Surgical Management of Rheumatoid Arthritis of the Spine
Key Takeaway
Rheumatoid arthritis of the cervical spine is a progressive inflammatory condition leading to atlantoaxial subluxation, basilar impression, and subaxial instability. Left untreated, cervical myelopathy carries a high mortality rate. Surgical management is indicated for neurological deficits, intractable pain, or critical radiographic instability. This guide details the biomechanical evaluation, essential radiographic measurements, and step-by-step operative techniques for posterior cervical and occipitocervical fusion.
PATHOPHYSIOLOGY AND NATURAL HISTORY
Rheumatoid arthritis (RA) is a systemic, chronic inflammatory disorder characterized by a lymphoproliferative disease process within the synovium. In the cervical spine, this erosive synovitis leads to the formation of a destructive pannus that aggressively degrades articular cartilage, subchondral bone, and critical ligamentous restraints. The cervical spine is the most frequently involved region of the axial skeleton in RA, with disease activity often correlating with the severity of appendicular joint involvement.
The natural history of rheumatoid cervical spine disease is characterized by progressive instability, neurological deterioration, and, ultimately, severe morbidity or death if left untreated. The inflammatory cascade primarily targets the synovial joints of the upper cervical spine, including the atlanto-odontoid, atlantoaxial, and atlanto-occipital articulations. As the transverse, alar, and apical ligaments are destroyed, biomechanical failure ensues.
Clinical Pearl: The incidence of sudden death from the combination of basilar impression and atlantoaxial instability is approximately 10%. Furthermore, in patients with established cervical myelopathy who refuse surgical intervention, mortality approaches 100% within 7 years of symptom onset.
Other predictive factors for severe spinal involvement include a longer duration of the disease, seropositivity for rheumatoid factor, chronic corticosteroid use, and male sex. Although patients with RA generally have a shorter life expectancy than the normal population, aggressive identification and management of cervical instability are paramount to preventing catastrophic neurological sequelae.
CLINICAL PRESENTATION
The clinical manifestations of rheumatoid cervical spine instability are often insidious. Many patients remain asymptomatic despite profound radiographic abnormalities. When symptoms arise, they typically include:
* Mechanical Neck Pain: Often the earliest symptom, characterized by severe occipital or suboccipital pain and stiffness.
* Neurological Deficits: Pyramidal tract involvement manifests as weakness, gait clumsiness, and loss of fine motor skills.
* Myelopathic Signs: Early clinical indicators include hyperreflexia, a positive Hoffmann sign, a positive Babinski reflex, and sustained clonus.
* Lhermitte’s Sign: An electric shock-like sensation radiating down the spine or limbs upon neck flexion.
* Vertebrobasilar Insufficiency: Tinnitus, vertigo, visual disturbances, or dysphagia resulting from vertebral artery compression or brainstem ischemia due to cranial settling.
CLASSIFICATION OF CERVICAL INSTABILITY
Rheumatoid involvement of the cervical spine presents in three distinct, often overlapping, patterns of instability:
1. Atlantoaxial Subluxation (AAS)
AAS is the most common form of instability, identified in 11% to 46% of RA patients at necropsy. It results from erosive synovitis of the atlantoaxial and atlantoodontoid joints, leading to the incompetence of the transverse ligament. Subluxation can be anterior (most common), posterior (20%), or lateral (7%). Lateral subluxation implies rotation of the atlas and is diagnosed when the lateral masses of C1 lie 2 mm or more laterally than those of C2.
2. Basilar Impression (Vertical Settling / Atlantoaxial Impaction)
Basilar impression represents the catastrophic settling of the skull onto the atlas, and the atlas onto the axis, secondary to severe bone loss and articular destruction. This superior migration of the odontoid into the foramen magnum directly compresses the cervicomedullary junction and can lead to vertebral artery thrombosis. As AAS progresses, vertical instability frequently develops; paradoxically, as superior migration occurs, the anterior atlantodens interval (ADI) may decrease, masking the severity of the instability.
3. Subaxial Subluxation (SAS)
Affecting 10% to 20% of RA patients, SAS is characterized by a cascading or "staircase" appearance of the middle and lower cervical spine. It is driven by synovitis of the facet and uncovertebral joints, combined with erosion of the vertebral endplates. This multi-level instability frequently results in foraminal narrowing, root compression, and dynamic cord compression.
