Adult Isthmic Spondylolisthesis: A Comprehensive Surgical and Clinical Guide
Key Takeaway
Adult isthmic spondylolisthesis is an acquired condition characterized by a pars interarticularis defect, leading to translational instability. While most adult slips are low-grade and static, progressive disc degeneration and foraminal stenosis often necessitate surgical intervention. This guide details the pathoanatomy, biomechanics, clinical evaluation, and step-by-step surgical management—including decompression and fusion techniques—for optimizing patient outcomes in symptomatic isthmic spondylolisthesis.
Introduction and Epidemiology
Spondylolisthesis is predominantly an acquired condition characterized by the anterior translation of one vertebral body over the adjacent caudal vertebra. While the majority of progressive deformities manifest during childhood and adolescence, deformities in the adult population are typically static and low-grade. Adult patients generally present with two distinct types of spondylolisthesis: isthmic and degenerative. Each variant possesses a unique etiology, pathoanatomy, and natural history, dictating specific therapeutic algorithms.
Isthmic spondylolisthesis is notably absent in newborns but develops throughout childhood, reaching an adult prevalence of 5% to 8% by the age of 18 years. The biomechanical demands of upright walking and associated axial weight-bearing are absolute prerequisites for its development; notably, this disorder has never been reported in nonambulatory patients.
Men are affected twice as frequently as women. Risk factors for the development of isthmic spondylolisthesis are strongly correlated with activities that subject the lumbar spine to repetitive hyperextension, excessive lordosis, or hyperflexion. High-risk athletics include gymnastics, football, pole-vaulting, weight lifting, dancing, and volleyball. Furthermore, individuals engaged in highly active vocations, particularly military recruits, demonstrate a significantly higher incidence of symptomatic or asymptomatic pars interarticularis fractures. Epidemiological studies have reported pars defects in up to 9.7% of screened military personnel. A genetic predisposition is also strongly suspected, as familial clustering of the condition is well-documented.
Pathoanatomy and Structural Failure
In the adult population, isthmic spondylolisthesis is generally nonprogressive; however, the clinical sequelae of back pain and radiculopathy are highly prevalent. The anatomical distribution of isthmic spondylolisthesis is highly specific: it affects the L5 vertebral level in 89% of patients, L4 in 11%, and L3 in 3%.
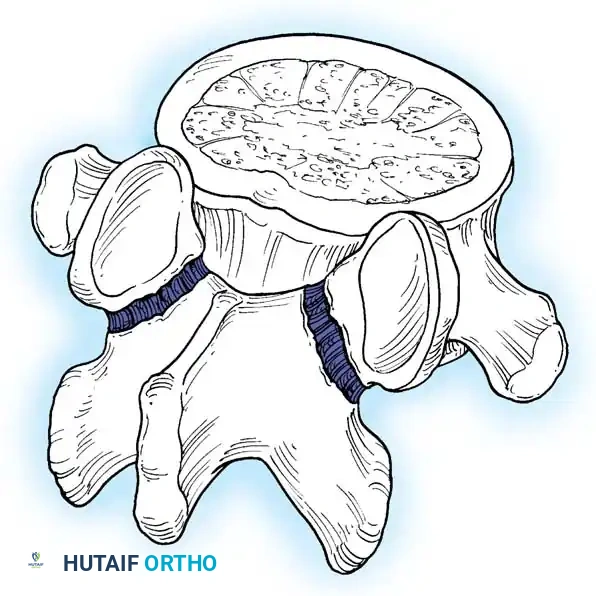
In adults, the degree of anterior translation (slip) is typically less than 50% (Grade I or II). This mechanical fault invariably leads to accelerated degeneration of the intervertebral disc at the level of the pars defect. The fundamental anatomical failure occurs at the pars interarticularis, which disrupts the integrity of the "bony hook" of the affected spinal motion segment.
The bony hook is a critical stabilizing structure consisting of the pedicle, the pars interarticularis, and the inferior articular facet of the cephalad segment, articulating with the superior articular facet of the caudal segment. When a spondylolytic defect occurs, this structural linkage is compromised and can no longer resist anterior translational shear forces. Consequently, the posterior elements separate through the pars fracture—leaving the facet joints anatomically located—while the entire trunk and anterior vertebral column translate anteriorly over the sacrum.
