Surgical Management of Recurrent Joint Instability: Patellofemoral, Elbow, and Hip
Key Takeaway
Recurrent joint instability presents a complex biomechanical challenge requiring precise surgical intervention. This comprehensive guide details evidence-based approaches for managing patellofemoral, elbow, and hip instability. Key procedures include medial patellofemoral ligament (MPFL) reconstruction, tibial tubercle osteotomies, lateral ulnar collateral ligament (LUCL) repair, and hip capsulolabral reconstruction. Mastery of these techniques, grounded in rigorous anatomical understanding and biomechanical principles, is essential for restoring joint kinematics and preventing long-term degenerative arthropathy in the active patient population.
Comprehensive Introduction and Patho-Epidemiology
The management of recurrent joint instability demands a profound, multidimensional understanding of articular biomechanics, dynamic muscular restraints, and static ligamentous anatomy. Chronic instability not only severely limits patient function and athletic participation but also predictably leads to early-onset osteoarthritis due to abnormal contact stresses, repetitive microtrauma, and catastrophic chondral shear forces. Historically, orthopedic interventions often relied on non-anatomic tenodeses or isolated soft-tissue tightening procedures that failed to respect the native kinematics of the joint. Modern orthopedic surgery has undergone a paradigm shift toward anatomic reconstruction, recognizing that the restoration of native isometric ligamentous footprints and the correction of underlying osseous dysplasias are paramount to achieving durable, long-term stability.
Patellofemoral instability represents one of the most common manifestations of recurrent joint dislocation, particularly prevalent in the young, active, female demographic. The patho-epidemiology is distinctly multifactorial, driven by a complex interplay of osseous dysplasia (such as trochlear dysplasia), ligamentous incompetence (specifically the medial patellofemoral ligament), and lower extremity malalignment (increased Q-angle, valgus collapse, and rotational malalignment). First-time lateral patellar dislocations carry a recurrence rate approaching 40%, which skyrockets to nearly 70% following a second dislocation event. The cumulative effect of these recurrent subluxations is profound patellofemoral chondrosis, necessitating aggressive and precise surgical intervention to halt the degenerative cascade.
In the upper extremity, recurrent instability of the elbow is most frequently manifested as Posterolateral Rotatory Instability (PLRI). This pathology typically follows a traumatic elbow dislocation—often a fall on an outstretched hand resulting in axial compression, valgus stress, and supination—where the lateral ligamentous complex fails to heal isometrically. The epidemiology of PLRI is characterized by a spectrum of instability, defined eloquently by O'Driscoll, ranging from mild subluxation of the radiocapitellar joint to frank, recurrent dislocation. Patients often present not with frank dislocations, but with insidious mechanical symptoms, reporting a sensation of "giving way" when pushing off a chair or performing a push-up, highlighting the subtle yet debilitating nature of this pathoanatomy.
Conversely, recurrent dislocation of the native hip is a rare but devastating complication, typically occurring post-traumatically due to massive capsulolabral disruption, posterior wall acetabular fractures, or unrecognized intra-articular pathology. Atraumatic recurrent dislocations are exceedingly rare and are usually associated with generalized connective tissue disorders (e.g., Ehlers-Danlos syndrome, Marfan syndrome) or severe acetabular dysplasia. The patho-epidemiology of recurrent hip instability is rooted in a catastrophic failure of the static restraints, often exacerbated by a "Bankart-type" lesion of the hip, where the posterior capsule and labrum are avulsed from the acetabular rim. Recognizing the specific demographic and mechanical etiology of instability in each of these three distinct joints is the critical first step in formulating an effective, individualized surgical reconstruction plan.