RADIOGRAPHIC EVALUATION AND CRITICAL MEASUREMENTS
A rigorous radiographic evaluation is mandatory for all RA patients. Standard imaging includes a five-view cervical spine series (AP, lateral, open-mouth odontoid, and dynamic flexion-extension lateral views).
Atlantoaxial Measurements
- Atlantodens Interval (ADI): Measured between the posterior edge of the anterior ring of C1 and the anterior edge of the odontoid. Normal is ≤ 3.5 mm in adults. An ADI > 10 to 12 mm is clinically significant, indicating complete transverse ligament disruption. However, ADI is a poor predictor of neurological sequelae because it does not account for soft-tissue pannus.
- Posterior Atlantodens Interval (PADI) / Space Available for the Cord (SAC): The true predictor of neurological recovery. It is measured from the posterior aspect of the odontoid to the anterior aspect of the posterior ring of C1.
- Critical Thresholds: If the SAC is < 10 mm, neurological recovery is not expected. If basilar impression coexists, significant recovery requires an SAC of at least 13 mm. Decompression and stabilization must be considered if the SAC is ≤ 14 mm.
Basilar Impression Measurements
Accurate diagnosis of vertical settling requires specific craniometric lines.
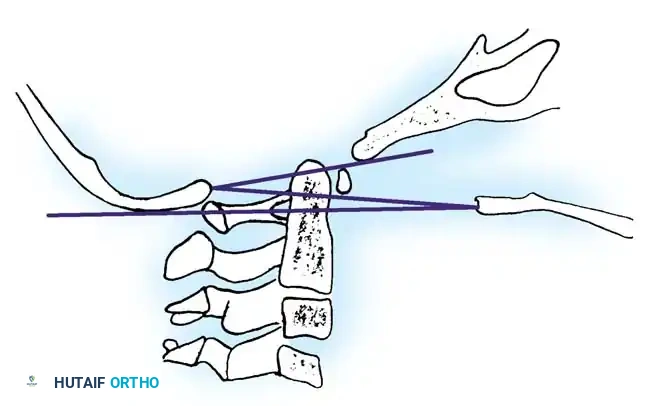
Fig. 1: Drawing of the base of the skull and upper spine showing the McGregor line, McRae line, and Chamberlain line.
- McGregor Line: Drawn from the posterior margin of the hard palate to the most caudal point of the occipital curve. Superior migration is diagnosed if the tip of the odontoid projects > 4.5 mm above this line.
- Ranawat Method: Measures the distance from the center of the C2 pedicles to a line connecting the centers of the anterior and posterior arches of C1.
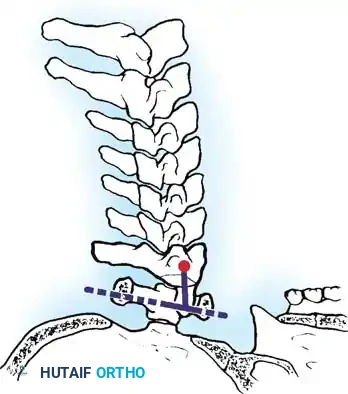
Fig. 2: Measurement of superior migration using the Ranawat method.
Normal values are 15 mm for women and 17 mm for men. A value of < 13 mm is considered definitively abnormal.
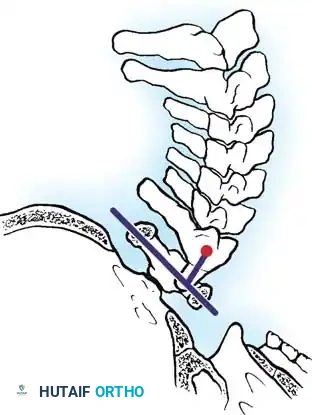
Fig. 3: Ranawat measurement in extension.
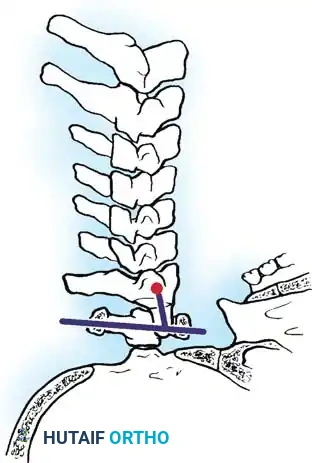
Fig. 4: Ranawat measurement in flexion. Note that the measurement of superior migration remains relatively unchanged during dynamic motion.
