Congenital Kyphosis: Comprehensive Surgical Management and Reconstruction
Key Takeaway
Congenital kyphosis is a severe spinal deformity driven by anomalous vertebral development, primarily failure of formation or segmentation. Because orthotic management is universally ineffective, early surgical intervention is paramount. This guide details the biomechanical rationale, advanced imaging protocols, and step-by-step surgical techniques—ranging from posterior in situ arthrodesis in young children to complex combined anterior-posterior reconstructions in severe or rigid deformities—ensuring optimal neurological and structural outcomes.
INTRODUCTION TO CONGENITAL KYPHOSIS
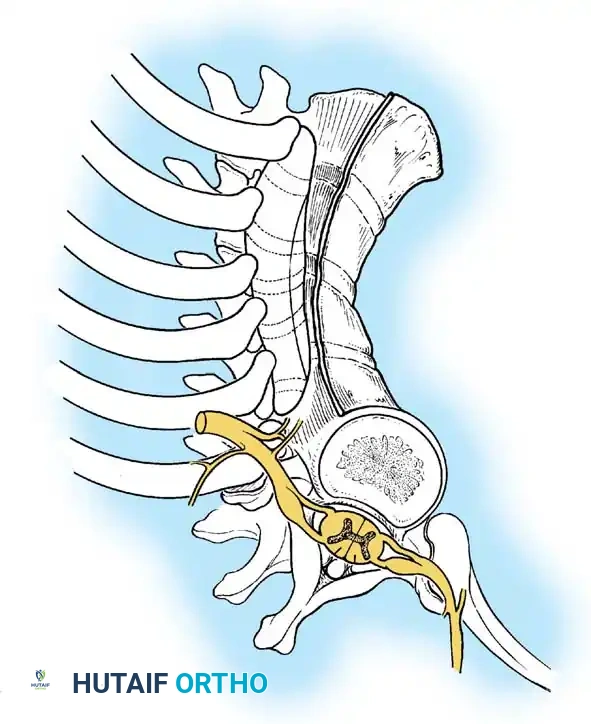
Congenital kyphosis is a rare but potentially devastating spinal deformity resulting from anomalous embryological development of the vertebrae. Unlike adolescent idiopathic scoliosis or Scheuermann's kyphosis, congenital kyphosis is characterized by a relentless, rigid progression that frequently leads to severe sagittal plane decompensation and, critically, neurological compromise.
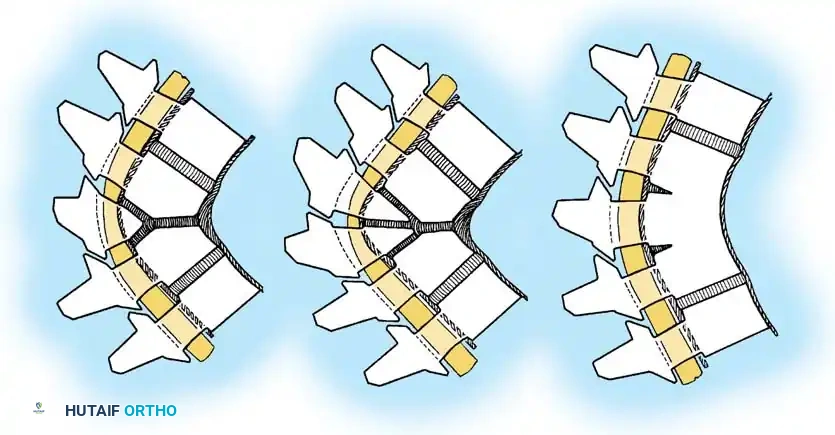
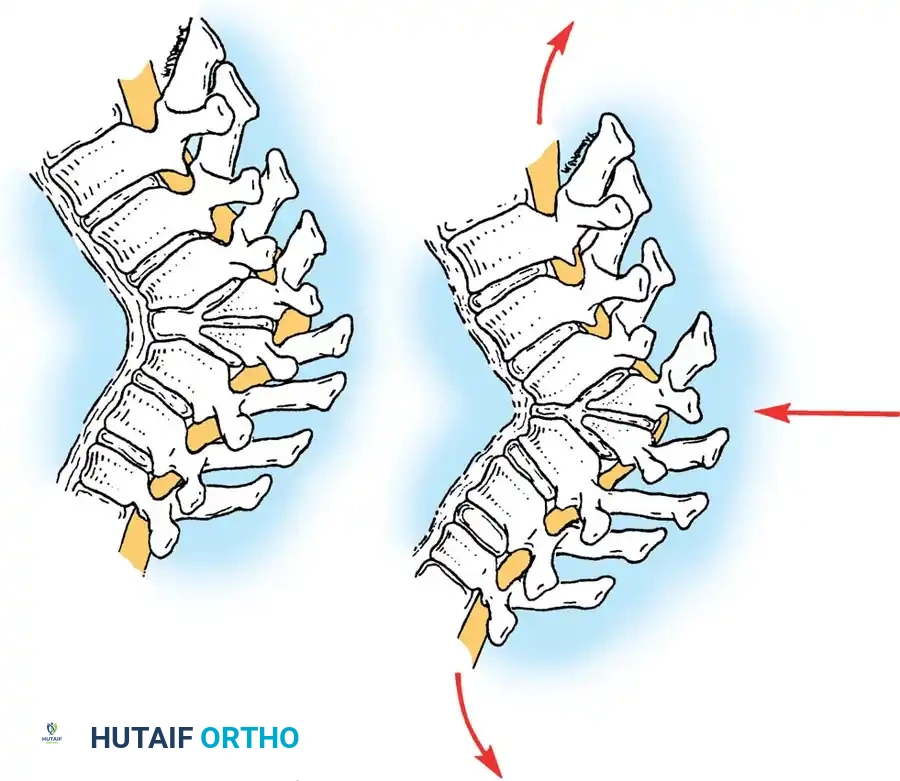
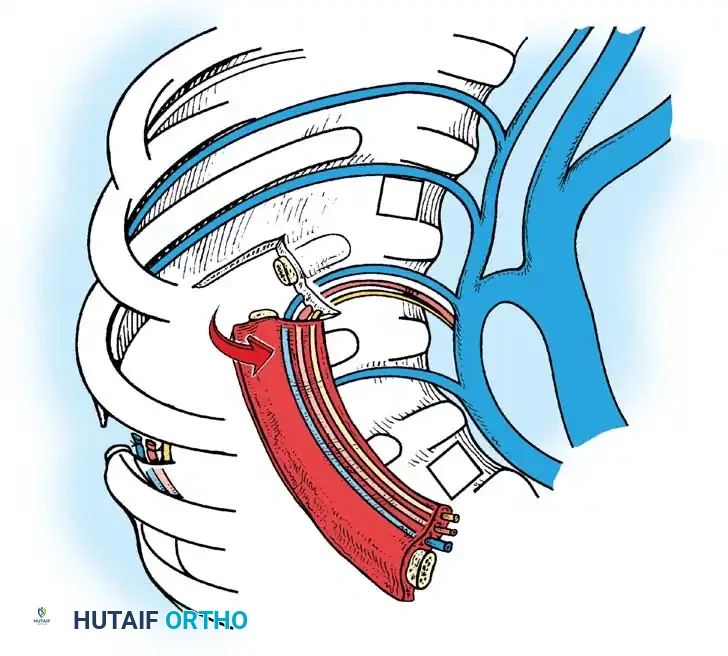
Because the anterior elements of the spine fail to develop or segment normally while the posterior elements continue to grow, the spine is subjected to a biomechanical tethering effect. This creates a sharp, angular deformity that drapes the spinal cord over a bony fulcrum. Orthotic management is universally ineffective; therefore, the cornerstone of management is early recognition and definitive surgical arthrodesis.