Detailed Surgical Anatomy and Biomechanics
Patellofemoral Joint Anatomy and Kinematics
The stability of the patellofemoral joint relies on a delicate, synergistic balance between static and dynamic restraints. The medial patellofemoral ligament (MPFL) is the primary static restraint to lateral patellar translation, providing approximately 50% to 60% of the restraining force at early flexion (0° to 30°). Anatomically, the MPFL is located in layer 2 of the medial knee, residing deep to the superficial medial collateral ligament (sMCL) and blending intimately with the vastus medialis obliquus (VMO) aponeurosis. Its patellar insertion spans the proximal half to two-thirds of the medial patellar border, while its femoral origin is located in a highly specific anatomic saddle between the medial epicondyle and the adductor tubercle.
Biomechanically, the MPFL functions strictly as a check-rein rather than a dynamic retractor. It is most taut in full extension and early flexion; as the knee flexes beyond 30°, the patella engages the trochlear groove, and osseous geometry dictates stability. Therefore, a thorough understanding of the tibial tubercle-trochlear groove (TT-TG) distance and patellar height (measured via the Caton-Deschamps or Insall-Salvati indices) is mandatory. A TT-TG distance exceeding 20 mm significantly lateralizes the extensor mechanism force vector, rendering isolated soft-tissue reconstruction destined for failure due to excessive biomechanical overload.
Lateral Collateral Complex of the Elbow
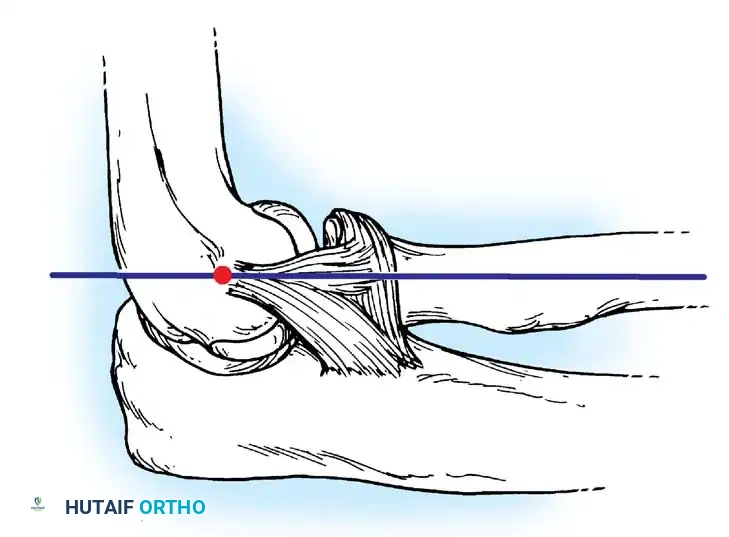
The lateral collateral ligament (LCL) complex of the elbow is the primary stabilizer against varus and external rotatory stress. It is a highly specialized tripartite structure consisting of the radial collateral ligament (RCL), the lateral ulnar collateral ligament (LUCL), and the annular ligament. The LUCL is the critical structure implicated in PLRI. It originates at the isometric point on the lateral epicondyle, located precisely at the center of the capitellar curvature, and inserts on the supinator crest of the proximal ulna.
Functionally, the LUCL acts as a hammock supporting the radial head. When this structure is incompetent, the radius and ulna supinate and subluxate posterolaterally away from the humerus as a single unit, pivoting on the intact medial collateral ligament (MCL). This kinematic derangement occurs primarily during elbow extension combined with forearm supination and axial load. Restoring the exact isometric footprint of the LUCL is paramount; even a 2 mm deviation in the humeral tunnel placement can result in graft laxity in extension or severe stiffness in flexion, obliterating the functional arc of motion.
Hip Acetabular and Capsulolabral Anatomy
The hip is an inherently stable ball-and-socket joint, fortified by the deepest osseous articulation in the human body and the thickest capsuloligamentous envelope. The static soft-tissue restraints include the robust iliofemoral ligament (Y-ligament of Bigelow) anteriorly, the ischiofemoral ligament posteriorly, and the pubofemoral ligament inferiorly. The acetabular labrum, a fibrocartilaginous ring encircling the acetabular rim, deepens the socket by 21% and, crucially, creates a fluid seal that provides a suction effect, enhancing stability and maintaining a pressurized layer of synovial fluid for cartilage nutrition.