- Redlund-Johnell Method: Measures the minimal distance between the McGregor line and the midpoint of the inferior margin of the C2 vertebral body on a neutral lateral radiograph.
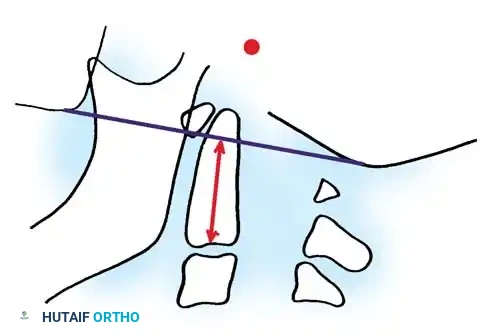
Fig. 5: Determination of vertebral settling using the Redlund-Johnell method.
Normal values are ≥ 34 mm for men and ≥ 29 mm for women. Studies indicate this is one of the most predictive screening methods for basilar impression.
Subaxial Measurements
Any subaxial slippage of ≥ 4 mm, or 20% of the adjacent vertebral body width, is considered significant. A sagittal spinal canal diameter of < 13 mm places the patient at high risk for spinal cord compression.
Advanced Imaging: MRI and CT Myelography
Three-dimensional imaging is imperative for patients with neurological deficits or radiographic instability.
* Magnetic Resonance Imaging (MRI): The gold standard for evaluating soft tissues, neural elements, and the retro-odontoid pannus. Pannus decreases the SAC by ≥ 3 mm in approximately 66% of patients. MRI is 100% accurate in identifying vertical settling. Flexion-extension MRI can uniquely demonstrate dynamic cord compression.
* Cervicomedullary Angle: Measured on sagittal MRI. A line along the dorsal surface of the odontoid intersects a line parallel to the ventral medulla. Normal is 135° to 175°. An angle < 135° indicates severe atlantoaxial impaction and correlates strongly with myelopathy.
* CT Myelography: Utilized if MRI is contraindicated. It provides excellent bony detail and delineates the true space available for the cord.
NONOPERATIVE MANAGEMENT
The goals of nonoperative treatment are to prevent neurological injury, avoid sudden death, minimize pain, and maximize functional independence.
- Medical Management: Aggressive pharmacological control of the systemic disease using Disease-Modifying Antirheumatic Drugs (DMARDs) and biologic agents is essential. This must be coordinated closely with a rheumatologist.
- Orthoses: A rigid cervical collar (e.g., Philadelphia collar) may alleviate mechanical pain but does not halt the progression of instability.
- Physical Therapy: Isometric neck exercises help stabilize the cervical musculature without inducing excessive, potentially dangerous motion.
- Surveillance: Asymptomatic patients with radiographic abnormalities require strict yearly follow-up with five-view cervical radiographs to detect progressive instability before irreversible neurological deficits occur.
SURGICAL MANAGEMENT
Indications for Surgery
Surgical intervention is indicated for intractable pain, progressive neurological impairment, or critical radiographic instability.
Surgical Warning: Boden et al. established strict criteria for prophylactic arthrodesis in RA patients, even in the absence of neurological deficits. Surgery is indicated if:
* The posterior atlantoodontoid interval (SAC) is ≤ 14 mm.
* AAS is accompanied by ≥ 5 mm of basilar invagination.
* Subaxial subluxation presents with a sagittal canal diameter ≤ 14 mm.
* Axial imaging demonstrates absolute spinal cord compression to a diameter of < 6 mm.
Preoperative Planning and Positioning
- Airway Management: Awake fiberoptic intubation is mandatory to avoid hyperextension of the unstable cervical spine during induction.
- Neuromonitoring: Somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs) must be utilized throughout the procedure.
- Positioning: The patient is placed prone using Mayfield skull tongs. Extreme care is taken to maintain a neutral neck position. A trial of preoperative halo or tong traction may be utilized to reduce basilar impression or subaxial subluxations.
