Biomechanical Construct Complications in Orthopaedic Trauma
Key Takeaway
Biomechanical construct complications occur when the fatigue life of an orthopaedic implant is exceeded prior to achieving solid bony union. All internal and external fixation systems will eventually fail under cyclic loading if osteogenesis is delayed. Successful management requires early recognition of hardware failure, comprehensive biological optimization, and meticulous surgical revision utilizing techniques such as exchange nailing, plate augmentation, and autologous bone grafting to restore mechanical stability and stimulate fracture healing.
BIOMECHANICAL CONSTRUCT COMPLICATIONS: PATHOPHYSIOLOGY AND PRINCIPLES
The fundamental tenet of osteosynthesis is that fracture fixation represents a physiological and mechanical race between bone healing and implant failure. All implants and external fixation systems eventually fail if bone regeneration does not occur in a timely fashion. Orthopaedic hardware is designed to provide temporary mechanical stability, offloading physiological stresses from the fracture site until the biological envelope can bridge the defect with a mature, mineralized callus. When a nonunion or delayed union occurs, the implant is subjected to prolonged, repetitive cyclic loading that inevitably exceeds its fatigue life, culminating in catastrophic biomechanical construct complications.
Understanding the interplay between mechanical stability and biological vitality is paramount for the orthopaedic surgeon. Construct failure is rarely an isolated mechanical event; it is almost universally the clinical manifestation of an underlying biological failure (nonunion, infection, or avascularity). Therefore, the management of broken plates, fractured intramedullary nails, or failed external fixators must address both the mechanical instability and the compromised biological environment.
Clinical Pearl: Never revise a failed biomechanical construct without simultaneously addressing the biological cause of the nonunion. Simply replacing a broken implant with a larger one without optimizing the biological environment (e.g., bone grafting, decortication, infection eradication) will predictably lead to a second failure.
BIOMECHANICS OF IMPLANT FATIGUE AND FAILURE
Orthopaedic implants are subjected to complex multiaxial forces, including bending, torsion, shear, and axial compression. The failure of these constructs is governed by the principles of materials science and fatigue mechanics.
The S-N Curve and Endurance Limit
The fatigue life of an implant is graphically represented by the S-N (Stress-Number of cycles) curve. Every material (e.g., Titanium alloy, 316L Stainless Steel) has an endurance limit—a stress level below which the material can theoretically endure an infinite number of loading cycles without failing. However, in the presence of a nonunion, the physiological loads transmitted through the implant often exceed this endurance limit. Microcracks initiate at areas of high stress concentration and propagate with each step the patient takes, eventually leading to macroscopic failure.
Stress Risers and Notch Sensitivity
Construct complications frequently occur at stress risers. These are architectural features of the implant or iatrogenic alterations that concentrate mechanical forces. Common stress risers include:
* Empty screw holes in a plate over a fracture gap.
* The junction between the solid and slotted portions of an intramedullary nail.
* Scratches or gouges created by drill bits or reduction forceps during the index procedure.
* The thread-shaft junction of locking screws.
CLINICAL AND RADIOGRAPHIC EVALUATION
The diagnosis of a biomechanical construct complication requires a high index of suspicion, particularly in patients who present with new-onset pain after a period of postoperative comfort.
Clinical Presentation
Patients typically report a sudden "pop" or a gradual return of pain at the fracture site, often accompanied by swelling, deformity, or a subjective feeling of instability. A thorough history must evaluate risk factors for nonunion, including smoking (which severely compromises microvascular circulation), diabetes, NSAID use, and previous open fracture.
Radiographic Assessment
High-quality, orthogonal radiographs are mandatory. The surgeon must scrutinize the images for:
* Hardware Breakage: Obvious fracture of plates, nails, or screws.
* Hardware Loosening: Radiolucent halos around screws or pins, indicating micromotion and fibrous encapsulation.
* Implant Deformation: Bending of plates or nails, which precedes frank breakage.
* Fracture Status: Absence of bridging callus, hypertrophic nonunion (elephant foot), or atrophic nonunion (penciling of bone ends).
