Comprehensive Surgical Management of Intraarticular Hand Fractures

Key Takeaway
Intraarticular fractures of the hand, particularly those involving the distal interphalangeal joint, require precise anatomical reduction to restore joint congruity and biomechanical function. Management ranges from conservative extension splinting for stable mallet fractures to complex open reduction and internal fixation for fracture-dislocations. This guide details evidence-based protocols, surgical techniques including Doyle's pull-out wire, and pediatric considerations like Seymour fractures, ensuring optimal functional outcomes and minimizing post-traumatic arthritis.
Principles of Intraarticular Hand Fractures
Intraarticular fractures of the phalanges present a complex biomechanical challenge to the orthopedic surgeon. The delicate interplay between the flexor and extensor mechanisms, combined with the minimal soft-tissue envelope of the digits, demands meticulous surgical technique and a profound understanding of hand anatomy. Fractures involving a single fragment that comprises one-third or more of the articular surface—particularly when accompanied by joint subluxation or dislocation—mandate anatomical reduction and rigid internal fixation. Failure to restore joint congruity inevitably leads to altered kinematics, chronic pain, and post-traumatic osteoarthritis.
The primary goals of intervention are the restoration of articular congruity, the re-establishment of joint stability, and the facilitation of early, controlled mobilization to prevent debilitating stiffness.
Surgical Pearl: Closed reduction of intraarticular distal interphalangeal (DIP) joint fractures can occasionally be achieved by acutely flexing the finger, thereby utilizing the intact soft-tissue hinge to appose the larger diaphyseal fragment to the smaller articular fragment. However, this position is notoriously difficult to maintain and frequently contributes to dorsal skin breakdown over the fracture apex.
Classification and Management of Mallet Finger Fractures
Mallet finger injuries encompass a spectrum of disruptions to the terminal extensor tendon mechanism, ranging from pure tendinous avulsions to complex intraarticular fracture-dislocations.
Type 1: Acute Closed Mallet Finger
Type 1 injuries represent acute, closed disruptions of the terminal extensor tendon, often with a small bony avulsion. If left untreated, the loss of terminal extension alters the biomechanical balance of the digit. The unopposed pull of the central slip at the proximal interphalangeal (PIP) joint, combined with volar plate laxity, frequently results in a secondary "swan neck" deformity.
Standard treatment involves continuous extension splinting of the DIP joint for 6 to 8 weeks. The PIP joint must be left free to mobilize, preventing stiffness and counteracting the swan neck cascade.
Type 2: Open Mallet Finger Injuries
Open type 2 injuries involve a laceration or crush component over the dorsum of the DIP joint. While they can occasionally be managed with closed reduction and splinting following meticulous surgical debridement and wound care, splint management is often complicated by the overlying soft-tissue injury.
In these scenarios, direct repair of the terminal extensor tendon is recommended. This is typically achieved using a dermatendinous roll stitch (e.g., a figure-of-eight suture incorporating both skin and tendon), supplemented by temporary transarticular Kirschner wire (K-wire) fixation of the DIP joint in absolute full extension to protect the repair.
Type 3: Mallet Finger with Extensive Soft-Tissue Loss
Type 3 injuries are severe, involving significant loss of the dorsal skin, subcutaneous tissue, and extensor mechanism. These devastating injuries require complex soft-tissue coverage (such as local rotational flaps or cross-finger flaps) combined with transarticular pinning of the DIP joint. In cases of irreparable articular or tendinous destruction, primary arthrodesis of the DIP joint is the most reliable method to provide a stable, pain-free digit.
Type 4: Intraarticular Mallet Fractures (B and C)
Type 4 injuries involve a significant intraarticular fracture of the distal phalanx. The management of Type 4B (fractures involving 20-50% of the articular surface) and Type 4C (fractures >50% of the articular surface with volar subluxation of the distal phalanx) remains highly controversial in orthopedic literature.
Operative intervention, while anatomically logical, is fraught with complications. Documented risks include deep infection, permanent nail bed deformity, tender pulp scars, iatrogenic comminution, and loss of fixation.
