Hand Fasciotomies and the Surgical Management of Volkmann Ischemic Contracture
Key Takeaway
Volkmann ischemic contracture represents the devastating sequela of untreated forearm compartment syndrome. Surgical management depends on contracture severity. Acute phases require emergent fasciotomies of the hand and forearm. Established contractures necessitate a staged approach, beginning with radical excision of fibrotic flexor musculature and meticulous neurolysis of the median and ulnar nerves, followed by secondary reconstructive tendon transfers or free functional muscle flaps to restore digital prehension and wrist kinematics.
INTRODUCTION TO VOLKMANN ISCHEMIA AND COMPARTMENT SYNDROME
Compartment syndrome of the upper extremity is a devastating orthopedic emergency characterized by elevated interstitial pressures within a closed osseofascial space, leading to microvascular compromise, tissue hypoxia, and ultimately, myoneural necrosis. When left untreated or inadequately decompressed, this ischemic cascade culminates in Volkmann ischemic contracture—a rigid, fibrotic deformity of the forearm and hand characterized by severe flexor contractures, intrinsic muscle paralysis, and profound sensorimotor deficits.
Historically described by Richard von Volkmann in 1881, the condition was initially attributed to the application of tight splints or bandages. Modern orthopedic understanding recognizes that any mechanism increasing intracompartmental volume (e.g., hemorrhage, edema, reperfusion injury) or decreasing compartmental volume (e.g., tight casts, circumferential burns) can precipitate this ischemic cascade.
The management of this pathology is strictly dichotomous: acute intervention via emergent fasciotomies to prevent irreversible necrosis, and chronic reconstruction via radical debridement, neurolysis, and tendon transfers to salvage function in the established contracture.
PATHOANATOMY AND BIOMECHANICS OF ISCHEMIA
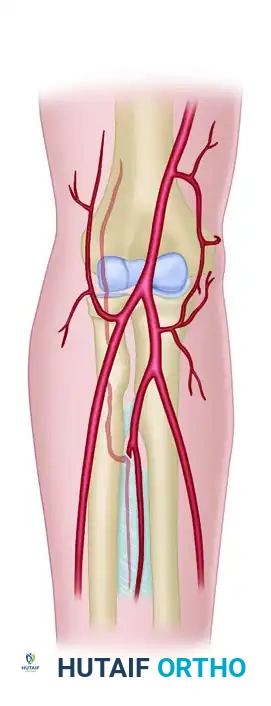
Understanding the precise vascular and neural topography of the forearm is paramount for both acute decompression and chronic reconstruction. The flexor compartment of the forearm is uniquely vulnerable to ischemic insult due to its rigid fascial boundaries and specific anatomical bottlenecks.
The Vascular Bottleneck: The Proximal Guardian
The "collateral circulation" of the elbow does not effectively communicate with the vessels within the deep flexor compartment. These elbow collaterals join the radial and ulnar arteries proximal to the pronator teres. Consequently, the pronator teres acts as the "proximal guardian" of the flexor compartment. If vascular compromise occurs distal to this muscle, the deep flexors (specifically the flexor digitorum profundus [FDP] and flexor pollicis longus [FPL]) are entirely isolated from collateral perfusion.
The Cruciate Tendon-Muscle Portal
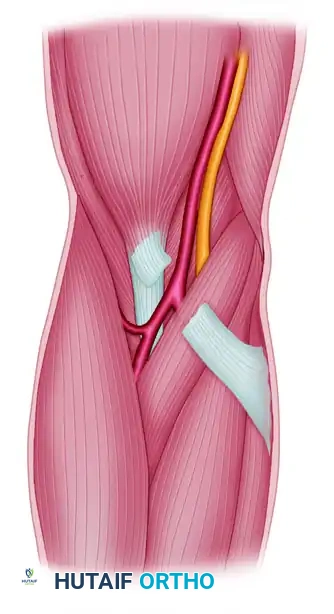
The brachial artery and median nerve enter the forearm through a highly restrictive anatomical portal. This tight opening is bordered laterally by the rigid biceps tendon insertion and medially by the fleshy pronator teres muscle. The entire complex is tightly roofed by the unyielding lacertus fibrosus (bicipital aponeurosis).
Surgical Warning: Proximal angulation of a supracondylar humerus fracture, expanding hematoma, or reactive muscle swelling within this cruciate tendon-muscle portal is capable of causing major, rapid compression of the neurovascular bundle. Division of the lacertus fibrosus is a mandatory step in any volar forearm fasciotomy.
Arterial and Neural Trajectories
Once past the lacertus fibrosus, the neurovascular structures diverge, dictating their respective vulnerabilities:
* Radial Artery: Arising from the brachial artery, it passes distally and superficial to the pronator teres and all flexor muscles. It is not crossed by any major fascial structure along this route, making it relatively less susceptible to deep compartmental compression.
* Ulnar Artery: Passes deep beneath the pronator teres and lies in the deepest, most rigid portions of the flexor compartment, rendering it highly vulnerable to elevated intracompartmental pressures.
* Median Nerve: The median nerve usually passes between the humeral and ulnar heads of the fleshy pronator teres. Upon emerging, it dives deep to the flexor digitorum sublimis (FDS). During severe edema, the nerve becomes aggressively compressed against the firm, unyielding arcuate band of the FDS origin.
ACUTE MANAGEMENT: HAND AND DIGITAL FASCIOTOMIES
In the acute setting of compartment syndrome, time is tissue. Irreversible muscle necrosis begins within 4 to 6 hours of ischemia, and nerve damage can become permanent shortly thereafter. When intracompartmental pressures exceed 30 mm Hg (or are within 20-30 mm Hg of the patient's diastolic blood pressure), emergent fasciotomy is indicated.