In the setting of posterior hip instability, the ischiofemoral ligament and the posterior labrum are the primary structures compromised. Biomechanically, the hip is most vulnerable to posterior dislocation when positioned in flexion, adduction, and internal rotation—the classic "dashboard injury" posture. When a posterior dislocation occurs, it frequently results in a capsulolabral avulsion from the posterior-inferior and posterior-superior acetabular rim. Failure of these structures to heal anatomically leads to a patulous posterior capsule, abolishing the fluid seal and allowing the femoral head to translate posteriorly under physiologic loads, culminating in recurrent micro- or macro-instability.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for recurrent joint instability must be predicated on a meticulous clinical examination, advanced cross-sectional imaging, and a comprehensive understanding of the patient's physiologic demands. Operative management is generally indicated when conservative measures—including prolonged, targeted physical therapy focusing on dynamic muscular stabilizers, proprioceptive retraining, and functional bracing—have been exhausted without achieving symptomatic relief. The surgeon must differentiate between primary traumatic events, which may occasionally be managed non-operatively, and recurrent instability, which almost universally requires surgical reconstruction to prevent progressive articular degradation.
Absolute contraindications to any joint reconstruction include active intra-articular or peri-articular infection, severe medical comorbidities precluding safe anesthesia, and end-stage degenerative joint disease. In the presence of advanced osteoarthritis, soft-tissue stabilization procedures will not alleviate the patient's pain and may paradoxically exacerbate symptoms by altering joint kinematics and increasing contact pressures on compromised chondral surfaces. In such scenarios, arthroplasty or arthrodesis must be considered. Relative contraindications include profound generalized ligamentous laxity without a clear traumatic etiology, voluntary dislocators (often associated with psychiatric overlays), and uncorrected, severe osseous malalignment that would predictably overload the reconstructed ligaments.
For patellofemoral instability, isolated MPFL reconstruction is contraindicated in the presence of severe bony dysplasia, such as a TT-TG distance greater than 20 mm or severe patella alta (Caton-Deschamps > 1.2). In these cases, osseous realignment via a tibial tubercle osteotomy (TTO) must be performed concomitantly. Similarly, in the elbow, LUCL reconstruction is contraindicated if there is an unaddressed, massive coronoid fracture or severe radial head deficiency, as the bony architecture must be restored to provide a foundation for soft-tissue stability. In the hip, capsulolabral repair is insufficient if there is a posterior wall acetabular fracture encompassing more than 20-30% of the articular surface; such defects require structural bone grafting or rigid internal fixation.
| Joint System | Primary Procedure | Key Surgical Indications | Absolute & Relative Contraindications |
|---|---|---|---|
| Patellofemoral | MPFL Reconstruction ± TTO | Recurrent lateral dislocations; Failed conservative therapy; TT-TG > 20mm (requires TTO); Patella alta. | End-stage patellofemoral osteoarthritis; Fixed lateral patellar tilt without release; Uncorrected severe valgus alignment. |
| Elbow | LUCL Reconstruction | Symptomatic recurrent PLRI; Positive lateral pivot-shift test; Inability to perform push-ups/weight-bearing tasks. | Severe radiocapitellar arthritis; Unreconstructed coronoid/radial head fractures; Active joint infection. |
| Hip | Posterior Capsulolabral Repair | Recurrent posterior subluxation/dislocation; MRI-proven posterior labral/capsular avulsion; Intractable pain with flexion/IR. | Large, ununited posterior wall fractures (>25%); Advanced avascular necrosis (AVN); Severe acetabular retroversion. |
Pre-Operative Planning, Templating, and Patient Positioning
Patellofemoral Planning and Positioning
Meticulous pre-operative imaging is the cornerstone of patellofemoral surgery. A standard radiographic series must include weight-bearing anteroposterior, true lateral (to assess trochlear dysplasia via the crossing sign, supratrochlear spur, and double contour sign), and axial Merchant views. However, a fine-cut Computed Tomography (CT) scan or Magnetic Resonance Imaging (MRI) is mandatory to precisely calculate the TT-TG distance and evaluate the tibial tubercle-posterior cruciate ligament (TT-PCL) distance. The Dejour classification should be utilized to categorize trochlear dysplasia, dictating whether a trochleoplasty might be necessary in extreme cases (Type B or D).