CLASSIFICATION OF CONGENITAL KYPHOSIS
The natural history and surgical decision-making for congenital kyphosis rely heavily on the morphological classification originally described by Winter et al., and later refined by McMaster and Singh.
Type I: Failure of Formation
Type I deformities are the most common and carry the highest risk of neurological deficit. They occur predominantly in the thoracic spine and at the thoracolumbar junction, and are exceedingly rare in the cervical spine.
McMaster and Singh further subdivided Type I anomalies based on the specific morphological failure:
* Posterolateral Quadrant Vertebrae
* Posterior Hemivertebrae
* Butterfly (Sagittal Cleft) Vertebrae
* Anterior or Anterolateral Wedged Vertebrae
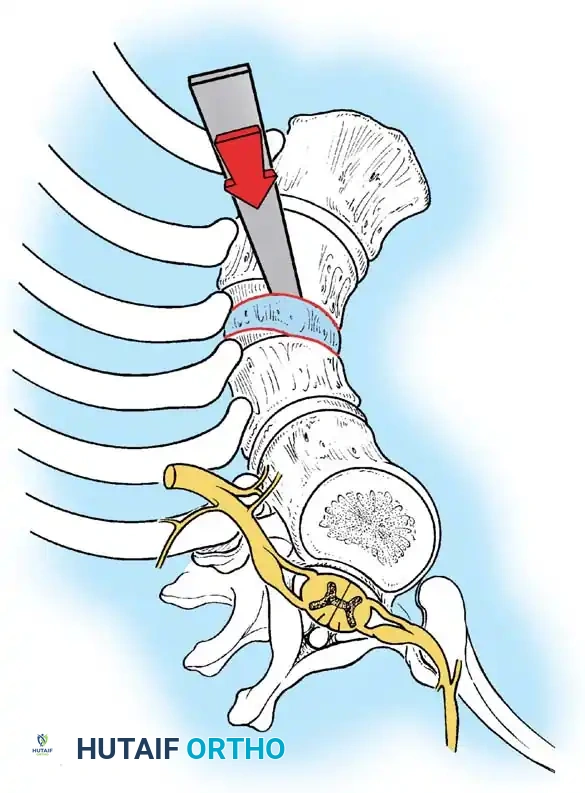
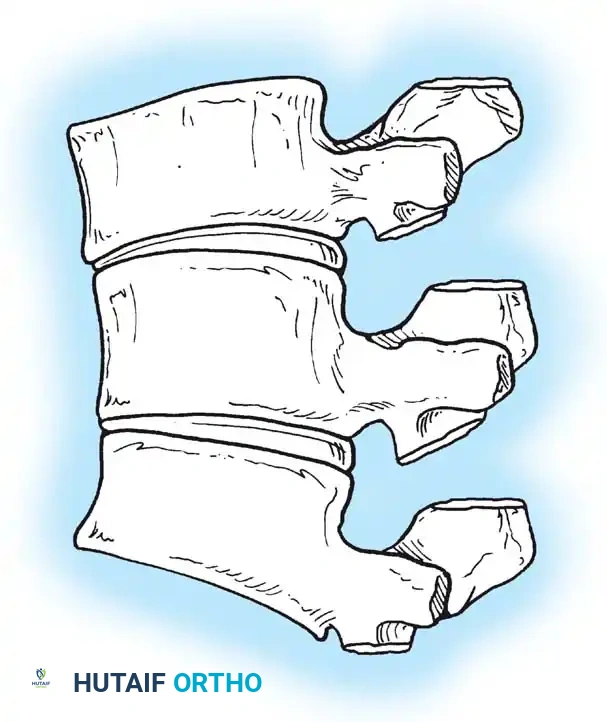
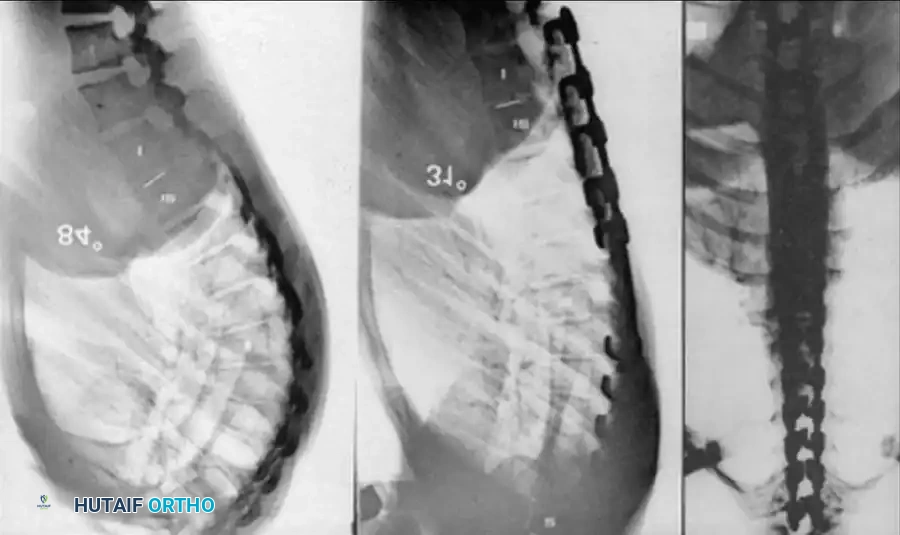
An anterior failure of vertebral body formation produces a sharply angular kyphosis. This sharp apex is highly deforming and neurologically dangerous. Approximately 25% of patients with Type I deformities develop neurological deficits. Deformities in the upper thoracic spine are particularly prone to causing spinal cord compression. Notably, if the apex of the kyphosis is at or caudad to the T12 vertebra, neurological abnormalities are virtually nonexistent due to the presence of the cauda equina rather than the spinal cord.
