Masterclass in Traumatic Hip Dislocations and Associated Lower Extremity Injuries

Key Takeaway
Traumatic hip dislocations are orthopaedic emergencies requiring immediate reduction to mitigate the risk of femoral head osteonecrosis. Typically resulting from high-energy trauma, these injuries demand meticulous clinical evaluation, advanced radiographic profiling, and precise execution of closed or open reduction techniques. This guide details the biomechanics, classification systems, step-by-step reduction maneuvers, and management of associated lower extremity injuries, including proximal tibiofibular joint dislocations.
Introduction to Traumatic Hip Dislocations
The hip joint is an inherently stable, highly constrained ball-and-socket (diarthrodial) joint. Its stability is derived from its deep bony architecture—with the acetabulum providing extensive coverage of the femoral head—augmented by the fibrocartilaginous labrum and a robust capsuloligamentous complex. The iliofemoral ligament (Y ligament of Bigelow) is the strongest ligament in the human body, providing critical anterior restraint. Because of this profound intrinsic stability, hip dislocations generally are produced only by high-energy trauma and are frequently associated with multiple injuries to different organ systems.
Motor vehicle accidents (MVAs) remain the most common mechanism of hip dislocation, often referred to as the classic "dashboard injury." This is followed by falls from a significant height, high-impact industrial accidents, and, more rarely, high-velocity contact sports such as football, rugby, or wrestling.
Clinical Pearl: Always approach a traumatic hip dislocation as a polytrauma scenario. The energy required to dislocate a native hip is immense; therefore, the physician must maintain a high index of suspicion for concomitant life-threatening injuries, adhering strictly to Advanced Trauma Life Support (ATLS) protocols before focusing solely on the orthopaedic injury.
Biomechanics and Mechanisms of Injury
The direction of the dislocation is dictated by the position of the lower extremity at the exact moment of impact, combined with the vector of the applied force.
Posterior Dislocations
Posterior dislocations occur much more frequently than anterior dislocations (accounting for approximately 85% to 90% of all hip dislocations). They typically result from a posteriorly directed force applied to the anterior aspect of a flexed knee, with the hip also in a flexed position.
* Simple Posterior Dislocation: Occurs when the hip is in a state of adduction and internal rotation during axial loading. The femoral head is driven posteriorly over the rim of the acetabulum without causing a major fracture.
* Fracture-Dislocation: Lesser degrees of hip flexion and increasing amounts of hip abduction with a similarly applied force often result in the femoral head striking the posterior wall of the acetabulum, leading to an associated posterior wall or column fracture.
Anterior Dislocations
Anterior dislocations are less common (10% to 15%) and are caused by a forceful abduction and external rotation applied to the affected limb. The femoral head is levered out of the acetabulum anteriorly, tearing the anterior capsule. Depending on the degree of hip flexion at the time of injury, the head may migrate superiorly (pubic) or inferiorly (obturator).
Clinical Presentation and Initial Evaluation
The clinical posture of the patient is often pathognomonic for the direction of the dislocation.
- Posterior Dislocation: Patients with an isolated posterior hip dislocation present with the affected limb in a position of hip flexion, adduction, internal rotation, and apparent shortening.
- Anterior Dislocation: Anterior dislocations cause the leg to be held in a position of abduction and external rotation. If it is a superior (pubic) dislocation, the hip is extended; if it is an inferior (obturator) dislocation, the hip is flexed.
Although isolated hip dislocations are easily recognized by these classic deformities, associated lower extremity injuries (such as ipsilateral femoral shaft fractures) may distract the examining physician or alter the classic resting position of the dislocated hip.
Surgical Warning: Careful physical examination is crucial, with particular attention paid to the sciatic nerve. Sciatic nerve neurapraxia or axonotmesis occurs in 10% to 20% of posterior dislocations. The peroneal division is most susceptible due to its lateral position and tethering at the sciatic notch and fibular head. Document detailed motor and sensory function of the deep and superficial peroneal nerves prior to any reduction attempt.
Radiographic Assessment and Advanced Imaging
Standardized radiographic profiling is mandatory for diagnosis, classification, and preoperative planning.
- Anteroposterior (AP) Pelvis: The initial screening view. It confirms the direction of the dislocation and identifies gross fractures of the acetabulum or femoral head.
