Proximal Interphalangeal Joint Capsulotomy: Comprehensive Surgical Guide
Key Takeaway
Proximal interphalangeal (PIP) joint capsulotomy is a precise surgical intervention indicated for severe, refractory joint stiffness where articular cartilage remains intact. This procedure addresses yielding surrounding tissues, extensor tendon adhesions, and collateral ligament contractures. Success relies on meticulous stepwise release of the collateral ligaments, volar plate checkreins, and contracted soft tissues, ideally performed under regional anesthesia to allow intraoperative assessment of active motion.
INTRODUCTION TO PROXIMAL INTERPHALANGEAL JOINT STIFFNESS
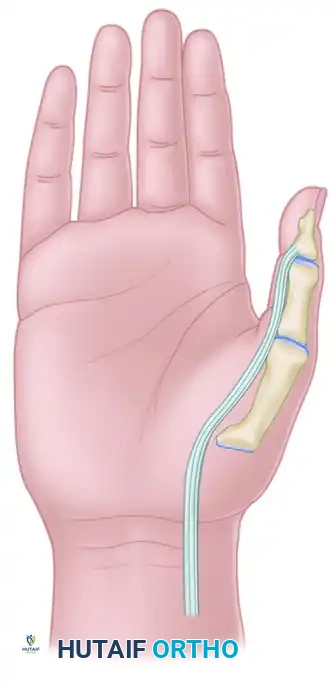
The proximal interphalangeal (PIP) joint is the functional epicenter of the digital ray, accounting for approximately 85% of the total flexion arc of the finger. Because of its complex capsuloligamentous anatomy and its close relationship with the flexor and extensor mechanisms, the PIP joint is notoriously prone to severe, refractory stiffness following trauma, infection, or prolonged immobilization.
Proximal interphalangeal joint capsulotomy is a highly specialized, salvage-level soft-tissue reconstruction. It is indicated strictly when the surrounding tissues are yielding, the articular surface integrity has been radiographically and clinically maintained, and the primary offenders to motion limitation are isolated to extensor tendon adhesions, dorsal capsular tightness, and collateral ligament contractures.
Surgical Warning: Capsulotomy is contraindicated in the presence of severe articular destruction, advanced osteoarthritis, or unyielding bony ankylosis. In such cases, arthroplasty or arthrodesis must be considered.
BIOMECHANICS AND PATHOANATOMY
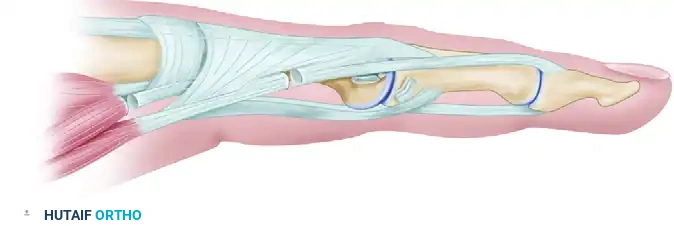
Understanding the kinematics of the PIP joint is paramount before undertaking a capsular release. The PIP joint is a ginglymus (hinge) joint with a bicondylar proximal phalangeal head articulating with the biconcave base of the middle phalanx.
Stability and motion are dictated by a delicate balance of structures:
* Proper Collateral Ligaments (PCL): Originating from the lateral condyles of the proximal phalanx and inserting into the volar-lateral base of the middle phalanx. They are maximally taut in flexion and lax in extension.
* Accessory Collateral Ligaments (ACL): Volar to the PCL, inserting into the volar plate. They are taut in extension.
* Volar Plate: A thick fibrocartilaginous structure that prevents hyperextension.
* Checkrein Ligaments: As described by Watson, Light, and Johnson, these are robust ligamentous structures consisting of fibers from the dorsal portion of the flexor sheath and reflections of the accessory ligament. They extend from thick attachments along the proximal edge of the volar plate and diverge to insert separately along the volar-lateral periosteum of the proximal phalanx.
When the PIP joint is immobilized in flexion, the proper collateral ligaments shorten, and the checkrein ligaments contract, leading to a fixed flexion deformity. Conversely, immobilization in extension leads to shortening of the collateral ligaments in their lax position, preventing subsequent flexion.
ETIOLOGY OF MOTION LIMITATION (THE CURTIS CLASSIFICATION)
Before proceeding to surgery, the exact anatomical structures restricting motion must be systematically identified. Curtis outlined a comprehensive list of causes for limited motion in the PIP joint. These causes must be carefully considered and, except for those involving the collateral ligaments, systematically eliminated or addressed prior to or during the capsulotomy.
Conditions Limiting Flexion
Flexion of the PIP joint may be blocked by dorsal or lateral pathology:
* Skin Contracture: Scarring or contracture of the skin on the dorsum of the finger.
* Extensor Mechanism: Contracture of the long extensor muscle or adherence of the extensor tendon to the proximal phalanx.
* Intrinsic Tightness: Contracture of the interosseous muscle or adherence of its tendon (positive Bunnell test).