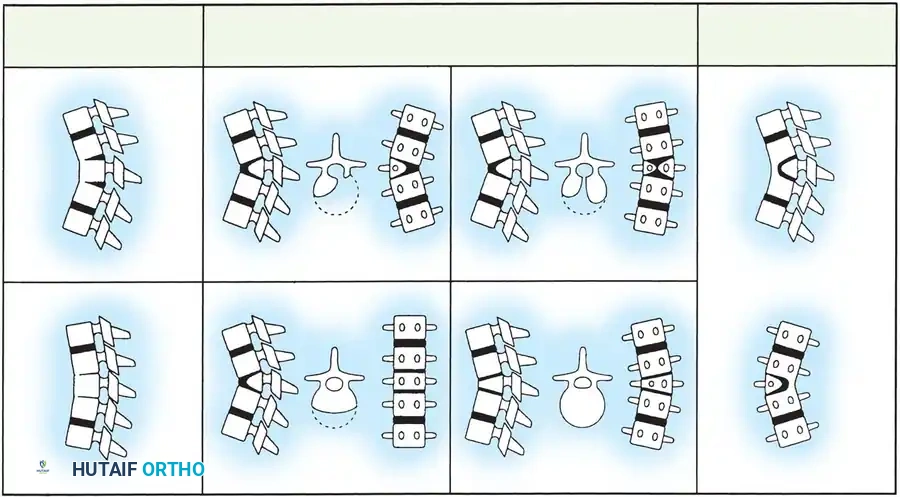
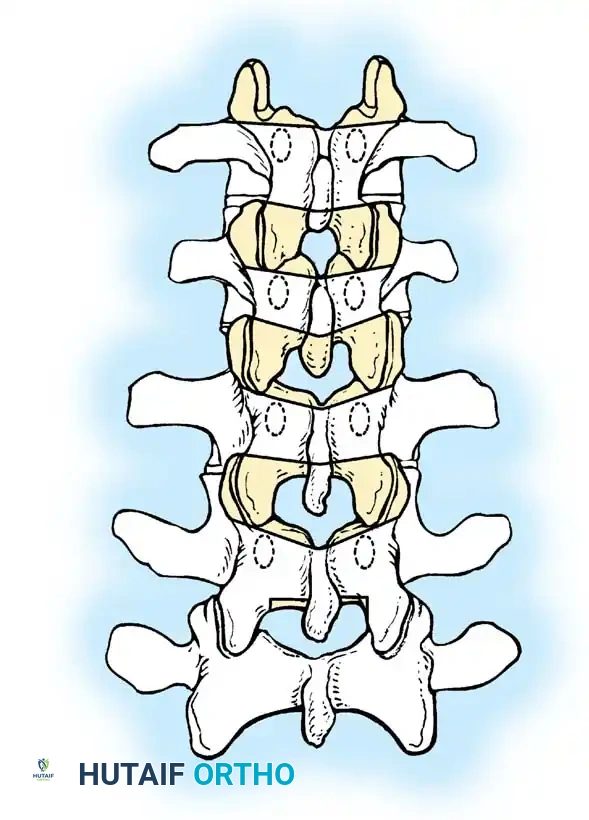
Type II: Failure of Segmentation
Type II deformities are less common and result from an absence of physes and intervertebral discs anteriorly across one or more segments, creating an anterior unsegmented bar.
The severity of the kyphosis is directly proportional to the growth discrepancy between the tethered anterior bar and the normally growing posterior elements. Mayfield et al. demonstrated that these curves progress at an average rate of 5 degrees per year. While they produce a smoother, less angular deformity and are not associated with paraplegia, they cause significant cosmetic deformity and intractable low back pain, warranting early surgical intervention.
Type III: Mixed Anomalies
Type III represents a combination of formation and segmentation failures. According to McMaster and Singh, Type III deformities exhibit the most rapid and relentless progression, followed closely by Type I. Kyphosis caused by two adjacent Type I anomalies progresses significantly faster than a single anomaly.
Clinical Pearl: Type I and Type III congenital kyphosis progress relentlessly during growth, with a marked acceleration during the adolescent growth spurt. Do not wait for skeletal maturity to intervene; early in situ fusion is biomechanically and neurologically protective.
CLINICAL AND RADIOGRAPHIC EVALUATION
Clinical Presentation
Diagnosis is frequently established by a pediatrician, via prenatal ultrasound, or during a newborn clinical examination. Mild deformities may remain occult until the adolescent growth spurt accelerates the curve.