Clinical Pearl: In severe, high-grade slips (which are rare in adults), global sagittal balance is profoundly affected due to the anterior shift of the body’s center of gravity, leading to compensatory hyperlordosis of the adjacent segments and pelvic retroversion.
The Role of Dysplasia
Abnormal local anatomy, such as congenital dysplasia, strongly predisposes a segment to progressive spondylolisthesis. Defects such as spina bifida occulta and dysplastic facet joints further compromise the bony hook, diminishing the segment's innate resistance to shear forces. According to the Marchetti and Bartolozzi classification, dysplasia is categorized into high and low grades. Untreated high dysplasia carries a high incidence of progression but is rare in adults. Low dysplasia, often featuring spina bifida occulta, is more common, rarely progresses, and is typically an incidental finding in the adult demographic.
Biomechanics of Instability
Recreating the exact biomechanics of spondylolisthesis in a laboratory setting has proven complex. In vitro division of the pars interarticularis results in significant motion in the axial and coronal planes, yet pure translational instability does not spontaneously occur. Biomechanical data strongly suggest that repetitive rotational forces, rather than pure extension forces, are the primary instigators of pars fractures.
The inability to perfectly recreate spondylolisthesis via isolated pars osteotomies indicates that the pars fracture is not the sole etiology of translational instability. Grobler et al. demonstrated that further sectioning of the iliolumbar ligaments did not independently create translation. However, when comparing a normal spine to one with simulated defects, Grobler et al. revealed that pars defects at L4-L5 resulted in 12% more rotation, 33% more shear translation, and 43% more axial translation compared to identical defects at L5-S1.
This biomechanical discrepancy explains why L4-L5 isthmic spondylolisthesis, though less common, is inherently more unstable and prone to progression than L5-S1 slips. The iliolumbar ligaments provide substantial tethering stability to the L5 vertebra, anchoring it to the pelvis, a protection lacking at the L4 level.
Natural History and Disease Progression
While adolescent patients are at a higher risk for slip progression, adults generally experience a static deformity. Slips exceeding 50% are exceedingly rare in the adult population. Consequently, adult patients are treated therapeutically once pain or neurological deficits develop, rather than prophylactically as is common in pediatric orthopedics.
Surgical Warning: Postoperative progression of spondylolisthesis is a critical iatrogenic complication. Laminectomy or combined bilateral resection of more than one facet in the presence of a pars fracture removes the remaining posterior tension band, precipitating rapid translational instability. Such decompressive procedures are a strict relative indication for concomitant spinal fusion.
Haraldsson and Willner’s comparative study highlighted that only 2 out of 20 adults (older than 25 years) experienced slip progression, and notably, both instances occurred following isolated laminectomies.
Progressive disc degeneration is the hallmark of adult isthmic spondylolisthesis. Floman documented slip progression from 9% to 30% over a mean of 6.8 years in adult patients presenting with incapacitating lumbar back pain. This progression typically commenced after age 30 and correlated directly with marked disc degeneration. As the disc collapses, shear stresses increase; 100% of body weight creates an anteriorly directed force across the disc space, compared to 80% when intact facets share the axial load.
Clinical Evaluation
Adult patients predominantly present with insidious, deep, aching distal lumbar pain. Wiltse reported that 11% of patients presenting with distal back pain harbor pars defects. While back pain is reported in up to 91% of symptomatic patients, spondylolysis itself does not inherently predispose individuals to greater overall disability than the general population unless complicated by nerve root compression or severe discogenic collapse.
History and Physical Examination
Pain localized to the distal lumbar spine that exacerbates with extension is the classic hallmark of posterior element (facet or pars) pathology. Conversely, pain exacerbated by flexion or prolonged sitting is typically discogenic.
Clinical Pearl: Pain that is reliably alleviated by walking uphill, resting on a grocery cart, or pushing a lawnmower (activities that induce lumbar flexion) strongly indicates posterior element pathology and secondary foraminal stenosis.
Physical examination may reveal:
* Palpable Step-off: Present in up to 42% of patients, typically felt at the spinous process of the level above the slip (e.g., an L4 spinous process step-off in an L5-S1 slip, as the L5 posterior arch remains behind).
* Hamstring Spasm (Phalen-Dickson Sign): Present in 27% of patients, causing a characteristic crouched, knee-flexed gait and flattening of the lumbar lordosis.
* Tension Signs: Present in 19% of patients, helping differentiate true radiculopathy from referred mechanical pain.