Clinical Controversy: Wehbe and Schneider famously advocated for the nonoperative treatment of all mallet fractures, including those with volar subluxation of the distal phalanx. Their landmark series demonstrated that strict extension splinting yielded satisfactory functional results, and surprisingly, that residual joint incongruity did not significantly correlate with poor long-term clinical outcomes.
Despite this, the prevailing modern consensus among hand surgeons is that fractures involving more than one-third of the articular surface, particularly those with persistent volar subluxation of the distal phalanx despite extension splinting, warrant open reduction and internal fixation (ORIF) to prevent rapid joint destruction.
Pediatric Considerations: Seymour Fractures and Salter-Harris Injuries
Seymour Fractures
Pediatric mallet equivalents, commonly known as Seymour fractures, are juxta-epiphyseal fractures of the distal phalanx. They are frequently misdiagnosed as simple mallet fingers.
Pathoanatomy: A Seymour fracture is almost universally an open fracture. The mechanism of injury causes the proximal edge of the nail plate to avulse from the eponychial fold, resting dorsally on the skin. The germinal matrix is torn, and the fracture site communicates directly with the external environment, evidenced by continuous, slow bleeding around the base of the nail.
Management Protocol:
1. Administer a comprehensive digital block.
2. Thoroughly irrigate and debride the fracture site. This often requires gently flexing the distal fragment to expose the entrapped soft tissues.
3. Extract any interposed germinal matrix or soft tissue from the fracture site.
4. Reduce the fracture anatomically.
5. Carefully tuck the proximal nail plate back beneath the eponychial fold. The nail acts as a highly effective biological splint.
6. Apply a dorsal splint with the DIP joint in neutral or slight extension for 4 weeks.
7. Prescribe prophylactic oral antibiotics covering skin flora.
Surgical Warning: Failure to recognize a Seymour fracture as an open injury, or failure to extract the entrapped nail bed from the fracture site, will inevitably lead to osteomyelitis, premature physeal closure, and severe growth arrest of the distal phalanx.
Salter-Harris Type III Fractures
Displaced Salter-Harris Type III fractures of the distal phalanx epiphysis should initially be managed with closed reduction, achieved by applying mild extension to the distal phalanx. If anatomical reduction of the articular surface cannot be obtained closed—often due to soft tissue interposition—open reduction and fine K-wire fixation of the epiphyseal fragment are strictly indicated.
Surgical Techniques for Intraarticular Fractures
For intraarticular fractures involving more than one-third of the joint surface with associated subluxation, open reduction utilizing a pull-out wire and a transarticular K-wire is the gold standard.
Doyle Technique: Open Reduction and Fixation with Pull-out Wire
Indications: Displaced Type 4 mallet fractures, large avulsion fractures of the DIP joint.
Step-by-Step Surgical Procedure:
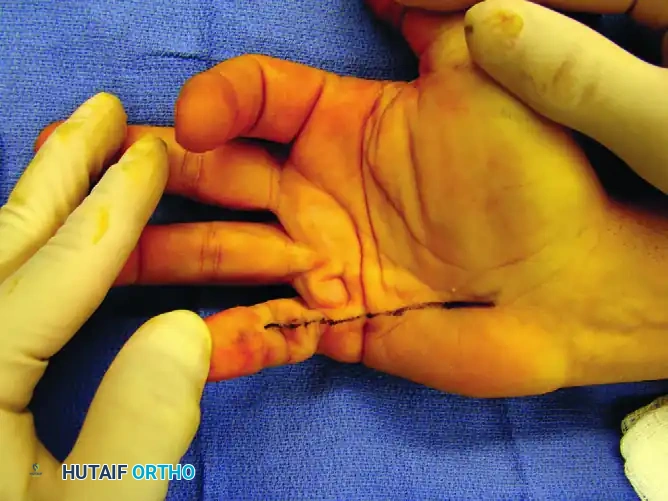
- Exposure: Under tourniquet control and appropriate anesthesia, expose the DIP joint through a dorsal zigzag (Bruner-type) or H-shaped incision to prevent scar contracture over the joint.