A meticulous neurological examination is mandatory to detect subtle signs of myelopathy, hyperreflexia, or asymmetric motor weakness. Furthermore, congenital spinal anomalies are highly associated with the VACTERL association (Vertebral, Anorectal, Cardiac, Tracheoesophageal, Renal, and Limb anomalies).
* Renal Ultrasonography: Mandatory to rule out unilateral renal agenesis or horseshoe kidney.
* Echocardiography: Required to rule out structural cardiac defects.
* Cervical Spine Radiographs: To rule out Klippel-Feil syndrome.
Advanced Imaging Protocols
High-quality imaging is the foundation of preoperative planning.
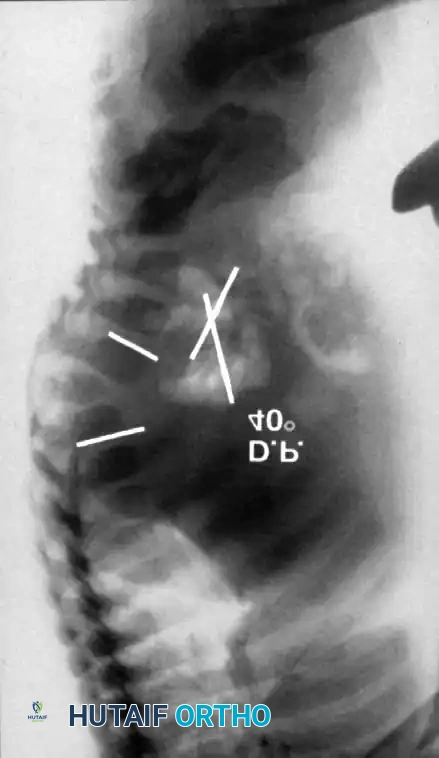
1. Plain Radiographs:
Detailed anteroposterior (AP) and lateral radiographs are essential. Flexion and extension lateral views help determine the rigidity of the kyphosis and identify any compensatory hypermobility or instability in adjacent segments.
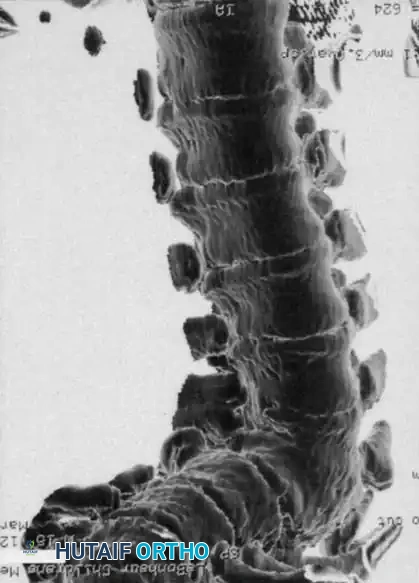
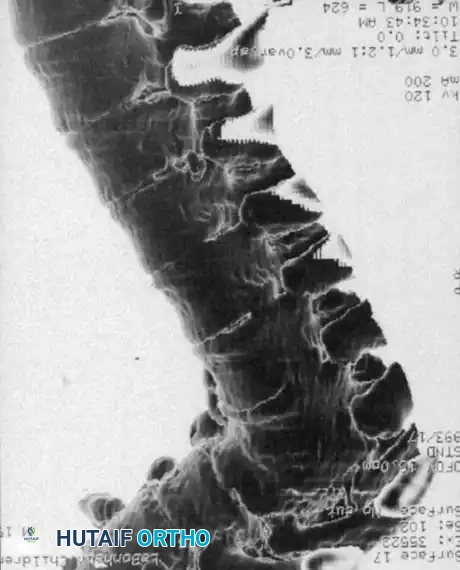
2. Computed Tomography (CT) with 3D Reconstruction:
CT is invaluable for defining the complex bony architecture. It delineates the exact extent of formation/segmentation failure and helps predict the trajectory of the deformity (kyphosis vs. kyphoscoliosis). However, CT cannot assess the growth potential of the cartilaginous anlage.



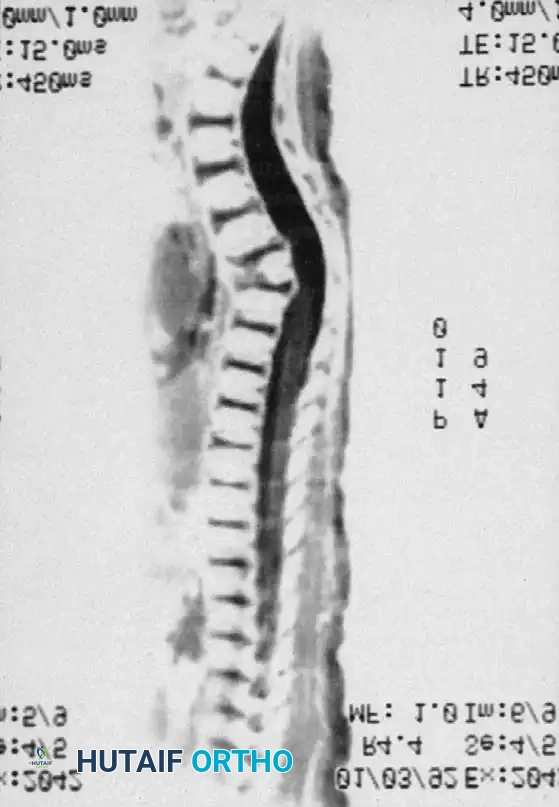
3. Magnetic Resonance Imaging (MRI):
MRI is the gold standard for evaluating the neural elements. It identifies the exact location of the spinal cord relative to the bony apex, highlights areas of cord compression or myelomalacia, and detects associated intraspinal anomalies (e.g., diastematomyelia, tethered cord, syringomyelia). MRI also clearly defines the unossified cartilage anlage in young children.
SURGICAL INDICATIONS AND BIOMECHANICS
Orthotic management (bracing) is completely ineffective for congenital kyphosis and should not be utilized, as it delays definitive treatment and allows the deformity to worsen.