Sciatica in adults with isthmic spondylolisthesis is almost exclusively caused by foraminal stenosis compressing the exiting nerve root (the L5 root in an L5-S1 slip). As the disc collapses and the vertebral body translates anteriorly, the pars defect fills with fibrocartilaginous hypertrophic tissue (a failed nonunion response). This tissue, combined with a buckling ligamentum flavum and a bulging disc, severely tethers and compresses the nerve root within the neuroforamen.
Symptoms of neurogenic claudication caused by central spinal stenosis are distinctly uncommon in isthmic spondylolisthesis. The bilateral pars defects effectively "auto-decompress" the central canal by allowing the posterior elements to float posteriorly as the vertebral body slips anteriorly. If central claudication is present, alternative sources of neural compression must be aggressively investigated.
Diagnostic Imaging
Radiography
Standing anteroposterior (AP) and lateral radiographs are the foundational diagnostic modalities.

- Standing Lateral View: Essential for loading the disc and revealing the true extent of translational instability. Lowe et al. demonstrated that in 26% of patients, translation was visible only on standing films and reduced completely when supine.
- AP View: May reveal a lucency at the pars, reactive sclerosis contralateral to a unilateral defect, or the classic "Napoleon’s hat" sign in high-grade slips (the L5 body viewed end-on as it drops anterior to the sacrum).
- Oblique Views: Historically utilized to visualize the "Scotty dog" profile, where a radiolucent gap in the dog's neck represents the pars fracture. Oblique views can identify up to 19% of pars fractures missed on standard AP/Lateral films.
- Ferguson View: A modified pelvic outlet view (30-degree cephalad tilt focused on the L5-S1 disc) is invaluable for preoperative assessment of the L5 transverse processes, L5-S1 disc space, and sacral ala.
- Flexion-Extension Views: Critical for identifying dynamic hypermobility and preoperative surgical planning.
Magnetic Resonance Imaging (MRI)
MRI is the gold standard noninvasive screening tool for evaluating neural element compression and disc desiccation.
* Sagittal T1/T2 Images: Delineate disc hydration, Modic endplate changes, and the dimensions of the spinal canal. A normal adult disc appears hyperintense (white) on T2-weighted images with a slight central cleft. Loss of this signal indicates desiccation.
* Parasagittal Sequences: Provide exquisite detail of the neural foramen. In isthmic spondylolisthesis, horizontalization of the facet and diminished perineural fat often obscure the nerve root. A distinct area of low signal intensity within the foramen correlates surgically with the fibrocartilaginous nonunion mass and hypertrophic ligament compressing the exiting root.
Surgical Management: Indications and Principles
The primary goal of surgical intervention in adult isthmic spondylolisthesis is the alleviation of radicular pain and the stabilization of the motion segment, rather than the anatomical reduction of the slip itself.
Indications for Surgery:
1. Intractable back or leg pain unresponsive to a minimum of 6 months of comprehensive conservative management (physical therapy, NSAIDs, epidural steroid injections).
2. Progressive neurological deficit (motor weakness, sensory loss).
3. Iatrogenic instability following previous decompressive surgery.
Step-by-Step Surgical Approaches
1. Patient Positioning and Preparation
The patient is typically positioned prone on a radiolucent Jackson spinal table. This positioning allows the abdomen to hang free, reducing intra-abdominal pressure and minimizing epidural venous bleeding. Careful padding of all bony prominences is mandatory. Fluoroscopy is utilized to localize the exact operative level prior to incision.
2. Posterior Decompression and Posterolateral Fusion (PLF)
Historically, the Gill procedure involved the isolated removal of the loose posterior lamina (the "Gill fragment"). However, due to the high risk of iatrogenic instability, this is now universally combined with instrumented fusion.