Operative Techniques
1. Posterior C1-C2 Fusion (For Atlantoaxial Subluxation)
AAS without basilar impression is best treated with a posterior C1-C2 arthrodesis.
* Technique: Modern constructs utilize C1 lateral mass screws combined with C2 pedicle or pars screws (Harms-Goel technique). This provides superior biomechanical rigidity compared to historical wiring techniques (e.g., Gallie or Brooks-Jenkins) and often obviates the need for postoperative halo immobilization.
* Transarticular Screws: Magerl transarticular screws (C2 to C1) are an excellent alternative but require meticulous preoperative CT evaluation to ensure the vertebral artery is not anomalous or at risk.
* Pannus Management: Direct excision of the retro-odontoid pannus is rarely necessary. Rigid posterior stabilization induces spontaneous regression of the inflammatory pannus. Odontoidectomy is reserved strictly for cases where anterior bony compression persists despite reduction and posterior fusion.
2. Occipitocervical Fusion (For Basilar Impression)
Basilar impression requires extension of the fusion to the occiput.
* Reduction: Preoperative traction is attempted. If the impaction is reducible, a posterior occipitocervical fusion is performed in the reduced position.
* Instrumentation: Fixation is achieved using an occipital plate fixed with bicortical screws, connected via rods to cervical lateral mass or pedicle screws. Corticocancellous autograft from the iliac crest is decorticated and laid over the posterior elements.
* Irreducible Deformity: If the basilar impression is irreducible and causing ventral brainstem compression, an anterior transoral odontoidectomy must be performed to decompress the neuraxis, followed immediately by a posterior occipitocervical fusion. Posterior decompression (suboccipital craniectomy and C1 laminectomy) may also be required.
3. Subaxial Posterior Fusion (For Subaxial Subluxation)
Symptomatic SAS is treated with posterior decompression and instrumented fusion.
* Approach: Anterior cervical discectomy and fusion (ACDF) has historically yielded unsatisfactory results in RA patients due to poor bone quality and high subsidence rates. Posterior fusion is the gold standard.
* Instrumentation: Lateral mass screws are utilized in the subaxial spine (C3-C6). At C7 and T1, where lateral masses are thin, transpedicular fixation provides superior pull-out strength.
* Bone Grafting: Copious autogenous bone graft is placed laterally over the decorticated facet joints. In cases of profound osteopenia, polymethylmethacrylate (PMMA) cement augmentation around the screws may be considered to enhance immediate stability.
POSTOPERATIVE PROTOCOLS AND OUTCOMES
Rehabilitation and Orthoses
Postoperatively, patients are typically managed in a rigid cervical orthosis (e.g., Miami J or Philadelphia collar) for 6 to 12 weeks, depending on bone quality and construct rigidity. Early mobilization is encouraged to prevent pulmonary and thromboembolic complications.
Clinical Outcomes
- Pain Relief: Surgical stabilization is highly effective for mechanical symptoms, with 90% to 97% of patients reporting significant pain reduction.
- Neurological Recovery: Recovery is heavily dependent on the preoperative severity of the deficit (Ranawat classification).
- Patients with isolated AAS show neurological improvement in up to 95% of cases.
- Patients with combined AAS and basilar impression have a more guarded prognosis (76% improvement).
- Ambulatory patients with myelopathy (Ranawat Class IIIA) have a 58% chance of improvement, whereas nonambulatory, severely myelopathic patients (Ranawat Class IIIB) have only a 20% chance of meaningful recovery.
Complications
Surgery in the rheumatoid spine carries significant risk. The mortality rate associated with these complex reconstructions ranges from 8% to 20%, largely due to the systemic fragility of the patient population. Furthermore, the altered biology and chronic immunosuppression in RA patients contribute to a high nonunion (pseudoarthrosis) rate of 20% to 33%. Meticulous surgical technique, rigid modern instrumentation, and robust autogenous bone grafting are critical to minimizing these risks and achieving a successful arthrodesis.
📚 Medical References
- rheumatoid cervical spine for the non-ambulant myelo pathic patient—too much, too late? Lancet 347:1004, 1996.
- Casey AT, Crockard HA, Pringle J, et al: Rheumatoid arthritis of the cervical spine: current techniques for management, Orthop Clin North Am 33:291, 2002.