The surgical strategy is dictated by:
1. The type of deformity (Type I, II, or III).
2. The magnitude and angularity of the curve.
3. The age and remaining growth potential of the patient.
4. The presence or absence of neurological deficits.
Surgical Warning: Never use longitudinal traction (e.g., halo-gravity traction) in rigid Type I congenital kyphosis. Traction across a rigid anterior bony fulcrum stretches the spinal cord directly over the apex, carrying an unacceptably high risk of iatrogenic paraplegia.
OPERATIVE TECHNIQUES: STEP-BY-STEP
1. Posterior-Only Arthrodesis (Children < 5 Years)
For young children (under 5 years of age) with a Type I deformity measuring less than 50 degrees, a posterior-only in situ fusion (Moe-type) is the procedure of choice.
Biomechanics: A solid posterior arthrodesis halts posterior growth. If the anterior cartilaginous physes retain growth potential, continued anterior growth against a tethered posterior column can lead to spontaneous, gradual correction of the kyphosis over time.
Surgical Steps:
1. Positioning: Prone on a pediatric Jackson table, ensuring the abdomen is free to reduce venous pressure.
2. Exposure: Subperiosteal dissection is strictly limited to the vertebrae to be fused. The fusion must include the anomalous vertebrae plus one healthy, neutral vertebra proximal and distal to the deformity.
3. Decortication and Grafting: Meticulous decortication of the laminae and facet joints is performed. Autogenous iliac crest bone graft is the gold standard, though structural allograft can supplement if autograft volume is insufficient.
4. Postoperative Protocol: Historically, Winter recommended 4 months of strict bed rest followed by a Risser cast. Modern protocols utilize immediate postoperative custom-molded TLSO casting for 6 to 12 months. If fusion solidity is questionable at 6 months, surgical exploration and regrafting are indicated.

2. Combined Anterior and Posterior Fusion (Children > 5 Years or Curves > 55°)
In children older than 5 years, or in any patient with a curve exceeding 55 degrees, posterior fusion alone is insufficient. The biomechanical forces of a severe curve will overpower a posterior graft, leading to pseudarthrosis and continued progression. A combined anterior release/fusion and posterior instrumented fusion is required.
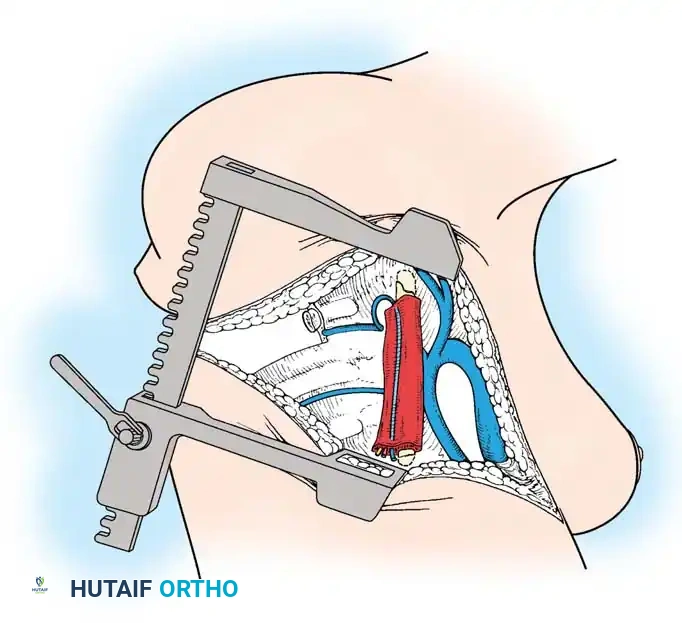
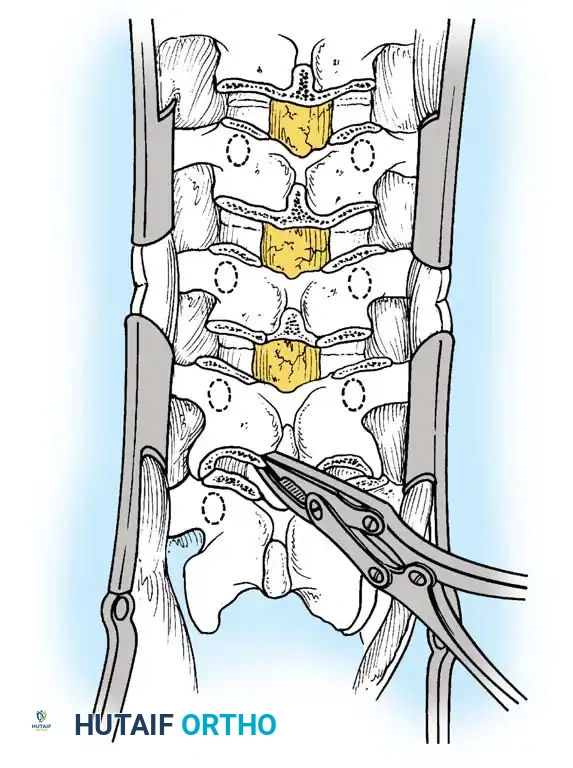
Phase 1: Anterior Approach and Release
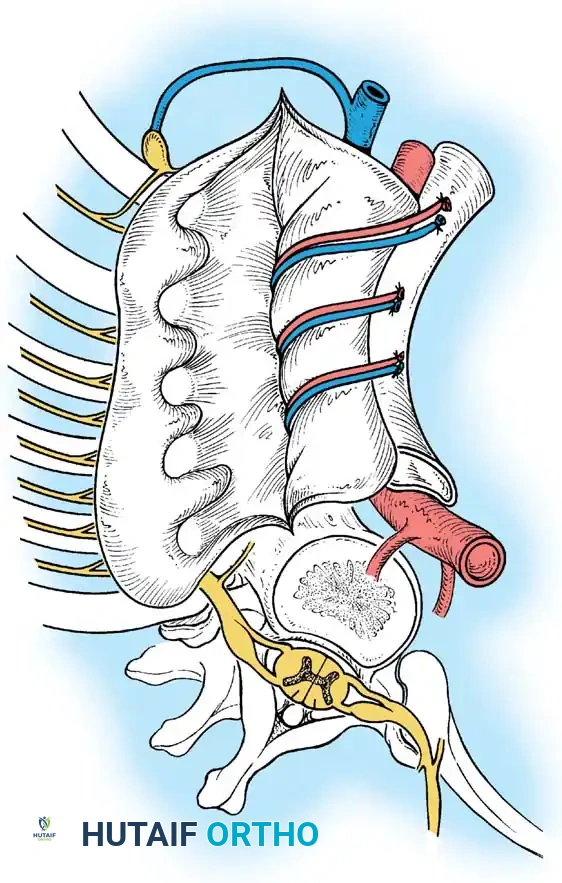
- Approach: A standard thoracotomy or thoracoabdominal approach is utilized, depending on the apex of the curve.