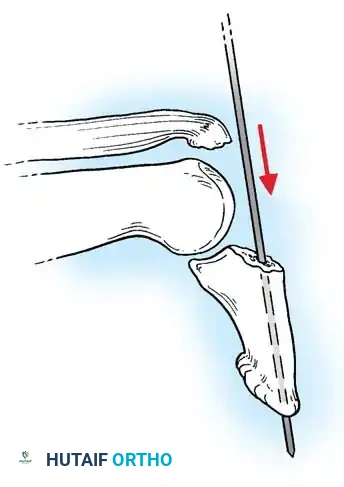
- Distal Wire Placement: Isolate the distal phalanx. Pass a 0.035-inch (0.9 mm) K-wire longitudinally through the center of the distal phalanx, exiting the distal tip of the finger.
-
Reduction: Anatomically reduce the DIP joint. Carefully manipulate the dorsal articular fracture fragment into its anatomical bed using a dental pick or fine periosteal elevator.
-
Transarticular Fixation: Once the joint is reduced and held in full extension, drive the previously placed K-wire proximally across the DIP joint into the middle phalanx to secure the joint in extension. Verify the reduction and joint congruity with multi-planar fluoroscopy.
-
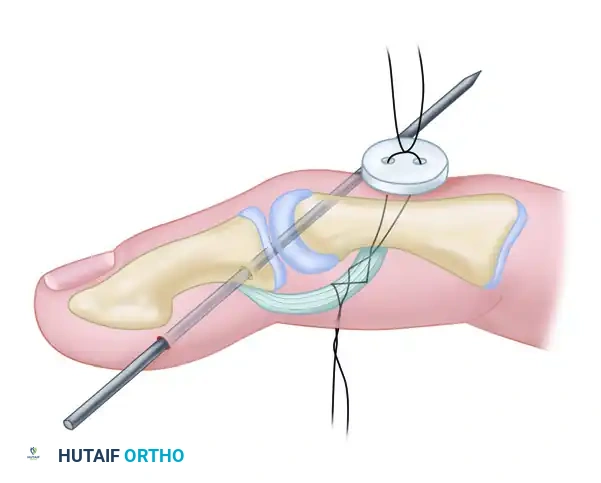
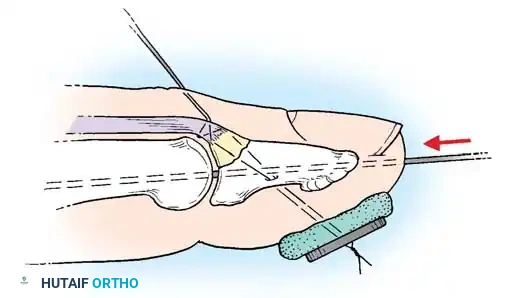
Fragment Fixation (Pull-out Suture): If the dorsal fracture fragment cannot be maintained in rigid apposition to the major diaphyseal fragment, a pull-out suture technique is required. Pass a non-absorbable suture (e.g., 4-0 Prolene) through the extensor tendon insertion on the fragment.

- Securing the Suture: Pass the two ends of the suture volarly through the distal phalanx, exiting the volar pulp. Tie the suture over a heavily padded external button to compress the fragment into place.
Surgical Pitfall: Insufficient padding beneath the volar button will cause rapid ischemic necrosis of the digital pulp. Always use a sterile felt pad or a piece of foam under the button, and avoid excessive tension when tying the suture.
- Closure and Splinting: Close the skin meticulously. Apply a protective volar splint to shield the transarticular K-wire and the pull-out button.
Clinical Case Example
The efficacy of the pull-out wire technique is demonstrated in the management of high-demand athletes.

In this scenario, a Type 4 mallet finger in a high school basketball player (A) was treated with pull-out wire and pin fixation. The transarticular pin is typically removed at 4 weeks (B), allowing early protected motion, while the pull-out wire is maintained until 6 weeks postoperatively (C) to ensure solid bony union of the avulsed fragment.