In the operating theater, the patient is placed supine on a radiolucent table. A high thigh tourniquet is applied, and the operative leg is secured in a leg holder or a lateral post setup that allows full, unencumbered range of motion from 0° to 120° of flexion. This dynamic mobility is absolutely critical, as the MPFL graft must be tensioned and evaluated through a full functional arc to ensure it does not over-constrain the medial compartment in deep flexion. A diagnostic arthroscopy setup is prepared to evaluate chondral surfaces and remove any loose bodies prior to the open reconstruction.
Elbow PLRI Planning and Positioning
Pre-operative evaluation of the elbow requires standard AP, lateral, and oblique radiographs to rule out subtle fractures or heterotopic ossification. Fluoroscopic stress views under anesthesia can be invaluable for confirming the diagnosis of PLRI. If osseous defects of the radial head or capitellum are suspected, a 3D-reconstructed CT scan is highly recommended to quantify the bone loss. MRI is useful for evaluating the integrity of the common extensor origin and confirming the attenuation or avulsion of the LUCL complex.
Patient positioning for LUCL reconstruction can be tailored to surgeon preference, utilizing either the supine or lateral decubitus position. In the supine position, the arm is draped freely across the chest, which allows excellent access to the lateral aspect of the elbow and facilitates intra-operative assessment of the pivot-shift maneuver. Alternatively, the lateral decubitus position with the arm resting over a radiolucent post provides exceptional stability and visualization, particularly if concomitant posterior or medial procedures are anticipated. A sterile tourniquet is applied high on the brachium to ensure a bloodless surgical field.
Hip Capsulolabral Planning and Positioning
For recurrent posterior hip instability, high-resolution MRI or MR arthrography is the gold standard for delineating labral tears, capsular avulsions (the hip equivalent of a Bankart lesion), and the presence of intra-articular loose bodies. A CT scan with 3D reconstructions is critical if there is any history of high-energy trauma to evaluate for subtle posterior wall fractures, marginal impaction, or intra-articular osseous fragments that could act as a fulcrum, levering the hip out of the socket.
The patient is meticulously positioned in the lateral decubitus position on a radiolucent operating table. Rigid pelvic fixation is absolutely paramount; this is achieved using a combination of a peg board, rigid anterior and posterior pubic/sacral supports, or a heavy-duty bean bag. The operative leg is draped free to allow for dynamic manipulation during the procedure, facilitating dislocation and reduction of the femoral head as needed to access the posterior acetabular rim. All pressure points, particularly the peroneal nerve on the down leg and the axilla, must be heavily padded to prevent positioning-related neuropraxias during these often lengthy procedures.
Step-by-Step Surgical Approach and Fixation Technique
Medial Patellofemoral Ligament Reconstruction and Tibial Tubercle Osteotomy
The procedure begins with a diagnostic arthroscopy to address any chondral shearing injuries. For the MPFL reconstruction, a semitendinosus or gracilis autograft is harvested using a standard anteromedial tibial incision and whipstitched with non-absorbable #2 high-tensile suture. Attention is then turned to the patella. A 2-3 cm longitudinal incision is made over the medial border of the upper half of the patella. The extensor retinaculum is incised, and two transverse 3.2 mm blind tunnels are drilled in the proximal two-thirds of the medial patellar edge. The graft limbs are secured into these tunnels using bio-composite suture anchors or small interference screws.