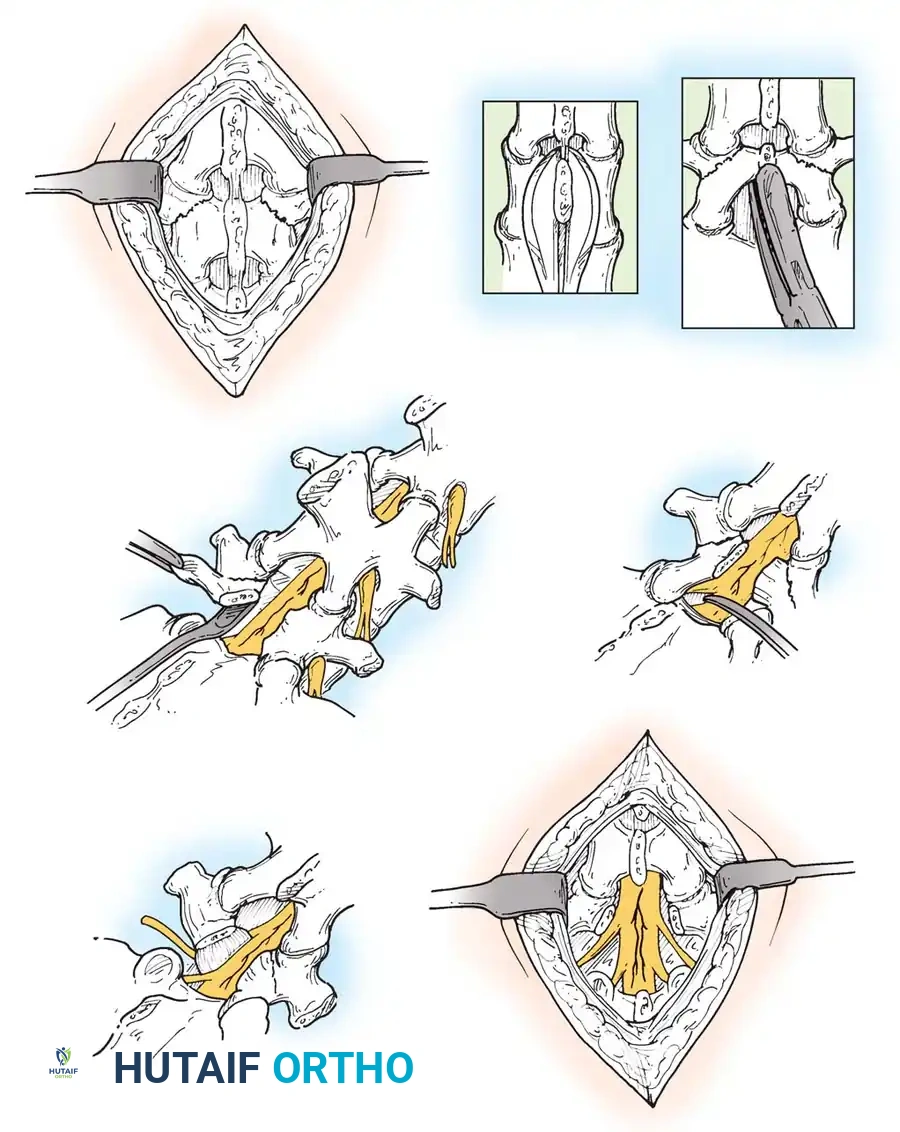
- Exposure: A standard midline incision is made. Subperiosteal dissection exposes the spinous processes, laminae, pars defects, and transverse processes of the affected levels.
- Decompression: The loose lamina and spinous process are carefully excised. The fibrocartilaginous mass at the pars defect is meticulously resected using Kerrison rongeurs to decompress the exiting nerve root (e.g., L5 root) throughout its course in the neuroforamen.
- Instrumentation: Pedicle screws are placed under fluoroscopic or navigation guidance. The trajectory must account for the altered anatomy; the L5 pedicle in isthmic spondylolisthesis is often dysplastic and sclerotic.
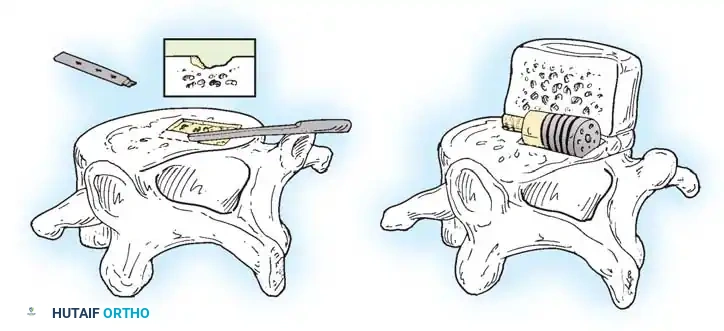
- Grafting: The transverse processes and lateral gutters are decorticated with a high-speed burr. Autologous local bone graft, supplemented with allograft or orthobiologics, is packed into the posterolateral gutters to facilitate fusion.