Alternative Fixation Strategies
Retrograde K-wire Technique:
An alternative to the pull-out wire is direct K-wire fixation. A fine K-wire is drilled directly into the small dorsal fragment. The fracture is reduced, and the wire is driven volarly through the larger fragment. The drill is then attached to the volar end of the wire, pulling it through until the dorsal tip is buried just beneath the articular cartilage of the smaller fragment. The DIP joint is then transfixed with a separate K-wire. Motion can usually commence at 2 weeks, with wire removal at 4 weeks.
AO Screw Fixation:
For larger fragments, a small AO cortical screw (1.2 mm, 1.5 mm, or 2.0 mm) can be utilized.
Biomechanical Rule: Screw fixation is only viable if the width of the articular fragment is at least three times the diameter of the screw being used. Attempting to place a 1.5 mm screw into a 3 mm fragment will inevitably cause iatrogenic comminution and catastrophic failure of fixation.
Bone Grafting for Impaction:
High-energy intraarticular fractures often feature central articular impaction. These depressed articular fragments must be carefully elevated using a fine bone tamp. The resulting metaphyseal void requires supplemental cancellous bone grafting (often harvested from the distal radius or olecranon) to support the articular surface prior to internal fixation.
Avulsion and Hemicondylar Fractures
Avulsion Fractures
Intraarticular fractures frequently present as avulsion injuries at the precise insertion sites of critical tendons and collateral ligaments. The muscular or ligamentous pull widely displaces these fragments.
* Large Fragments (>25% of joint surface): Require open reduction and internal fixation (using screws or K-wires) to restore both ligamentous competence and joint congruity.
* Small Fragments (<25% of joint surface): Treatment is directed primarily at the soft-tissue injury. Management consists of splinting in the position of function or, if the joint is grossly unstable, open repair of the ligament with excision of the tiny bone fragment.
Hemicondylar Fractures
Hemicondylar fractures are typically produced by severe lateral shear stress, most commonly affecting the proximal interphalangeal (PIP) joint. If displaced, these fractures disrupt the bicondylar anatomy of the phalanx, leading to rapid angular deformity and joint destruction.
Internal fixation is mandatory for displaced hemicondylar fractures. While closed reduction and percutaneous pinning can be attempted under fluoroscopic guidance, open reduction is frequently necessary to ensure absolute anatomical alignment of the articular cartilage. Fixation is typically achieved with multiple parallel fine K-wires or interfragmentary mini-screws.
Long-Term Outcomes and Prognosis
The ultimate functional outcome following an intraarticular fracture of the interphalangeal joints depends on a matrix of factors: the patient’s age, the specific location of the injury, the degree of initial comminution, the severity of associated soft-tissue trauma, the anatomical accuracy of the surgical reduction, and strict adherence to postoperative rehabilitation protocols.
A landmark long-term follow-up study by Barton provided critical insights into the natural history of these injuries:
* Pain: Pain predictably diminishes over time. While only 27% of patients reported being completely pain-free at early follow-up, an impressive 66% reported zero discomfort at 11 years post-injury.
* Motion: A gradual improvement in range of motion is observed over the first year, though only 60% of patients ever regain a completely normal arc of motion.
* Radiographic Arthritis: Approximately 17% of patients develop clear radiographic evidence of post-traumatic osteoarthritis.
Clinical Pearl: Barton's study highlighted a crucial paradox in hand trauma: radiographic findings of post-traumatic arthritis correlate very poorly with subjective pain scores. As the injured joint develops osteophytes and stiffens over time, the reduction in micro-motion often leads to a spontaneous decrease in clinical pain, even as the x-ray appears progressively worse.
For patients who develop painful, chronic mallet fingers resulting from untreated or failed fracture-dislocations, salvage procedures are required. Arthrodesis of the distal interphalangeal joint in 0 to 5 degrees of flexion remains the definitive treatment, providing a stable, pain-free pinch grip.
You Might Also Like