Correction of Cervicotrochanteric Malunion: Advanced Surgical Techniques and Outcomes
Key Takeaway
Cervicotrochanteric malunion presents a complex reconstructive challenge characterized by varus collapse, external rotation, and limb shortening. Successful surgical correction requires meticulous preoperative planning, precise osteotomy, and rigid internal fixation. This guide details the step-by-step surgical technique, from the lateral approach and fibrous tissue excision to deformity correction and pediatric considerations. Mastery of these principles is essential for restoring hip biomechanics and optimizing patient outcomes.
Introduction to Cervicotrochanteric Malunion
Cervicotrochanteric fractures, occurring at the junction of the femoral neck and the intertrochanteric line, are inherently unstable injuries. When managed nonoperatively or when internal fixation fails, these fractures frequently progress to a cervicotrochanteric malunion. This condition presents a formidable reconstructive challenge for the orthopaedic surgeon, characterized by a complex three-dimensional deformity: severe varus collapse, external rotation of the distal fragment, and significant limb shortening.
The profound alteration of proximal femoral anatomy severely compromises the abductor lever arm, leading to a debilitating Trendelenburg gait, chronic hip pain, and accelerated joint degeneration. Surgical correction is technically demanding and requires a deep understanding of hip biomechanics, meticulous preoperative templating, and precise execution of corrective osteotomies. This comprehensive guide details the evidence-based surgical management of cervicotrochanteric malunions, tailored for the postgraduate orthopaedic surgeon.
Pathoanatomy and Biomechanics
Understanding the pathoanatomy of a cervicotrochanteric malunion is critical for executing a successful surgical correction. The deformity is driven by the unopposed pull of the powerful musculature crossing the hip joint during the period of fracture healing.
Deforming Muscular Forces
- Proximal Fragment: The short external rotators and the iliopsoas muscle exert a strong force on the proximal fragment, pulling it into flexion, abduction, and external rotation.
- Distal Fragment: The adductor complex pulls the femoral shaft medially and proximally, resulting in varus collapse and limb shortening. Simultaneously, the weight of the limb and the pull of the gluteus maximus contribute to the external rotation of the distal fragment.
The Malunion Morphology
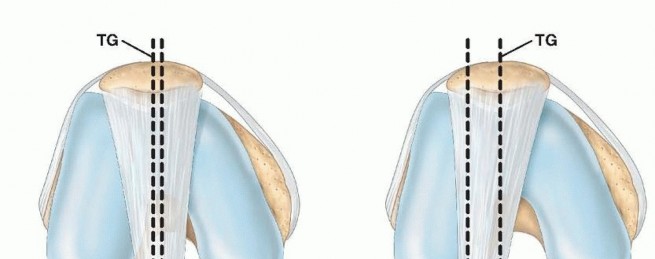
Because of the severe external rotation of the distal fragment relative to the proximal fragment, the fractured surface of the greater trochanter faces anteromedially rather than medially.
Clinical Pearl: A hallmark of cervicotrochanteric malunion is the presence of a wedge-shaped space between the fragments. The base of this wedge is located anteriorly and is typically filled with dense, unyielding fibrous tissue, while the osseous union occurs predominantly along the posterior cortex. Recognizing this specific morphology is the key to successful intraoperative reduction.
Preoperative Evaluation and Templating
A rigorous preoperative assessment is mandatory to quantify the deformity and plan the corrective osteotomy.
Clinical Assessment
Patients typically present with a pronounced limp, limb length discrepancy (LLD), and restricted range of motion, particularly in internal rotation and abduction. A thorough neurovascular examination is essential, as the planned correction will involve significant lengthening and rotation of the limb, placing tension on the sciatic and femoral nerves.
Radiographic Imaging and 3D Templating
- Standard Radiographs: Anteroposterior (AP) pelvis, cross-table lateral of the affected hip, and full-length standing leg films are required to assess the neck-shaft angle, offset, and overall limb alignment.
- Computed Tomography (CT): A fine-cut CT scan with 3D reconstructions is the gold standard for evaluating the rotational profile and the exact location of the posterior osseous bridge versus the anterior fibrous wedge.