Identification of the femoral isometric point is the most technically demanding step. A 2 cm incision is made between the medial epicondyle and the adductor tubercle. Using strict lateral fluoroscopy, Schöttle's Point is identified: 1 mm anterior to the posterior cortex extension line, 2.5 mm distal to the posterior origin of the medial femoral condyle, and proximal to Blumensaat's line. A guide pin is placed here. The graft is then routed from the patella to the femoral incision between layer 2 (capsule) and layer 1 (deep fascia). The knee is cycled through a full range of motion. The graft must be tensioned with the knee at exactly 30° of flexion to restore the anatomic check-rein effect. It is secured with a bioabsorbable interference screw.
If a TTO is indicated (TT-TG > 20 mm), a longitudinal incision is made lateral to the tibial crest. An oblique osteotomy (Fulkerson anteromedialization) is performed using an oscillating saw, starting proximal to the patellar tendon insertion and exiting distally along the anterior tibial crest (typically 5-7 cm in length). The tubercle is translated medially and anteriorly to decompress the joint and normalize the TT-TG distance. The osteotomy is temporarily pinned, tracking is verified arthroscopically, and rigid fixation is achieved with two 4.5 mm cortical lag screws directed from anterior to posterior.
Lateral Ulnar Collateral Ligament Reconstruction
The surgical approach for LUCL reconstruction utilizes the classic Kocher interval between the anconeus and the extensor carpi ulnaris. The common extensor origin is carefully elevated anteriorly to expose the lateral epicondyle and the radiocapitellar joint. The exact isometric footprint of the LUCL is identified on the lateral epicondyle at the center of the capitellar curvature. On the ulnar side, the supinator crest is exposed. Two converging 3.2 mm tunnels are drilled at the anatomic insertion of the LUCL, ensuring a robust 1 cm bone bridge remains between the tunnels to prevent iatrogenic fracture.
A blind tunnel or converging tunnels are then drilled at the isometric point on the lateral epicondyle. A palmaris longus or gracilis autograft is prepared and passed through the ulnar tunnels. The two limbs of the graft are routed proximally and passed into the humeral tunnel. Tensioning of the LUCL graft is a critical maneuver: it must be performed with the elbow in 30° to 40° of flexion and the forearm in maximum pronation. Pronation tightens the intact medial soft tissues and perfectly reduces the radiocapitellar joint, ensuring the graft is fixed in the anatomic position without capturing the joint in subluxation. Fixation is achieved using an interference screw or robust suture anchors.
Posterior Hip Capsulolabral Reconstruction
The surgical management of recurrent posterior hip instability requires a standard Kocher-Langenbeck approach. The gluteus maximus is split in line with its fibers. The sciatic nerve is meticulously identified and protected throughout the entirety of the procedure. The short external rotators (piriformis, obturator internus, and the gemelli) are tenotomized near their femoral insertion and reflected posteriorly over the sciatic nerve to act as a protective cushion. A T-shaped capsulotomy is performed, or the traumatic capsular rent is utilized. The hip is gently distracted, and the joint is meticulously cleared of all intra-articular loose bodies, debris, and organized hematoma.
The posterior acetabular rim is debrided to bleeding cancellous bone using a high-speed burr or curettes to promote a robust healing response. A modified Bankart repair of the hip is then performed. Two to three robust suture anchors are placed strategically along the posterior-superior and posterior-inferior acetabular rim. The sutures are passed through the avulsed labrum and the thick posterior capsule. The sutures are tied with the hip held in slight extension, abduction, and external rotation to maximally tension the posterior capsular repair. If severe capsular redundancy is noted, a formal capsular shift is performed by advancing the inferior leaflet superiorly. The short external rotators are then repaired anatomically to provide a dynamic buttress.
