus angulation of the knee.
Preoperative Evaluation and Templating
Detailed preoperative planning is mandatory. Evaluation must include long-leg, weight-bearing alignment radiographs to calculate the mechanical axis deviation (MAD) and the mechanical lateral distal femoral angle (mLDFA). Advanced imaging, including fine-cut Computed Tomography (CT) with 3D reconstructions, is essential to map the exact plane of the malunion and assess the bone stock available for internal fixation.
Surgical Technique: Lateral Femoral Condyle Malunion
Patient Positioning and Approach
- Place the patient supine on a radiolucent operating table. A sterile tourniquet may be applied to the proximal thigh.
- Incision: Approach the joint through a direct lateral incision. Begin the incision approximately 10 cm proximal to the knee joint line and extend it distally to a point 2.5 cm distal and slightly anterior to the head of the fibula (Gerdy's tubercle).
- Superficial Dissection: Incise the iliotibial (IT) band in line with its fibers.
- Nerve Protection: Meticulously identify and protect the common peroneal nerve as it courses posterior to the biceps femoris tendon and wraps around the fibular neck.
- Deep Dissection: Incise the vastus lateralis muscle fascia and elevate the muscle belly, retracting it anteriorly to expose the lateral femoral metaphysis and the site of the old fracture.
- Arthrotomy: Open the joint capsule and synovial membrane laterally. Direct visualization of the intra-articular step-off is critical during the reduction phase.
Osteotomy and Reduction
- Identify the plane of the malunion. Using a combination of an oscillating saw and sharp osteotomes, divide the bone as near to the original fracture plane as possible.
- Mobilization: Free the malunited fragment. In chronic cases, extensive soft tissue release (including the lateral collateral ligament origin if contracted) may be required to mobilize the fragment.
- Reduction: Grasp the mobilized lateral condyle with a large pointed bone-reduction forceps (Weber clamp). Manipulate the fragment into its anatomic position, ensuring absolute articular congruity under direct vision.
- Provisional Fixation: Drive two heavy Kirschner wires (K-wires) through the lateral fragment into the intact medial condyle. The wires should cross each other at an angle of approximately 30 degrees for maximum rotational stability and must protrude through the opposite (medial) cortex to ensure adequate purchase.
- Radiographic Verification: Obtain precise two-plane (AP and Lateral) fluoroscopic images to verify articular reduction, overall limb alignment, and K-wire trajectory.
Definitive Fixation
- Once reduction is confirmed, fix the fragment definitively using large fragment (6.5 mm or 7.3 mm) AO partially threaded cancellous screws with washers.
- If the fragment is large or if there is metaphyseal comminution/bone loss, augment the screw fixation with a lateral buttress plate (e.g., a pre-contoured distal femoral locking plate) to prevent shear displacement during rehabilitation.
Surgical Warning: When addressing a malunited fracture of the posterior aspect of the lateral condyle (Hoffa-type malunion), use the same lateral incision but carry the deep dissection further posteriorly. Retract the biceps tendon and peroneal nerve laterally and posteriorly. The posterior fragment is almost universally displaced proximally due to the pull of the gastrocnemius. It must be refractured from proximal to distal, reduced with a towel clip, and fixed with anterior-to-posterior (or posterior-to-anterior if using a specialized approach) lag screws.
Surgical Technique: Medial Femoral Condyle Malunion
The principles of correcting a medial femoral condyle malunion mirror those of the lateral side.
1. Utilize a standard medial or subvastus approach.
2. Perform the osteotomy along the malunion plane, reduce the articular surface, and stabilize with provisional K-wires followed by definitive AO cancellous lag screws and/or a medial buttress plate.