* Capsular Contracture: Contracture of the capsular ligament, specifically the proper collateral ligament, which fails to elongate to allow the proximal phalanx condyles to glide.
* Osseous Pathology: Bony block or dorsal exostosis.
Conditions Limiting Extension
Extension of the PIP joint is typically blocked by volar pathology:
* Skin Scarring: Contracture of the skin on the volar surface of the digit.
* Fascial Contracture: Contracture of the superficial fascia within the digit (e.g., Dupuytren's disease).
* Sheath Contracture: Contracture of the flexor tendon sheath within the digit.
* Flexor Mechanism: Contracture of the flexor muscle or adherence of the flexor tendon.
* Volar Plate Contracture: Shortening and fibrosis of the volar plate of the capsular ligament.
* Collateral Ligament Adherence: Adherence of the collateral ligament with the finger in the flexed position.
* Osseous Pathology: Volar bony block or exostosis.
PREOPERATIVE PLANNING AND ANESTHESIA
The Awake Patient Concept
Ideally, a PIP joint capsulotomy is performed with the patient awake and sedated. This allows the patient to actively move the fingers upon command, enabling the surgeon to observe real-time improvement in motion during the sequential release of structures.
To achieve this, proper sedation combined with a regional block at the wrist (e.g., median and ulnar nerve blocks) or a more distal digital block is utilized. The Wide Awake Local Anesthesia No Tourniquet (WALANT) technique using lidocaine with epinephrine has revolutionized this procedure, providing a bloodless field while maintaining full active motor function of the extrinsic flexors and extensors.
Staging the Reconstruction
When a PIP joint is stiff and volar structures are concomitantly suspected of limiting motion either actively (such as flexor tendon adhesions) or passively, the surgical reconstruction must be staged.
1. Stage One: Passive flexion and extension are achieved first through capsulotomy and release of passive restraints.
2. Stage Two: If active flexion remains limited due to flexor tendon adherence in the palm or digit, a flexor tenolysis is performed as a second-stage procedure, typically 10 to 12 weeks later, once the soft tissue envelope has healed and passive motion is maintained through therapy.
Clinical Pearl: Never attempt a simultaneous aggressive capsulotomy and a complex flexor tenolysis in a single setting. The resulting inflammatory response and scar formation will almost certainly lead to recurrent, intractable stiffness.
SURGICAL TECHNIQUE: THE CURTIS CAPSULOTOMY
The following step-by-step technique is based on the foundational principles described by Curtis, incorporating modern understandings of the volar checkrein ligaments.
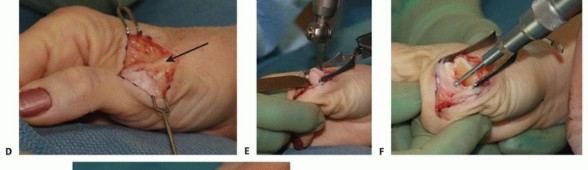
1. Surgical Approach and Exposure
Approach the interphalangeal joint through either a midlateral incision or a curved dorsal incision. The midlateral approach is often preferred as it remains in the neutral axis of the digit, minimizing scar contracture that could limit flexion or extension.
On the selected side, deepen the incision through the subcutaneous tissue. Carefully dissect to expose the transverse retinacular ligament. This structure must be identified and preserved, as it plays a crucial role in stabilizing the lateral bands of the extensor mechanism.
2. Elevation of the Transverse Retinacular Ligament
Expose the collateral ligament by approaching the joint from the base of the middle phalanx. Carefully elevate the transverse retinacular ligament from its underlying attachments.

Preserve this ligament meticulously; it will require precise repair at the conclusion of the capsulotomy to prevent dorsal subluxation of the lateral bands (which would result in a swan-neck deformity).
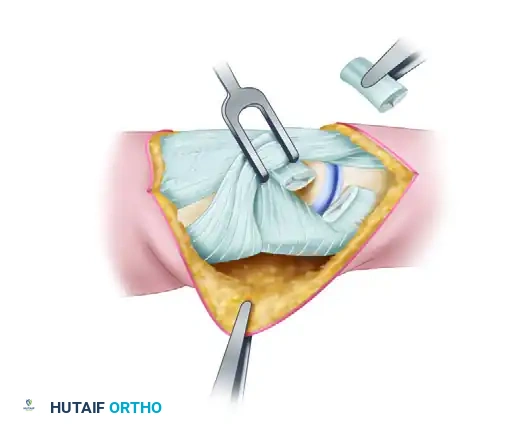
3. Excision of the Collateral Ligament
Once the collateral ligament complex is fully visualized, identify the thick, cord-like proper collateral ligament. Starting at its distal attachment on the base of the middle phalanx, excise en bloc as much of the cord portion of the collateral ligament as possible.
Repeat this exact procedure on the opposite side of the joint. It is critical to remove the ligamentous tissue rather than simply transecting it, as simple release often leads to rapid bridging scar formation and recurrent stiffness.