Complications, Incidence Rates, and Salvage Management
Surgical reconstruction for recurrent joint instability carries a unique set of complications that range from minor wound healing issues to catastrophic joint failure. Across all procedures, general surgical risks such as surgical site infection, deep vein thrombosis (DVT), and pulmonary embolism (PE) remain present, necessitating appropriate peri-operative antibiotic prophylaxis and mechanical or pharmacologic thromboprophylaxis tailored to the patient's risk profile. However, the most profound complications are inherently biomechanical, stemming from technical errors in graft placement, tensioning, or failure to recognize concurrent osseous pathology.
In patellofemoral surgery, the most devastating and common complication is over-tensioning of the MPFL graft. If the graft is tensioned in full extension or if the femoral tunnel is placed too proximal, the graft will act as a tether during deep flexion. This leads to severe medial patellofemoral articular overload, intractable anterior knee pain, loss of flexion, and iatrogenic medial subluxation. Salvage requires prompt arthroscopic or open release of the graft. Conversely, non-anatomic placement of the LUCL graft in the elbow (typically placing the humeral tunnel too anteriorly) will result in a graft that is tight in extension but lax in flexion, leading to recurrent PLRI.
Posterior hip reconstruction carries significant neurologic risks. The sciatic nerve is at extreme risk during the Kocher-Langenbeck approach, particularly in the setting of dense, post-traumatic scar tissue. Iatrogenic sciatic nerve palsy (predominantly affecting the peroneal division) can occur from excessive retraction or direct injury. Furthermore, extensive dissection of the posterior capsule and short external rotators risks disrupting the medial femoral circumflex artery (MFCA) blood supply to the femoral head, leading to avascular necrosis (AVN). Salvage for AVN or severe post-traumatic arthritis in this demographic inevitably requires total hip arthroplasty (THA).
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Strategy / Management |
|---|---|---|---|
| MPFL Over-tensioning | 5% - 10% | Tensioning in extension; Proximal femoral tunnel malposition. | Early recognition; Arthroscopic or open graft release/revision. |
| Recurrent PLRI (Elbow) | 8% - 15% | Non-isometric tunnel placement; Premature return to heavy lifting. | Revision LUCL reconstruction with allograft; Evaluation of bony alignment. |
| Sciatic Nerve Palsy | 2% - 8% | Excessive retractor pressure; Direct trauma during hip approach. | Immediate removal of compressive hematoma; AFO bracing; Nerve exploration if transected. |
| Femoral Head AVN | 3% - 12% | Disruption of MFCA during posterior hip exposure/trauma. | Core decompression (early stage); Total Hip Arthroplasty (late stage). |
Phased Post-Operative Rehabilitation Protocols
Patellofemoral Rehabilitation
The rehabilitation following MPFL reconstruction with or without TTO is meticulously phased to protect the healing soft tissues and osteotomy while preventing arthrofibrosis. During Phase I (Weeks 0-2), the knee is immobilized in a hinged brace locked in full extension. Weight-bearing is permitted as tolerated with crutches, strictly in extension to prevent eccentric quadriceps loading on the TTO. Passive range of motion (ROM) is initiated from 0° to 30°. In Phase II (Weeks 2-6), ROM is gradually advanced to 90° as tolerated. Isometric quadriceps strengthening and straight-leg raises are initiated, ensuring no extensor lag develops.
Phase III (Weeks 6-12) marks the transition to dynamic stabilization. The hinged brace is discontinued once the patient demonstrates adequate quadriceps control and a normalized gait pattern. Rehabilitation shifts toward closed-chain kinetic exercises (e.g., mini-squats, leg presses) to minimize patellofemoral joint reaction forces while maximizing VMO hypertrophy. Phase IV (Months 4-6) is focused on sport-specific activities, plyometrics, and agility drills. Return to competitive sports is permitted only after the patient achieves >90% limb symmetry on functional hop testing and demonstrates complete radiographic union of the TTO.