- Digital Templating: The surgeon must calculate the exact wedge of bone or fibrous tissue to be resected and determine the optimal angle of the fixation device (e.g., a 130-degree or 135-degree compression hip screw) to restore the normal neck-shaft angle.
Surgical Anatomy and Approach
The preferred surgical approach for the correction of a cervicotrochanteric malunion is a curved lateral incision, utilizing the internervous plane between the tensor fasciae latae (TFL) and the gluteus medius. This is classically known as the Watson-Jones approach.
The Watson-Jones Interval
- Incision: A curved lateral incision is made, starting approximately 2.5 cm posterior to the anterior superior iliac spine (ASIS), curving distally and posteriorly over the greater trochanter, and extending along the proximal 5 cm of the femoral shaft.
- Superficial Dissection: The fascia lata is incised in line with the skin incision.
- Deep Dissection: The interval between the TFL (supplied by the superior gluteal nerve) and the gluteus medius (also supplied by the superior gluteal nerve) is identified. While this is technically not a true internervous plane, it provides excellent access to the anterior capsule and the cervicotrochanteric junction.
Surgical Warning: The superior gluteal nerve and vessels cross the operative field approximately 3 to 5 cm proximal to the tip of the greater trochanter. Dissection proximal to this zone must be strictly avoided to prevent denervation of the abductor musculature, which would catastrophically worsen the patient's postoperative gait.
Step-by-Step Surgical Technique
Patient Positioning
The patient is placed supine on a radiolucent fracture table. This positioning is critical as it allows for the application of marked longitudinal traction and facilitates unimpeded intraoperative fluoroscopy (image intensification) in both the AP and lateral planes. Alternatively, a flat radiolucent table with a femoral distractor can be utilized, though a fracture table is generally preferred for dynamic control of the limb.
Exposure and Debridement
- Exposing the Malunion: Retract the TFL anteriorly and the gluteus medius posteriorly to expose the anterior capsule of the hip, the trochanters, and the proximal femoral shaft.
- Capsulotomy: A T-shaped or H-shaped capsulotomy is performed to visualize the cervicotrochanteric junction and the base of the femoral neck.
- Excising the Fibrous Wedge: Identify the anterior wedge-shaped space. Using a combination of rongeurs, curettes, and electrocautery, meticulously excise the dense fibrous tissue filling this gap.
- Preparation of the Bone: The fibrous tissue must be excised completely down to healthy, bleeding normal bone. Failure to clear this space will mechanically block the subsequent reduction maneuvers.
Osteotomy and Deformity Correction
- Dividing the Osseous Union: Once the anterior fibrous wedge is cleared, the posterior osseous union is visualized. Using a sharp, broad osteotome or an oscillating saw, carefully divide the bony bridge posteriorly.
- Mobilization: Ensure the distal fragment is completely free from the proximal fragment.
- Reduction Maneuver: Appose the freshly prepared bone surfaces. Correct the deformity by applying marked longitudinal traction to the leg via the fracture table, followed by controlled abduction and internal rotation of the distal fragment.
Clinical Pearl: The reduction maneuver essentially reverses the mechanism of the initial deformity. The internal rotation closes the anterior gap (where the fibrous tissue was excised), while the abduction restores the neck-shaft angle and the abductor lever arm.
Soft Tissue Balancing: Adductor Tenotomy
In chronic malunions, the adductor musculature becomes severely contracted. If marked traction and manual abduction fail to restore the neck-shaft angle, the adductors are acting as a tether.
* Technique: Perform a percutaneous or open tenotomy of the adductor longus (and occasionally the adductor brevis) near their origin on the pubis. This release is often the critical step required to obtain sufficient abduction of the distal fragment without placing undue stress on the osteotomy site.
Internal Fixation Strategies
Once the normal angle between the shaft and the neck has been restored, the reduction must be provisionally held with heavy Kirschner wires and confirmed via image intensification in both AP and lateral planes.
- Implant Selection: Fix the fracture with a sliding compression hip screw (Dynamic Hip Screw - DHS) or a cephalomedullary nail, utilizing a technique similar to that described for acute trochanteric fractures.
- Guidewire Placement: Insert the guidewire centrally into the femoral head, ensuring a tip-apex distance (TAD) of less than 25 mm to minimize the risk of hardware cut-out.