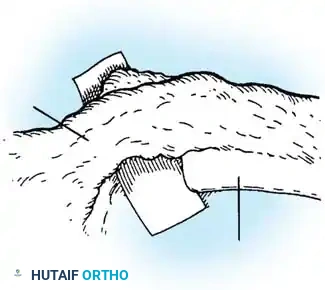
- Release: The shortened anterior longitudinal ligament, fibrotic tissue, and cartilaginous remnants of the anomalous vertebrae are radically excised.
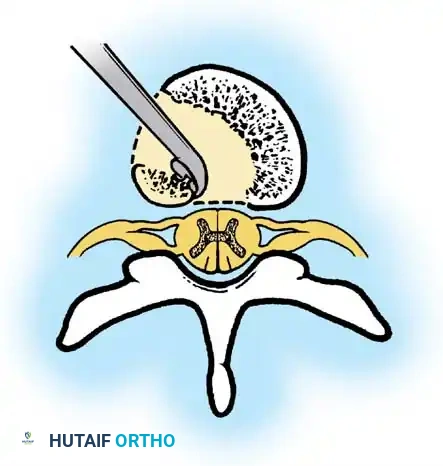
- Decompression (If Indicated): If the patient has a neurological deficit, an anterior corpectomy (vertebrectomy) is performed to decompress the spinal cord at the apex.

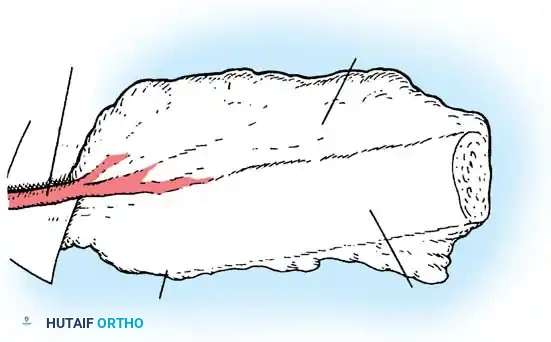
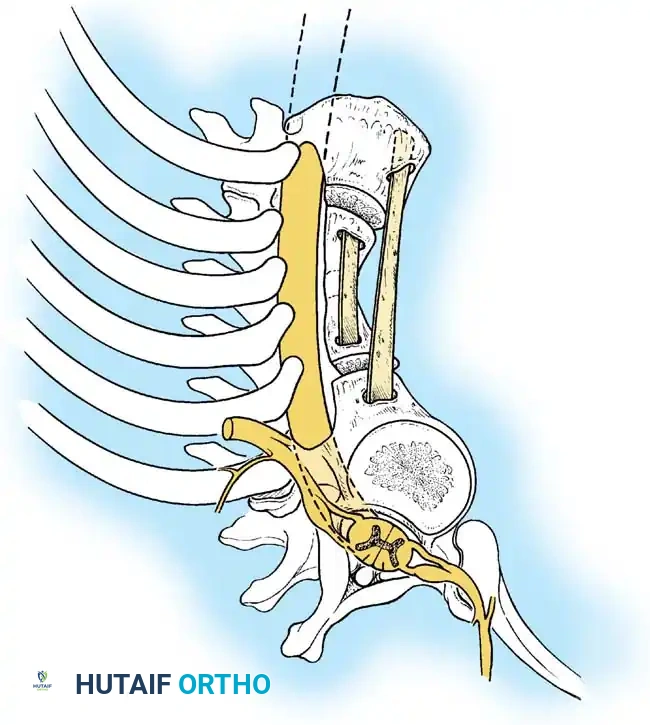
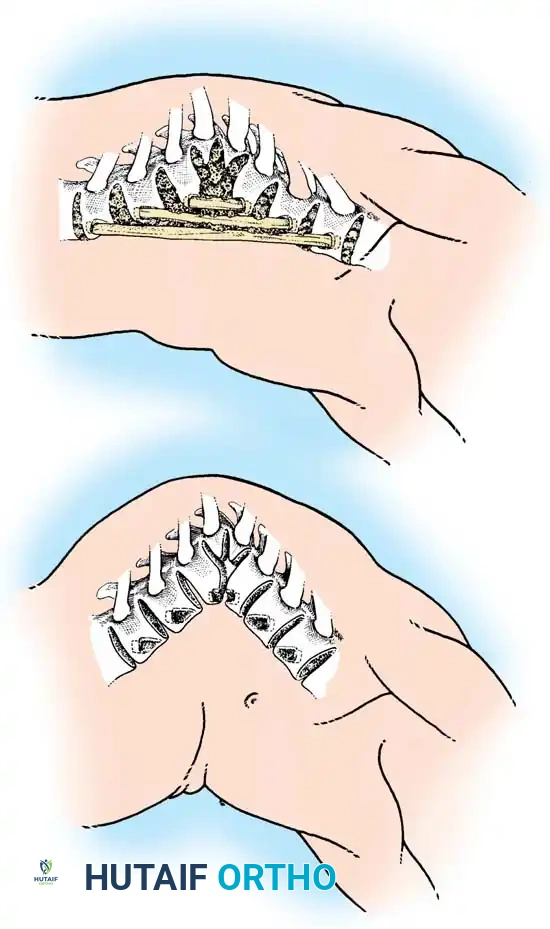
Phase 2: Anterior Strut Grafting
Once the anterior column is mobilized, structural support is mandatory to prevent collapse.