- Judet Views (45-degree Oblique): The obturator oblique and iliac oblique views are essential for evaluating the anterior and posterior columns and walls of the acetabulum.
- Post-Reduction Computed Tomography (CT): A CT scan of the pelvis with 3-mm cuts (or finer) and bone windows is strictly recommended after reduction. The CT scan is the gold standard to rule out associated femoral head fractures, acetabular fractures, incarcerated intraarticular osteochondral fragments, and to assess joint congruency.
Classification Systems for Hip Dislocations
Hip dislocations are classified according to the position of the femoral head in relation to the acetabulum and the presence of associated fractures.
Posterior Dislocations: Thompson and Epstein Classification
Thompson and Epstein classified posterior dislocations into five distinct types based on associated bony injuries:
* Type I: Simple dislocation with or without a minor (insignificant) posterior wall fracture.
* Type II: Dislocation with a large, single fracture of the posterior acetabular rim.
* Type III: Dislocation with a comminuted fracture of the rim of the acetabulum, with or without a major fragment.
* Type IV: Dislocation with fracture of the acetabular rim and floor.
* Type V: Dislocation with an associated fracture of the femoral head (often cross-referenced with the Pipkin classification).
Anterior Dislocations: Epstein Classification
Anterior dislocations have been classified by Epstein based on the anatomical resting place of the femoral head:
1. Pubic (Superior):
* With no fracture (simple)
* With fracture of the head of the femur
* With fracture of the acetabulum
2. Obturator (Inferior):
* With no fracture (simple)
* With fracture of the head of the femur
* With fracture of the acetabulum
FIGURE 60-10: Bilateral obturator dislocations of the hip. Note the extreme abduction and external rotation characteristic of this inferior anterior dislocation pattern.
(Note: The historical term "central dislocation" referred to a medial position of the femoral head after a fracture involving the medial wall of the acetabulum. This term is largely obsolete and is more accurately described as an acetabular fracture with medial displacement.)
Principles of Management: The Orthopaedic Emergency
A hip dislocation constitutes an absolute orthopaedic emergency. Delaying reduction exponentially increases the risk of osteonecrosis (avascular necrosis) of the femoral head due to prolonged kinking, stretching, or tearing of the medial circumflex femoral artery and its retinacular branches.
Evidence-Based Standard: Hougaard and Thomsen established the critical 6-hour window. They reported an osteonecrosis rate of 4.8% if reduction occurred within 6 hours of injury, compared with a catastrophic 53% if reduction was delayed for more than 6 hours.
Once the initial trauma survey is complete and life-threatening injuries are stabilized, the dislocated hip takes precedence over almost any other orthopaedic injury. Closed reduction should be attempted initially in the emergency department under deep intravenous sedation or general anesthesia. If other injuries require emergency operative intervention (e.g., exploratory laparotomy), the initial hip reduction can be performed simultaneously in the operating room.
Closed Reduction Techniques
The following guidelines refer to simple hip dislocations without significant associated fractures (Thompson and Epstein Type I). All closed reduction methods generally rely on re-creating the injurious deforming force to unlock the femoral head, followed by traction and corrective rotation.
- The Allis Maneuver: The most commonly utilized technique for posterior dislocations. The patient is placed supine. An assistant stabilizes the pelvis by applying downward pressure on the anterior superior iliac spines. The surgeon flexes the patient's knee and hip to 90 degrees. In-line traction is applied vertically. While maintaining traction, the surgeon applies gentle adduction and internal rotation to clear the posterior acetabular lip, followed by external rotation and extension to guide the head into the socket.
- The Stimson Maneuver: The patient is placed prone with the affected leg hanging off the side of the stretcher, flexing the hip and knee to 90 degrees. Gravity assists the reduction. The surgeon applies downward pressure on the proximal calf just distal to the popliteal fossa, combined with gentle rotation.
- Fulcrum Techniques: Other techniques involve levering the affected limb over a fulcrum (such as the surgeon's forearm placed under the patient's knee) while applying downward force at the ankle.
Crucial Pitfall: Regardless of the method chosen, only two or three attempts should be made at closed reduction. Multiple, increasingly forcible attempts can lead to iatrogenic femoral head, neck, or shaft fractures, or severe cartilaginous shear injury to the joint surfaces.