- Compression: The sliding mechanism of the compression screw allows for dynamic compression across the osteotomy site, promoting primary bone healing.
Pediatric Considerations and Physis Preservation
Cervicotrochanteric malunions in the pediatric population require highly specialized considerations due to the presence of open growth plates and the unique biology of the developing hip.
Implant Selection in Children
For children, standard adult implants are contraindicated. A pediatric compression hip screw or a specialized pediatric locking proximal femoral plate is preferable. These implants are designed to accommodate the smaller dimensions of the pediatric femur and are much easier to insert into the dense, hard bone characteristic of the pediatric femoral neck and head.
Protecting the Capital Femoral Physis
Surgical Warning: The capital femoral physis must be meticulously avoided during guidewire and screw insertion if at all possible. Penetration of the physis with large-diameter threaded implants can lead to premature physeal closure, resulting in severe leg length discrepancy and secondary deformities of the femoral head.
If the child is nearing skeletal maturity, intentional epiphysiodesis may be acceptable, but in younger children, smooth pins or screws that stop short of the physis are mandatory.
Associated Intra-Articular Pathology
When evaluating a patient with a proximal femoral malunion, the surgeon must maintain a high index of suspicion for concurrent intra-articular pathology, particularly if the patient has a history of high-energy trauma or hip dislocation.
Femoral Head Fractures (Pipkin Lesions)
Malunion should be strongly suspected in patients who exhibit severely limited hip motion following a history of femoral head fractures. For example, literature reports have documented cases of femoral head avulsion fractures (Pipkin type I) that have malunited directly to the acetabulum, creating a bony block to motion.
* Management: In such complex scenarios, surgical débridement of the intra-articular malunion, often requiring surgical dislocation of the hip (Ganz approach), is necessary. Excellent functional results can be obtained after meticulous surgical débridement and restoration of the articular congruity, provided avascular necrosis (AVN) has not set in.
Postoperative Care and Rehabilitation
The postoperative protocol must be tailored to the patient's age, bone quality, and the rigidity of the internal fixation achieved.
Pediatric Postoperative Protocol
If complete correction has been secured and the fracture was fixed internally in a child, the mechanical hold of the implants is often insufficient to withstand the robust activity levels of a pediatric patient.
* Immobilization: A one-and-a-half spica cast should be applied immediately postoperatively and worn for a minimum of 8 weeks.
* Monitoring: Serial radiographs are required every 2 to 3 weeks to monitor for loss of reduction.
Adult Postoperative Protocol
In young adults with good bone stock and rigid fixation with a compression hip screw:
* Weight-Bearing: Patients are typically restricted to toe-touch weight-bearing (TTWB) or partial weight-bearing (PWB) for the first 6 to 8 weeks.
* Physical Therapy: Early passive and active-assisted range of motion exercises are initiated to prevent capsular adhesions and restore abductor strength. Progression to full weight-bearing is permitted only after radiographic evidence of bridging callus at the osteotomy site.
Complications and Long-Term Outcomes
The surgical correction of a cervicotrochanteric malunion is fraught with potential complications, and managing patient expectations preoperatively is paramount.
Loss of Correction (Varus Collapse)
Even with the most careful surgical technique and rigid internal fixation, a decrease in the angle between the neck and the femoral shaft (recurrent coxa vara) is fairly common. This can occur even after the osseous union appears to be solid on radiographs, particularly in patients with poor bone quality or non-compliant weight-bearing.
Prognosis in Children
In children, the results of this operation are usually disappointing. Due to the remodeling potential and the complex interplay of growth plates, only moderate improvement in position may be secured long-term. Because salvage procedures yield suboptimal results, the efficient and aggressive anatomical treatment of fresh cervicotrochanteric fractures in children is absolutely crucial to prevent malunion from occurring in the first place.
Prognosis in Young Adults
In young adults, the functional outcome is generally much improved following surgical correction. Patients typically experience significant relief of pain and an improvement in their Trendelenburg gait. However, the surgeon must counsel the patient that rarely, if ever, is the angle between the neck and shaft or the absolute length of the limb restored completely to its pre-injury state. A residual mild limb length discrepancy or slight limitation in terminal hip rotation is to be expected.
You Might Also Like