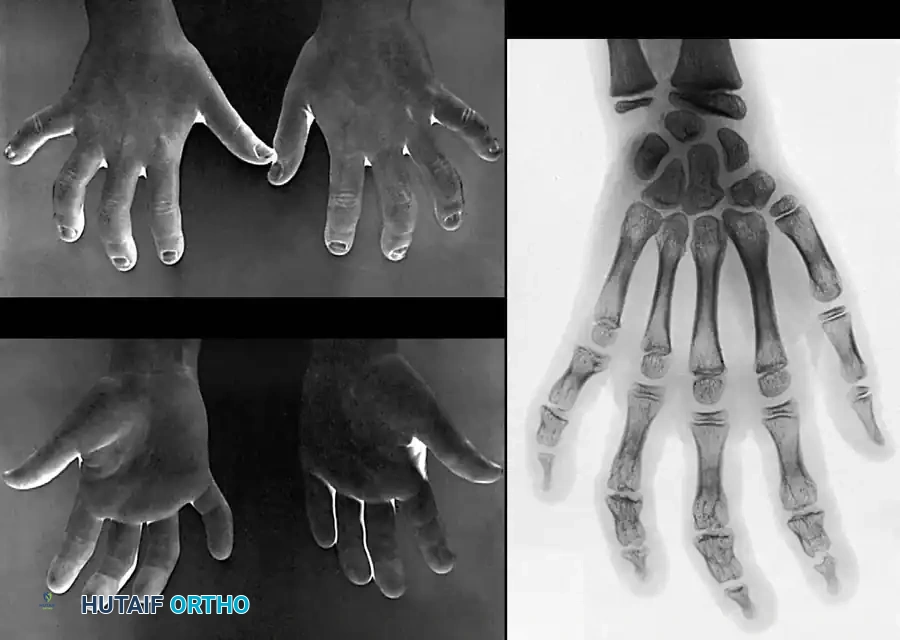
3. Pediatric Consideration: If the distal femoral physis is involved in a pediatric patient, the surgeon must anticipate and monitor for future growth disturbances (physeal arrest), which may necessitate subsequent epiphysiodesis or lengthening procedures.
Management of Bocondylar Malunions
Malunion of both femoral condyles with marked displacement presents a salvage situation.
Attempting open reduction and internal fixation of each individual condyle (as described above) is rarely indicated unless the malunion is of very short duration (less than 6-8 weeks) and occurs in a young, highly compliant patient with excellent bone stock.
For established bicondylar malunions:
* Extra-articular Deformity: If the primary issue is a varus or valgus mechanical axis deviation with a relatively congruent joint line, the extremity should be realigned via a corrective closing or opening wedge osteotomy through the distal femoral metaphysis.
* Intra-articular Destruction: When the contour of the joint is severely irregular, leading to intractable pain and profound functional impairment, joint salvage is often impossible. In these scenarios, Total Knee Arthroplasty (TKA) (often requiring constrained or hinged prostheses and structural bone grafting) or Knee Arthrodesis are the definitive procedures of choice.
MANAGEMENT OF FEMORAL SHAFT MALUNIONS
Preoperative Evaluation and Deformity Analysis
Femoral diaphyseal malunions require exhaustive preoperative planning. The surgeon must assess:
1. The extent of angular deformity (varus/valgus, procurvement/recurvatum).
2. Rotational malalignment (assessed clinically and via CT version studies).
3. Limb length discrepancy (shortening).
4. The degree of bony consolidation and the presence of any latent infection (aseptic vs. septic malunion).
5. The condition of the surrounding soft tissues and neurovascular structures.
Femoral osteotomies in adults—particularly those involving acute lengthening—carry significant risks, including deep infection, sciatic or femoral nerve palsies, hardware failure, and nonunion.
Surgical Strategies by Anatomic Zone
Diaphyseal Malunions (Lesser Trochanter to 5 cm Proximal to Intercondylar Notch)
For adults with aseptic malunions and healthy soft tissue envelopes, the gold standard treatment is corrective osteotomy, rigid fixation with an interlocking intramedullary (IM) nail, and autogenous iliac crest bone grafting.
- Osteotomy Execution: The femur can be divided directly through the plane of the malunion using a reciprocating or oscillating saw. Alternatively, to preserve bone stock and minimize thermal necrosis, the plane of the malunion can be outlined with multiple drill holes placed close together, and the division completed with a sharp osteotome.
- Fixation: Reamed, statically locked intramedullary nailing provides load-sharing biomechanics, allowing for early mobilization and weight-bearing. This technique requires a fracture table, high-quality image intensification, and advanced intramedullary instrumentation.
- Bone Grafting: Because the osteotomy site acts as an acute fracture with compromised local biology, autogenous cancellous bone grafting is highly recommended to ensure union.