Indications for Open Reduction
Failed closed reduction is a clear indication for immediate open reduction. Impediments to closed reduction include:
* "Buttonholing" of the femoral head through the capsule.
* Inversion of the acetabular labrum into the joint space.
* Interposition of the piriformis muscle or capsule into the acetabulum.
* Incarcerated osteochondral bone fragments.
If closed reduction fails, or if the post-reduction CT shows an incongruent joint (widened joint space >2mm compared to the contralateral side), skeletal traction with the femoral head slightly distracted should be applied to avoid further cartilaginous injury until surgery can be performed.
Surgical Approaches for Open Reduction
The surgical approach is dictated by the direction of the dislocation and the location of any associated fractures.
Posterior Approach (Kocher-Langenbeck)
Used for irreducible posterior dislocations or those with posterior wall/column fractures.
* Positioning: Lateral decubitus.
* Technique: The incision is centered over the greater trochanter, curving posteriorly toward the PSIS. The gluteus maximus is split in line with its fibers. The sciatic nerve is identified and protected. The short external rotators (piriformis, obturator internus, gemelli) are tagged and tenotomized near their femoral insertion to expose the posterior capsule. A capsulotomy is performed to extract incarcerated fragments and reduce the joint.
Anterior and Lateral Approaches
Anterior dislocations can be reduced via the direct anterior approach (Smith-Petersen) or the anterolateral/direct lateral approaches (Watson-Jones, Hardinge).
* Smith-Petersen: Utilizes the internervous plane between the sartorius (femoral nerve) and tensor fasciae latae (superior gluteal nerve). It offers an excellent view of the anterior femoral head and is ideal for extracting anterior intraarticular fragments or addressing Pipkin fractures.
* Watson-Jones/Hardinge: These approaches offer better access to the superior and lateral aspects of the joint and can be extended to access the posterior capsule if necessary.
Complications of Hip Dislocations
- Osteonecrosis (Avascular Necrosis): Occurs in 4% to 22% of simple hip dislocations. Time to reduction is the most critical modifiable risk factor. Most patients who develop osteonecrosis present with symptoms within 2 years of injury, though late radiographic changes delayed up to 5 years have been reported.
- Post-Traumatic Osteoarthritis: Can occur due to the initial cartilaginous impact (chondral shear) or secondary to osteonecrosis or subtle joint incongruity.
- Sciatic Nerve Injury: Present in up to 20% of posterior dislocations. Most are neurapraxias that recover with time, but foot drop splinting and rigorous physical therapy are required during the recovery phase.
Associated Lower Extremity Injuries: The Proximal Tibiofibular Joint
High-energy trauma causing hip dislocations frequently results in concomitant injuries along the kinetic chain of the lower extremity. One often-overlooked injury in the polytraumatized patient is the dislocation of the proximal tibiofibular joint (PTFJ).
Anatomy and Ogden Classification of the PTFJ
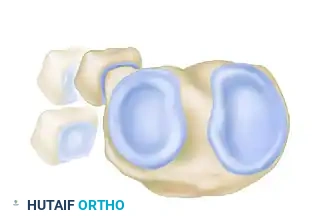
The PTFJ is a synovial joint between the lateral condyle of the tibia and the head of the fibula. Ogden classified the anatomical variants of this joint into two basic types based on the inclination of the articular surface:


FIGURE 60-7: Two basic types of proximal tibiofibular joints according to Ogden. The horizontal type is generally more stable, whereas the oblique type is more prone to rotational displacement and dislocation.
Acute Dislocation of the Proximal Tibiofibular Joint
Dislocations of the PTFJ usually occur with the knee flexed and the ankle inverted and plantarflexed. This tension on the lateral collateral ligament and biceps femoris tendon can avulse or displace the fibular head.




FIGURE 60-6: A and B, Acute dislocation of the proximal tibiofibular joint. C and D, After closed reduction. Note the distinct change in the position of the fibular head relative to the lateral tibial plateau in both orthogonal views.
Ogden Classification of PTFJ Disruptions
Ogden further classified disruptions of the proximal tibiofibular joint into four distinct directional categories:






You Might Also Like