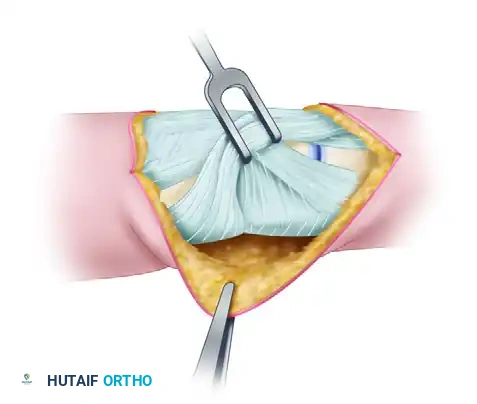
4. Restoration of the Volar Synovial Pouch
In cases where the joint contracture is of long duration, the volar synovial pouch (the recess between the volar plate and the proximal phalanx) may have been completely obliterated by dense adhesions.
If obliterated, the pouch must be restored. Introduce a small, curved elevator into the recess to bluntly sweep away adhesions, or gently force the phalangeal base into flexion to break the synechiae.
Surgical Warning: Careful attention to the vascular anatomy of the volar plate is necessary during this step. Aggressive dissection can injure the vincula supplying the flexor tendons, leading to avascular necrosis or tendon rupture.
5. Management of the Checkrein Ligaments
Sometimes, the standard capsulectomy recommended by Curtis is insufficient to allow full extension of the joint. Watson, Light, and Johnson emphasized the critical importance of the "check" ligaments in maintaining persistent flexion deformities.
These checkreins extend from thick attachments along the proximal edge of the volar plate and diverge to insert separately along the volar-lateral periosteum of the proximal phalanx. Resection of these checkrein ligaments should be considered a mandatory part of all middle joint releases for flexion contractures. Isolate the checkreins bilaterally and resect them sharply, allowing the volar plate to glide distally.
6. Addressing Intrinsic Contractures
Assess the intrinsic muscles (interossei and lumbricals). If the interosseous muscle is contracted (demonstrated by restricted PIP flexion when the metacarpophalangeal joint is held in extension), its tendon must be lengthened.

Perform a step-cut tenotomy of the lateral band/interosseous tendon, elongate it to permit full passive PIP flexion, and repair it with fine non-absorbable suture.
If necessary, free the central slip of the extensor tendon over the dorsum of the finger through the same approach, ensuring it glides smoothly over the proximal phalanx.
7. Intraoperative Assessment of Motion
Satisfactory passive motion must be exhibited during surgery. As a cardinal rule of hand surgery: no further motion can be anticipated after surgery than what is achieved on the operating table.
It is also imperative to confirm that the flexor tendons are not adherent in the palm. Ask the awake, sedated patient to actively attempt to flex the finger.
* If active flexion matches passive flexion, the flexor system is intact and gliding.
* If the tendons are adherent in the palm or at the wrist level, make a separate palmar incision to release them.
* If a complex flexor tenolysis within the digital sheath is necessary to regain active flexion, abort this step and stage the tenolysis 10 to 12 weeks later.
8. Closure and Splinting
Thoroughly irrigate the joint. Repair the transverse retinacular ligament to stabilize the extensor mechanism. Close the skin with interrupted non-absorbable sutures.
Apply a sterile, non-adherent dressing. Fabricate and apply palmar and dorsal plaster splints to hold the hand in the intrinsic-plus position: the wrist extended (20-30 degrees), the metacarpophalangeal joints flexed (70-90 degrees), and the interphalangeal joints fully extended.
POSTOPERATIVE CARE AND REHABILITATION
The success of a PIP joint capsulotomy is heavily dependent on the postoperative rehabilitation protocol. Without rigorous, immediate therapy, the joint will rapidly stiffen, rendering the surgical intervention futile.
Immediate Mobilization
Motion is begun immediately under the strict supervision of a certified hand therapist. The initial bulky dressing is removed within 24 to 48 hours, and a lighter dressing is applied to facilitate movement.
Dynamic and Static Progressive Splinting
The joint is splinted alternately in flexion and extension to maintain the gains achieved in the operating room.
* Extension Splinting: A static progressive or dynamic extension splint is worn at night and during rest periods to prevent recurrence of flexion contractures.
* Flexion Splinting: Flexion strapping or dynamic flexion orthoses are utilized during the day to encourage maximum flexion.
Splinting is continued relentlessly until the full range of motion obtained at surgery is possible actively. Patients must be counseled preoperatively that splinting may be necessary at least part of the time for 3 to 4 months postoperatively.
Long-Term Outcomes
Patients should be educated that while capsulotomy can significantly improve the functional arc of motion, a completely "normal" joint is rarely achieved. A residual lack of terminal extension (10 to 15 degrees) is common and generally well-tolerated functionally. The primary goal is to place the arc of motion into a functional range (e.g., 15 degrees of extension to 80 degrees of flexion) to allow for strong grasp and fine pinch kinematics.
You Might Also Like