Surgical Warning: Always rule out subclinical infection in the setting of construct failure. Aseptic nonunion is a diagnosis of exclusion. Preoperative inflammatory markers (CRP, ESR) should be obtained, and intraoperative tissue cultures (minimum of 3-5 distinct samples) are mandatory during revision surgery.
SPECIFIC HARDWARE FAILURE PATTERNS
Intramedullary Nail Breakage
Intramedullary nails are load-sharing devices. When a diaphyseal fracture fails to heal, the nail is subjected to massive bending moments, particularly in the subtrochanteric region of the femur or the proximal third of the tibia. Nail breakage typically occurs directly at the level of the nonunion.
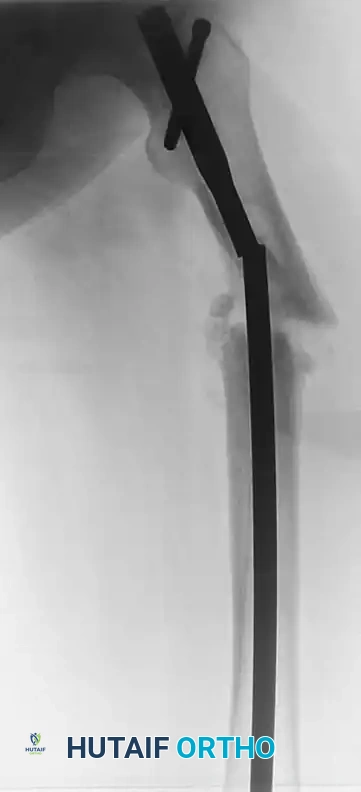
FIGURE 53-49 A: Broken femoral intramedullary nail resulted in nonunion that required bone grafting and plate fixation. The failure occurred at the zone of maximum bending stress, necessitating a comprehensive revision strategy.
If possible, it is best to augment the fracture prior to catastrophic failure if delayed union is identified early. However, once the nail breaks, extraction of the retained distal segment becomes a significant technical challenge.
Locking Screw Failure and "Auto-Dynamization"
Locking screws are subjected to high shear forces. In some instances, the failure of locking screws can paradoxically benefit the healing process. If the screws break, the nail may be allowed to slide axially, compressing the fracture site—a phenomenon known as "auto-dynamization."

FIGURE 53-49 B: Broken screws proximally and distally did not impede bony union. The shear failure of the screws allowed for axial compression, facilitating secondary bone healing.
While auto-dynamization can lead to union, it is an uncontrolled process that may also result in loss of length, malrotation, or angular deformity. Therefore, prophylactic, controlled dynamization (removing static locking screws) is preferred over waiting for implant failure.
SURGICAL REVISION STRATEGIES: STEP-BY-STEP APPROACH
The revision of a failed biomechanical construct is a complex procedure that demands meticulous preoperative planning, specialized equipment, and a deep understanding of both mechanical and biological augmentation.
Preoperative Optimization
- Host Optimization: Strict smoking cessation is mandatory. Nutritional deficiencies (Vitamin D, Calcium, Albumin) must be corrected.
- Equipment Availability: Ensure the availability of universal hardware extraction sets, broken screw removal kits, carbide drills, metal-cutting burrs, and specialized extraction hooks for retained intramedullary nails.
- Biological Planning: Plan for autologous bone grafting (e.g., Reamer-Irrigator-Aspirator [RIA] from the femur, or iliac crest bone graft) and consider osteoinductive adjuncts.
Step-by-Step Surgical Technique: Broken Nail Extraction and Revision
Step 1: Patient Positioning and Approach
Position the patient supine or lateral on a radiolucent table, depending on the bone involved. Ensure unimpeded fluoroscopic access in two orthogonal planes. Utilize the previous surgical incisions, extending them as necessary to achieve adequate exposure.
Step 2: Proximal Hardware Removal
Expose the proximal end of the nail. Remove any remaining proximal locking screws. Engage the proximal nail segment with the appropriate extraction device and remove it. This step is usually straightforward unless the internal threads of the nail are stripped or damaged by tissue ingrowth.