Alternative Techniques: For patients with narrow medullary canals, active infection, or severe soft tissue compromise, alternative options include Open Reduction and Internal Fixation (ORIF) with broad dynamic compression plates (DCP) and screws, or external fixation utilizing the Ilizarov method for gradual deformity correction and lengthening.
Pediatric Considerations
In children, where nonoperative treatment (spica casting) of femoral fractures remains common, remodeling potential is high. However, for unacceptable malunions, osteotomy combined with skeletal traction and subsequent spica casting often yields excellent results without the need for rigid internal hardware.
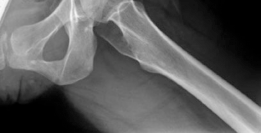
Proximal Third and Subtrochanteric Malunions
Malunions in the high-stress subtrochanteric region require robust fixation due to the massive deforming forces of the iliopsoas, abductors, and adductors.
* Fixation Options: A cephalomedullary interlocking nail (reconstruction nail) is the implant of choice, providing excellent biomechanical control of the proximal fragment. Alternatively, a standard interlocking nail or a fixed-angle compression hip screw device can be utilized depending on the exact level of the deformity.
Distal Third Malunions
Distal metaphyseal-diaphyseal malunions can be stabilized using:
* Retrograde intramedullary nails.
* Dynamic condylar compression plates (DCS).
* 95-degree angled blade plates.
* Modern pre-contoured distal femoral locking plates.
Specialized Osteotomy Techniques
The choice of osteotomy depends entirely on the geometry of the deformity:
* Opening Wedge Osteotomy: Used for angular correction; lengthens the limb but creates a structural void requiring robust bone grafting.
* Closing Wedge Osteotomy: Used for angular correction; provides excellent bony apposition but shortens the limb.
* Transverse Osteotomy: Ideal for correcting pure rotational deformities.
* Z-Step Osteotomy: A highly specialized technique used for one-stage femoral lengthening and realignment. The Z-cut allows for sliding lengthening while maintaining cortical contact. It is typically stabilized with an intramedullary nail, and the resulting step-defects are meticulously packed with corticocancellous bone graft.
Management of Overlapping Malunions
Malunions characterized by angulation, rotation, and end-to-end apposition (often resulting from premature weight-bearing before solid union) present a unique challenge.
* Early Intervention: If the malunion is of very short duration (e.g., early callus phase following nonoperative treatment), it can sometimes be broken up manually under anesthesia. The overlapping and angulation are then corrected via skeletal traction or graduated distraction with an external fixator.
* Neurologic Warning: During acute or gradual distraction, the surgeon must maintain extreme vigilance to prevent traction neuropraxia of the sciatic nerve or its peroneal division.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol must be tailored to the stability of the fixation and the quality of the patient's bone.
Phase I: Immediate Postoperative (Weeks 0-2)
- For condylar osteotomies fixed with screws/plates, the limb may be placed in a hinged knee brace locked in extension to protect the soft tissues and fixation.
- Strict elevation and cryotherapy are employed to manage edema.
- Weight-bearing is strictly restricted (Non-Weight Bearing - NWB).
Phase II: Early Mobilization (Weeks 2-8)
- At 2 weeks, surgical wounds are inspected, and sutures are removed.
- A functional cast brace or hinged orthosis is applied.
- Active and active-assisted Range of Motion (ROM) exercises are initiated. If fixation is deemed exceptionally rigid intraoperatively, continuous passive motion (CPM) and overhead pulley exercises can be utilized.
- An elevated shoe lift may be fitted to the contralateral limb to facilitate crutch clearance.
- Weight-bearing remains restricted to toe-touch or NWB until radiographic evidence of bridging callus is observed.
Phase III: Consolidation and Strengthening (Weeks 8-12+)
- Clinical and radiographic union is typically assessed at 8 to 12 weeks.
- Once union is confirmed, progressive weight-bearing is initiated.
- Free motion of the knee is permitted, and aggressive physical therapy focuses on quadriceps strengthening, hamstring flexibility, and proprioceptive retraining.
- The surgeon must monitor the patient closely during this phase, as partial loss of reduction can occur if the bone graft has not fully incorporated or if the patient is non-compliant with weight-bearing restrictions.
You Might Also Like