Elbow LUCL Rehabilitation
Post-operative management of LUCL reconstruction requires a delicate balance between protecting the lateral soft-tissue envelope and preventing elbow stiffness, which is notoriously difficult to treat. In Phase I (Weeks 0-2), the elbow is rigidly splinted in 90° of flexion and full forearm pronation. This position maximizes the contact area of the radiocapitellar joint and removes all tension from the reconstructed LUCL. During Phase II (Weeks 2-6), the patient is transitioned to a hinged elbow brace locked in full pronation. Active and active-assisted ROM is permitted from 30° to 130°. Terminal extension and supination are strictly prohibited, as these motions place maximal stress on the healing graft.
As the patient enters Phase III (Weeks 6-12), the hinged brace is gradually weaned. Supination is slowly introduced, initially only in deep flexion where the joint is most congruous and stable. Progressive isometric and isotonic strengthening of the triceps, biceps, and common extensor mass is initiated. Phase IV (Months 4-6) involves a return to unrestricted heavy lifting and sports. Patients are counseled that achieving terminal extension may take up to a year, and a mild flexion contracture (5°-10°) is often considered an acceptable, even protective, outcome following complex instability reconstruction.
Hip Capsulolabral Rehabilitation
Rehabilitation following posterior capsulolabral reconstruction of the hip is highly restrictive to prevent early failure of the delicate capsular repair. In Phase I (Weeks 0-6), the patient is placed in a customized hip abduction orthosis that limits flexion to 70°, with a strict block at 0° of internal rotation and 0° of adduction. Weight-bearing is restricted to touch-down (toe-touch) only. The primary goal is to protect the posterior structures from any stretch or tension while allowing early, safe mobilization to prevent DVT and maintain cartilage nutrition.
During Phase II (Weeks 6-12), the abduction brace is discontinued. Weight-bearing is progressively advanced by 25% per week until full weight-bearing is achieved. Active-assisted and active ROM exercises are initiated, but the combined position of flexion, adduction, and internal rotation must still be strictly avoided. Phase III (Months 3-6) focuses heavily on abductor and external rotator strengthening to provide dynamic stability to the pelvis and hip joint. Return to high-impact activities, pivoting sports, or heavy manual labor is generally restricted until 6 to 9 months postoperatively, contingent upon radiographic confirmation of joint congruity and clinical evidence of robust dynamic stability.
Summary of Landmark Literature and Clinical Guidelines
The contemporary surgical management of recurrent joint instability is heavily predicated on landmark biomechanical and clinical studies that have redefined our understanding of joint kinematics. In the realm of patellofemoral instability, the work of Dejour et al. (1994) remains the foundational text on the pathoanatomy of the patellofemoral joint, establishing the critical thresholds for trochlear dysplasia, patella alta, and the TT-TG distance. Furthermore, the anatomic studies by Schöttle et al. (2006) revolutionized MPFL reconstruction by defining the precise radiographic landmarks for the femoral isometric point, drastically reducing the incidence of iatrogenic medial compartment overload and graft failure.
For elbow posterolateral rotatory instability, the seminal paper by O'Driscoll, Bell, and Morrey (1991) first defined the clinical entity of PLRI and established the lateral ulnar collateral ligament as the primary restraint to this specific kinematic derangement. Subsequent biomechanical studies by Cohen and Hastings refined our understanding of the isometric properties of the lateral collateral complex, leading to the development of the anatomic, dual-tunnel ulnar reconstruction techniques utilized today. Clinical guidelines now universally recommend anatomic LUCL reconstruction over non-anatomic tenodeses for symptomatic PLRI.
In the management of recurrent hip instability, the literature is driven by the evolution of hip arthroscopy and advanced open surgical dislocation techniques pioneered by Ganz et al. (2001). The recognition of the hip labrum as a critical structure for the fluid seal and joint stability—rather than merely a vestigial appendage—has shifted the paradigm toward labral repair rather than debrid