- Chiba H, Annen S, Shimada T, et al: Atlantoaxial subluxation complicated by diffuse idiopathic skeletal hyperostosis, Spine 17:1414, 1992.
- Clark CR: Occipitocervical fusion for the unstable rheumatoid neck, Orthopedics 12:469, 1989.
- Clark CR, Goetz DD, Menezes AH: Arthrodesis of the cervical spine in rheumatoid arthritis, J Bone Joint Surg 71A:381, 1989.
- Cocke EW, Robertson JH, Robertson JT, et al: The extended maxillotomy and subtotal maxillectomy for excision of skull base tumors, Arch Otolaryngol Head Neck Surg 116:92, 1990.
- Conlon PW, Isdale IC, Rose BS: Rheumatoid arthritis of the cervical spine: an analysis of 333 cases, Ann Rheum Dis 25:120, 1966.
- Crandall PH, Gregorius FK: Long-term follow-up of surgical treatment of cervical spondylotic myelopathy, Spine 2:139, 1977.
- Crockard A, Grob D: Rheumatoid arthritis: upper cervical involvement. In The Cervical Spine Research Society, Editorial Committee: The cervical spine, 3rd ed, Philadelphia, 1998, Lippincott-Raven. Crockard HA: Surgical management of cervical rheumatoid problems, Spine 20:2584, 1995.
- de los Reyes RA, Malik GM, Wu KK, et al: A new surgical approach to stabilizing C1-2 subluxation in rheumatoid arthritis, Henry Ford Hosp Med J 29:127, 1981.
- Dreyer SJ, Boden SD: Natural history of rheumatoid arthritis of the cervical spine, Clin Orthop Relat Res 366:98, 1999.
- Edwards WC, LaRocca H: The developmental segmental sagittal diameter of the cervical spinal canal in patients with cervical spondylosis, Spine 8:20, 1983.
- Epstein JA, Carras R, Hyman RA, et al: Cervical myelopathy caused by developmental stenosis of the spinal canal, J Neurosurg 51:362, 1979.
- Fehring TK, Brooks AL: Upper cervical instability in rheumatoid arthritis, Clin Orthop Relat Res 221:137, 1987.
- Floyd AS, Learmonth ID, Mody SAG, et al: Atlantoaxial instability and neurologic indicators in rheumatoid arthritis, Clin Orthop Relat Res 241:177, 1989.
- Freeman GE Jr: Correction of severe deformity of the cervical spine in ankylosing spondylitis with the halo device, J Bone Joint Surg 43A:547, 1961.
- Fujiwara K, Jufi moto M, Owaki H, et al: Cervical lesions related to the systemic progression in rheumatoid arthritis, Spine 23:2052, 1998.
- Fujiwara K, Owaki H, Fujimoto M, et al: A long-term follow-up study of cervical lesions in rheumatoid arthritis, J Spinal Disord 13:519, 2000.
- Fujiwara K, Yonenobu K, Ochi T: Natural history of upper cervical lesions in rheumatoid arthritis, J Spinal Disord 10:275, 1997.
- Goel MK: Vertebral osteotomy for correction of fi xed fl exion deformity of the spine, J Bone Joint Surg 50A:287, 1968.
- Grob D, Schutz U, Poltz G: Occipitocervical fusion in patients with rheumatoid arthritis, Clin Orthop Relat Res 366:46, 1999.
- Gui L, Merlini L, Savini R, et al: Cervical myelopathy due to ossifi cation of the posterior longitudinal ligament, Ital J Orthop Traumatol 9:269, 1983.
- Hadley MN, Spetzler RT, Sonntag VKH: The transoral approach to the cervical spine: a review of 53 cases of extradural cervicomedullary compression, J Neurosurg 71:16, 1989.
- Harta S, Tohno S, Kawagishi T: Osteoarthritis of the atlantoaxial joint, Int Orthop 5:277, 1981.
- Herbert JJ: Vertebral osteotomy, technique, indications, and results, J Bone Joint Surg 30A:680, 1948.
- Herbert JJ: Vertebral osteotomy for kyphosis, especially in MarieStrümpell arthritis: a report on fi fty cases, J Bone Joint Surg 41A:291, 1959.