3. Transforaminal / Posterior Lumbar Interbody Fusion (TLIF/PLIF)
When severe disc collapse and foraminal stenosis are present, an interbody fusion is highly advantageous. It restores disc height, indirectly decompresses the neuroforamen, and provides a massive surface area for fusion under compressive loading.
- Facetectomy: A unilateral (TLIF) or bilateral (PLIF) facetectomy is performed to gain access to the disc space while minimizing neural retraction.
- Discectomy and Endplate Preparation: A thorough annulotomy is performed. The disc material is evacuated using pituitary rongeurs and curettes. The cartilaginous endplates are scraped to expose bleeding subchondral bone, ensuring a robust fusion bed.
- Cage Insertion: An interbody cage, packed with bone graft, is impacted into the disc space. This maneuver restores foraminal height and tension on the annulus, often achieving partial reduction of the slip.
4. Anterior Lumbar Interbody Fusion (ALIF)
ALIF is an excellent option for L5-S1 isthmic spondylolisthesis. It allows for aggressive disc clearance, placement of a large lordotic footprint cage, and avoids the posterior musculature entirely.
- Approach: A retroperitoneal approach is utilized, often with the assistance of an access surgeon. The great vessels (aorta, IVC, iliac bifurcations) are carefully mobilized.
- Release and Grafting: The anterior annulus is incised. Complete discectomy is performed. The anterior approach allows for a powerful release of the contracted anterior structures, facilitating significant reduction of the slip when the interbody device is inserted. ALIF is typically supplemented with posterior percutaneous pedicle screws for rigid biomechanical stability.
5. Management of High-Grade Slips: In Situ Fusion
In the rare adult presenting with a high-grade slip (Grade III or IV), aggressive reduction maneuvers carry an unacceptably high risk of L5 nerve root stretch injury (neurapraxia). In these scenarios, an in situ fusion is preferred.
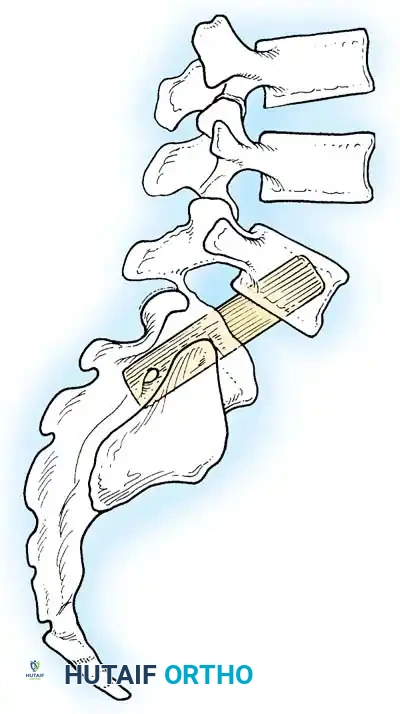
- Bohlman Technique: This technique involves a posterior decompression combined with a transsacral transvertebral fibular dowel graft.
- A trajectory is drilled from the posterior aspect of the S1 vertebral body, traversing the S1 endplate, across the disc space, and into the anteriorly translated L5 vertebral body.
- A structural fibular allograft or titanium dowel is impacted across this trajectory, effectively locking the L5 vertebra to the sacrum in its current position, preventing further shear while avoiding the neurological risks of reduction.
Postoperative Protocols and Rehabilitation
Successful surgical management of adult isthmic spondylolisthesis relies heavily on structured postoperative rehabilitation.
- Phase 1 (0-6 Weeks): Focus on wound healing and early mobilization. Patients are encouraged to walk daily. Bending, lifting (greater than 10 lbs), and twisting (BLT) are strictly prohibited. A rigid lumbosacral orthosis (LSO) may be utilized depending on bone quality and construct rigidity.
- Phase 2 (6-12 Weeks): Initiation of formal physical therapy. Focus shifts to isometric core strengthening, pelvic tilts, and gentle hamstring stretching. Radiographs are obtained at 6 and 12 weeks to assess hardware integrity and early fusion mass consolidation.
- Phase 3 (3-6 Months): Progression to dynamic core stabilization and functional restoration. Return to light manual labor or non-contact sports is generally permitted at 4 to 6 months, provided radiographic evidence of fusion is present and the patient is neurologically intact and pain-free. Heavy labor and high-impact activities are typically restricted until 9 to 12 months postoperatively.
📚 Medical References
You Might Also Like