Step 3: Distal Segment Extraction
This is the most challenging aspect of the procedure. Several techniques can be employed:
* Extraction Hook Technique: Pass a specialized extraction hook past the broken distal segment, engage the distal tip of the nail, and back-slap it out.
* Ball-Tipped Guide Wire Technique: Pass a ball-tipped guide wire through the cannulation of the broken distal segment. Impact a small reamer or a specialized interference device over the wire to jam it within the nail, then extract the entire unit.
* Open Extraction: If closed methods fail, open the fracture site directly. Use a high-speed burr to create a small cortical window if necessary, grasp the distal segment with vice grips, and extract it.
Step 4: Canal Preparation and Biological Stimulation
Once the hardware is removed, the nonunion site must be addressed. Over-ream the medullary canal by 1.5 to 2.0 mm larger than the previous nail. This serves two purposes: it removes the fibrous membrane lining the canal and generates autologous bone graft (reamings) that can be deposited at the fracture site.
Step 5: Definitive Fixation and Augmentation
Insert a new, larger diameter intramedullary nail to provide enhanced mechanical stability. If rotational stability is a concern, or if the nonunion is atrophic, augment the construct with a compression plate.
* Plate Augmentation: Applying a plate over an intramedullary nail (plate-nail construct) dramatically increases torsional and bending stiffness.
* Bone Grafting: Pack the nonunion site with autologous bone graft. In cases of severe biological compromise, the use of recombinant human bone morphogenetic protein (rhBMP-2 or rhBMP-7) may be indicated to stimulate osteogenesis.
BIOLOGICAL AUGMENTATION IN REVISION OSTEOSYNTHESIS
The literature heavily supports the aggressive biological management of nonunions following construct failure. The "Diamond Concept" of fracture healing must be respected, ensuring the presence of:
1. Osteogenic Cells: Provided by autograft or bone marrow aspirate concentrate (BMAC).
2. Osteoconductive Scaffold: Provided by cancellous bone chips, demineralized bone matrix (DBM), or synthetic calcium phosphate ceramics.
3. Osteoinductive Growth Factors: Provided by local hematoma, autograft, or exogenous BMPs.
4. Mechanical Stability: Provided by the revised, robust fixation construct.
Management of Soft Tissue and Infection
In cases where construct failure is secondary to an underlying low-grade infection or poor soft tissue envelope (common in severe open fractures), the principles of damage control orthopaedics apply.
* Irrigation: Evidence suggests that low-pressure lavage is superior to high-pressure pulsatile lavage, as the latter can drive bacteria deeper into the soft tissues and damage the local microvasculature.
* Antibiotic Delivery: The use of local antibiotic-impregnated polymethylmethacrylate (PMMA) beads or cement spacers may be required as a staged procedure before definitive revision osteosynthesis can be safely performed.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative management following revision of a failed biomechanical construct must be carefully tailored to the stability of the new fixation and the biological quality of the bone.
- Phase 1 (0-6 Weeks): Focus on soft tissue healing and joint mobilization. Weight-bearing is typically restricted (toe-touch or partial weight-bearing) to protect the new construct while early callus forms. Chemical and mechanical DVT prophylaxis is mandatory.
- Phase 2 (6-12 Weeks): Clinical and radiographic evaluation at 6 weeks. If early bridging callus is visible and the patient is pain-free at the fracture site, weight-bearing can be progressively advanced.
- Phase 3 (3-6 Months): Full weight-bearing is permitted once solid radiographic union is achieved in at least three out of four cortices on orthogonal views. Long-term monitoring is required to ensure the biological envelope has fully consolidated and the new implant does not succumb to fatigue failure.
Surgical Pitfall: Premature weight-bearing in an atrophic nonunion revision, even with a robust plate-nail construct, risks early catastrophic failure of the revision hardware. The mechanical construct is only a bridge; the bone must ultimately bear the load.
You Might Also Like