1. Graft Selection: Autogenous rib (harvested during the thoracotomy) or vascularized/non-vascularized fibular strut grafts are utilized.
2. Placement: The strut is keyed into healthy vertebral bodies above and below the apex.
3. Correction: An assistant applies gentle, manual, posteriorly directed pressure over the apex of the deformity while the strut is impacted. No mechanical distraction is used.
4. Packing: Cancellous autograft is packed densely around the strut to promote rapid incorporation.
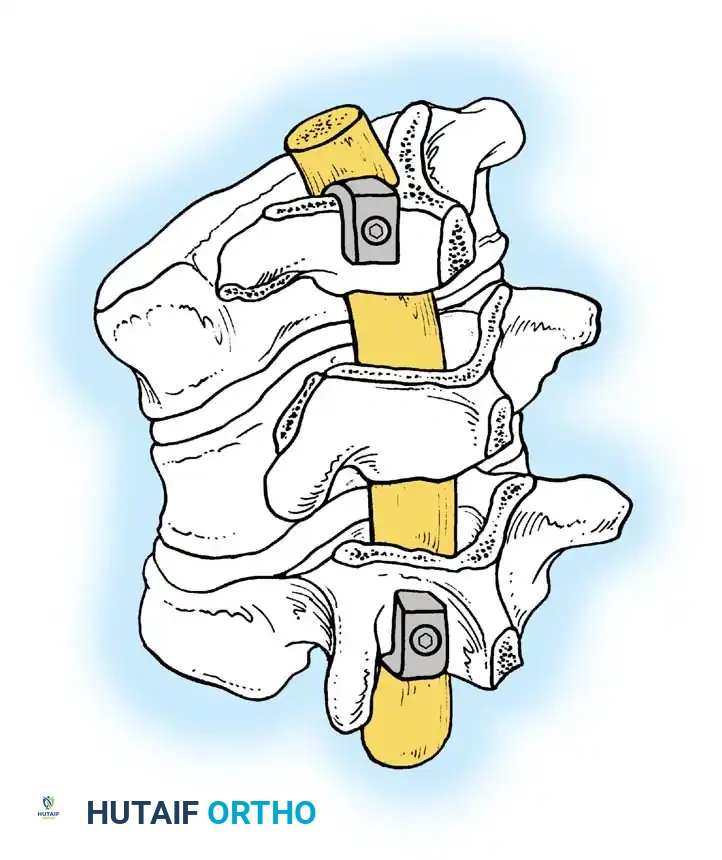
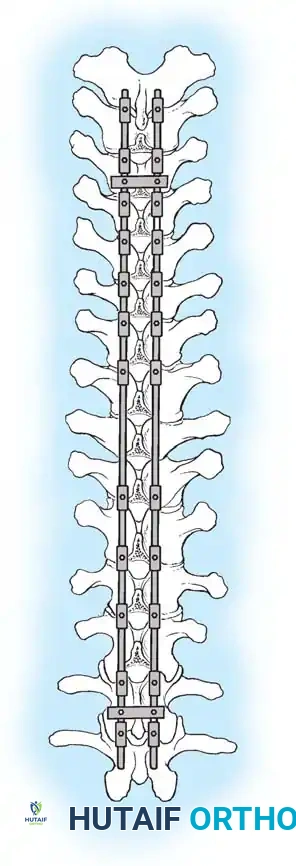
Phase 3: Posterior Instrumented Fusion
The posterior procedure is performed either under the same anesthetic or staged, depending on patient tolerance and blood loss.
1. Instrumentation: Pedicle screws and/or hooks are placed. The posterior construct must be longer than the anterior fusion, typically extending at least one normal vertebra above and below the anterior graft.
2. Correction Mechanics: Only compression forces are applied across the posterior construct to close the posterior elements and hinge on the anterior strut graft. Distraction is strictly contraindicated.
3. Fusion: Copious autograft is applied following meticulous decortication.
3. Posterior Column Shortening and Osteotomies
In older patients or those with rigid, mature deformities, posterior column shortening (e.g., Ponte osteotomies or Smith-Petersen osteotomies) may be required to achieve sagittal balance. While originally popularized for Scheuermann's kyphosis, the biomechanical principles apply to rigid congenital curves undergoing posterior reconstruction.
Technique Principles:
1. Resection: Broad posterior resections of the facet joints, ligamentum flavum, and portions of the lamina are performed at every intersegmental level within the fusion area.
2. Apical Treatment: The apical vertebra is often left uninstrumented to allow for maximal stress distribution.
3. Closure: Correction is achieved by closing the posterior osteotomy gaps using cantilever rod reduction and segmental compression.
The reduction of the kyphosis relies on a fully segmental construct. Transverse connectors are added to maximize torsional rigidity.
Clinical Pearl: When utilizing posterior instrumentation for congenital kyphosis, the primary goal is internal stabilization rather than aggressive correction. Over-correction of a rigid, angular curve carries an unacceptably high risk of spinal cord ischemia and paralysis.
Additional Surgical Considerations and Advanced Techniques
Depending on the complexity of the deformity, additional intraoperative steps may be required to ensure a safe and stable reconstruction.

POSTOPERATIVE PROTOCOLS AND COMPLICATION MANAGEMENT
Neuromonitoring
Continuous intraoperative neurophysiological monitoring, including Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs), is mandatory. If signal degradation occurs during correction, the surgeon must immediately release the corrective forces, increase mean arterial pressure (MAP), and assess for mechanical cord compression.
Postoperative Bracing
If modern, multi-hook or pedicle screw segmental instrumentation is utilized, postoperative external support may not be strictly necessary in older children. However, if pediatric-sized instrumentation is used, or if bone quality is poor, a custom TLSO brace is worn for 6 months to protect the construct until arthrodesis is solid.