- Heywood AWB, Learmonth ID, Thomas M: Cervical spine instability in rheumatoid arthritis, J Bone Joint Surg 70B:702, 1988.
- Hirabayashi K, Watanabe K, Wakano K, et al: Expansive opendoor laminoplasty for cervical spinal stenotic myelopathy, Spine 8:693, 1983.
- Hoff J, Nishimura M, Pitts L, et al: The role of ischemia in the pathogenesis of cervical spondylotic myelopathy: a review and new microangiographic evidence, Spine 2:100, 1977.
- Hukuda S, Mochizuki T, Ogata M, et al: The pattern of spinal and extraspinal hyperostosis in patients with ossifi cation of the posterior longitudinal ligament and the ligamentum fl avum causing myelopathy, Skeletal Radiol 10:79, 1983.
- Jacobs B, Krueger EG, Leivy DM: Cervical spondylosis with radiculopathy, JAMA 211:2135, 1970.
- Kandziora F, Mittlmeier T, Kerschbaumer F: Stage-related surgery for cervical spine instability in rheumatoid arthritis, Eur Spine J 8:371, 1999.
- Karlins NL, Yagan R: Dyspnea and hoarseness: a complication of diffuse idiopathic skeletal hyperostosis, Spine 16:235, 1991.
- Kawaida H, Sakou T, Morizono Y: Vertical settling in rheumatoid arthritis: diagnostic value of the Ranawat and RedlundJohnell methods, Clin Orthop Relat Res 239:128, 1989.
- Kerschbaumer F, Kandziora F, Klein C, et al: Transoral decompression, anterior plate fi xation, and posterior wire fusion for irreducible atlantoaxial kyphosis in rheumatoid arthritis, Spine 25:2708, 2000.
- Kimura I, Oh-Hama M, Shingu H: Cervical myelopathy treated by canal-expansive laminaplasty: computed tomographic and myelographic fi ndings, J Bone Joint Surg 66A:914, 1984.
- Kubota M, Baba I, Sumida T: Myelopathy due to ossifi cation of the ligamentum fl avum of the cervical spine: a report of two cases, Spine 6:553, 1981.
- Kudo H, Iwano K, Yoshizawa H: Cervical cord compression due to extradural granulation tissue in rheumatoid arthritis, J Bone Joint Surg 66B:426, 1984.
- LaChapelle EH: Osteotomy of the lumbar spine for correction of kyphosis in a case of ankylosing spondylarthritis, J Bone Joint Surg 28:851, 1946.
- Law WA: Osteotomy of the spine and the treatment of severe dorsal kyphosis: four cases, Proc R Soc Med 42:594, 1949.
- Law WA: Arthritis: surgical treatment of chronic arthritis. In Carling ER, Ross JP, eds: British surgical practice, surgical progress, London, 1952, Butterworth. Law WA: Surgical treatment of the rheumatic diseases, J Bone Joint Surg 34B:215, 1952.
- Law WA: Lumbar spinal osteotomy, J Bone Joint Surg 41B:270, 1959.
- Law WA: Osteotomy of the spine, J Bone Joint Surg 44A:1199, 1962.
- Law WA: The spine in rheumatoid spondylitis, Clin Orthop Relat Res 36:35, 1964.
- Lichtblau PO, Wilson PD: Possible mechanism of aortic rupture in orthopaedic correction of rheumatoid spondylitis, J Bone Joint Surg 38A:123, 1956.
- Lipson SJ: Rheumatoid arthritis of the cervical spine, Clin Orthop Relat Res 182:143, 1984.
- Lipson SJ: Rheumatoid arthritis in the cervical spine, Clin Orthop Relat Res 239:121, 1989.
- Lipson SJ: Subaxial cervical involvement in rheumatoid arthritis. In The Cervical Spine Research Society, Editorial Committee: The cervical spine, 3rd ed, Philadelphia, 1998, Lippincott-Raven. Lourie H, Stewart WA: Spontaneous atlantoaxial dislocation: a complication of rheumatoid disease, N Engl J Med 265:677, 1961.
- Lunsford LD, Bissonette DJ, Zorub DS: Anterior surgery for
You Might Also Like