Managing Complications
- Pseudarthrosis: The most common mechanical complication, particularly at the thoracolumbar junction. It presents as loss of correction or implant failure. Treatment requires revision surgery, exploration of the fusion mass, aggressive decortication, and re-grafting.
- Neurological Deficit: Delayed neurological deficits can occur due to epidural hematoma or progressive kyphosis from construct failure. Emergent MRI and surgical decompression/revision are required.
- Infection: Managed with aggressive surgical debridement, implant retention (if stable), and culture-directed intravenous antibiotics.
CONCLUSION
Congenital kyphosis is a complex, progressive spinal deformity that demands a high index of suspicion, thorough preoperative imaging, and decisive surgical intervention. By understanding the biomechanical behavior of formation and segmentation failures, the orthopedic surgeon can tailor the operative approach—whether a simple posterior in situ fusion in a toddler or a complex anterior-posterior reconstruction in an adolescent—to halt progression, protect the neural elements, and restore sagittal balance.
📚 Medical References
- Bernard TN, Burke SW, Johnston CE III, et al: Congenital spine deformities: a review of 47 cases, Orthopedics 8:777, 1985.
- Betz RR: Kyphosis of the thoracic and thoracolumbar spine in the pediatric patient: normal sagittal parameters and scope of the problem, Instr Course Lect 53:479, 2004.
- Bjekreim I, Magnaes B, Semb G: Surgical treatment of severe angular kyphosis, Acta Orthop Scand 53:913, 1982.
- Bradford DS: Anterior vascular pedicle bone grafting for the treatment of kyphosis, Spine 5:318, 1980.
- Bradford DS, Ganjavian S, Antonious D, et al: Anterior strutgrafting for the treatment of kyphosis: a review of experience with 48 patients, J Bone Joint Surg 64A:680, 1982.
- Guille JT, Forlin E, Bowen JR: Congenital kyphosis, Orthop Rev Feb:235, 1993.
- James JIP: Paraplegia in congenital kyphoscoliosis, J Bone Joint Surg 57B:261, 1975.
- Lonstein JE, Winter RB, Moe JH, et al: Neurologic defi cit secondary to spinal deformity: a review of the literature and report of 43 cases, Spine 5:331, 1980.
- Lowe TG: Kyphosis of the thoracic and thoracolumbar spine in the pediatric patient: surgical treatment, Instr Course Lect 53:501, 2004.
- Mayfi eld JK, Winter RB, Bradford DS, et al: Congenital kyphosis due to defects of anterior segmentation, J Bone Joint Surg 62A:1291, 1980.
- McMaster MJ, Singh H: Natural history of congenital kyphosis in kyphoscoliosis: a study of 112 patients, J Bone Joint Surg 81A:1367, 1999.
- McMaster MJ, Singh H: The surgical management of congenital kyphosis and kyphoscoliosis, Spine 26:2146, 2001.
- Montgomery SP, Hall JE: Congenital kyphosis, Spine 7:360, 1982.
- Morrin B, Poitras B, Duhaime M, et al: Congenital kyphosis by segmentation defect: etiologic and pathogenic studies, J Pediatr Orthop 5:309, 1985.
- Rose GK, Owen R, Sanderson JM: Transposition of rib with blood supply for the stabilization of spinal kyphosis, J Bone Joint Surg 57B:112, 1975.
- Shaffer JW, Bradford DS: The use of and techniques for vascularized rib pedicle grafts. In Bridwell KH, DeWald RL, eds: The textbook of spinal surgery, 2nd ed, Philadelphia, 1997, Lippincott-Raven. Singh M, Nagrath AR, Maini PS: Changes in trabecular pattern of the upper end of the femur as an index of osteoporosis, J Bone Joint Surg 52A:457, 1970.
- Smith JT, Gollogly S, Dunn HK: Simultaneous anterior-posterior approach through a costotransversectomy for the treatment of congenital kyphosis and acquired kyphoscoliotic deformities, J Bone Joint Surg 87A:2281, 2005.
- White AA III, Panjabi MM: Practical biomechanics of scoliosis and kyphosis. In White AA, Panjabi AA, eds: Clinical biomechanics of the spine, Philadelphia, 1990, JB Lippincott. Winter RB: Congenital kyphoscoliosis with paralysis following hemivertebra excision, Clin Orthop Relat Res 119:116, 1976.
- Winter RB: Congenital spinal deformity: what’s the latest and what’s the best? Spine 14:1406, 1989.
- Winter RB, Moe JH: The results of spinal arthrodesis for congenital spinal deformity in patients younger than 5 years old, J Bone Joint Surg 64A:419, 1982.
- Winter RB, Moe JH, Lonstein JE: The surgical treatment of congenital kyphosis: a review of 94 patients age 5 years or older with 2 years or more follow-up in 77 patients, Spine 10:224, 1985.
- Winter RB, Moe JH, Wang JF: Congenital kyphosis, J Bone Joint Surg 55A:223, 1973.
- Spondylolysis and Spondylolisthesis Ani N, Keppler L, Biscup RS, et al: Reduction of high-grade slips (grades III through V) with VSP instrumentation: report of a series of 41 cases, Spine 16:302, 1991.
- Askar Z, Wardlaw D, Koti M: Scott wiring for direct repair of lumbar spondylolysis, Spine 28:354, 2003.
- Balderston RA, Bradford DS: Technique for achievement and maintenance of reduction for severe spondylolisthesis using spinous process traction wiring and external fi xation of the pelvis, Spine 10:376, 1985.
- Bell DF, Ehrlich MG, Zaleske DJ: Brace treatment for symptomatic spondylolisthesis, Clin Orthop Relat Res 236:192, 1988.
- Beutler WJ, Fredrickson BE, Murtland A, et al: The natural history of spondylolysis and spondylolisthesis: 45-year followup evaluation, Spine 28:1027, 2003.
- Boachie-Adjei O, Do T, Rawlins BA: Partial lumbosacral kyphosis reduction, decompression, and posterior lumbosacral transfi xation in high-grade
You Might Also Like