While volar and dorsal forearm fasciotomies are standard, the intrinsic compartments of the hand (thenar, hypothenar, adductor, and interosseous compartments) must not be overlooked.
Dorsal Hand Fasciotomies
To decompress the interosseous compartments, dorsal longitudinal incisions are utilized.
1. Incision Placement: Two longitudinal incisions are typically made. The first is placed over the index metacarpal (second metacarpal) to access the first and second dorsal interosseous compartments. The second is placed over the ring metacarpal (fourth metacarpal) to access the third and fourth dorsal interosseous compartments.
2. Fascial Release: Blunt dissection is carried down to the dorsal fascia. The fascia over each interosseous muscle is incised longitudinally. Care must be taken to protect the dorsal sensory branches of the radial and ulnar nerves, as well as the extensor paratenon.

Digital Fasciotomies
Digital compartment syndrome, though rare, can occur following severe crush injuries, snakebites, or high-pressure injection injuries.
1. Midaxial Approach: A midaxial incision is made along the non-tactile border of the digit (ulnar side for index and middle fingers; radial side for ring and small fingers).
2. Ligamentous Release: The incision is carried through the skin and subcutaneous tissue. The transverse retinacular ligament is identified and preserved if possible, but the fascia enveloping the neurovascular bundle must be released. Cleland's ligaments (dorsal to the neurovascular bundle) and Grayson's ligaments (volar to the bundle) may need to be selectively divided to fully decompress the digital cylinder.
CLASSIFICATION OF ESTABLISHED VOLKMANN CONTRACTURE
If acute compartment syndrome is missed or inadequately treated, the necrotic muscle is gradually replaced by dense, inelastic scar tissue. The resulting Volkmann ischemic contracture is classified based on severity, which dictates the reconstructive approach.
Mild Contracture
- Pathology: Localized ischemia primarily affecting the deepest muscles, most commonly the flexor digitorum profundus (FDP) of the middle and ring fingers.
- Clinical Presentation: Flexion contracture of two or three fingers. Sensation is usually intact, and intrinsic hand function is preserved.
- Management: Dynamic splinting and functional training. If conservative measures fail after 3 months, surgical release, fractional tendon lengthening, or a localized muscle sliding operation may be indicated.
Moderate Contracture
- Pathology: Involves the long finger flexors (FDP and FDS), the flexor pollicis longus (FPL), and potentially the wrist flexors.
- Clinical Presentation: Classic "claw hand" presentation. The wrist is flexed, metacarpophalangeal (MCP) joints are hyperextended, and interphalangeal (IP) joints are flexed. Median and ulnar nerve sensory changes are prominent due to nerve strangulation within the fibrotic muscle bed. Intrinsic minus deformities are present.
- Management: Requires a comprehensive muscle sliding operation, meticulous neurolysis of the median and ulnar nerves, and excision of fibrotic muscle masses. If no useful movement of the finger flexors is retained, volar transfers of dorsal wrist extensors (e.g., brachioradialis, extensor carpi radialis longus) are required.
Severe Contracture
- Pathology: Global involvement of both flexors and extensors of the forearm. Often complicated by malunited fractures of the radius/ulna and severe cutaneous scarring.
- Clinical Presentation: A rigid, non-functional, insensate extremity. Nerves are severely strangulated by dense, scarred musculature.
- Management: Early, radical excision of all necrotic muscles combined with complete median and ulnar neurolysis to restore sensibility. Tendon transfers are performed as a secondary procedure. If local motor units are unavailable, a free innervated muscle transfer (e.g., functioning free gracilis flap) is required.
SURGICAL TECHNIQUE 74-4: MUSCLE SLIDING OPERATION & RECONSTRUCTION
The muscle sliding operation, originally described by Page in 1923 and popularized by Scaglietti in 1957, involves the proximal release and distal advancement of the flexor pronator origin. However, in true Volkmann contracture, the muscle is often entirely fibrotic and noncontractile, making a simple sliding operation insufficient. A radical debridement combined with secondary tendon transfers is the gold standard.
Clinical Pearl: Do not attempt tendon transfers during the primary debridement stage. The primary goal is to excise necrotic tissue, decompress the nerves, and restore passive joint suppleness. Tendon transfers performed in a stiff, scarred bed will inevitably fail.
Stage 1: Radical Debridement and Neurolysis
-
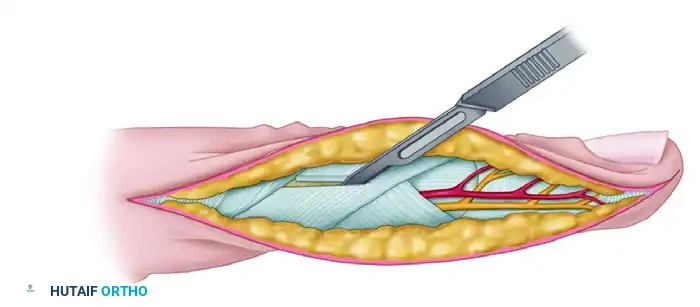
Incision and Exposure:
- Utilize an extensive volar forearm incision, beginning proximal to the medial epicondyle, crossing the antecubital fossa obliquely, and extending distally down the volar forearm, incorporating a carpal tunnel release.
- Elevate thick fasciocutaneous flaps to ensure adequate skin coverage postoperatively.
-
Muscle Excision (Infarctectomy):
- Systematically evaluate the flexor pronator mass. Viable muscle will bleed when cut and contract when stimulated.
- Excise all avascular, fibrotic masses of the flexor digitorum profundus (FDP) and flexor digitorum sublimis (FDS). Be ruthless in the debridement of pale, non-contractile scar tissue, but meticulously preserve any muscle fascicles that appear viable.
-
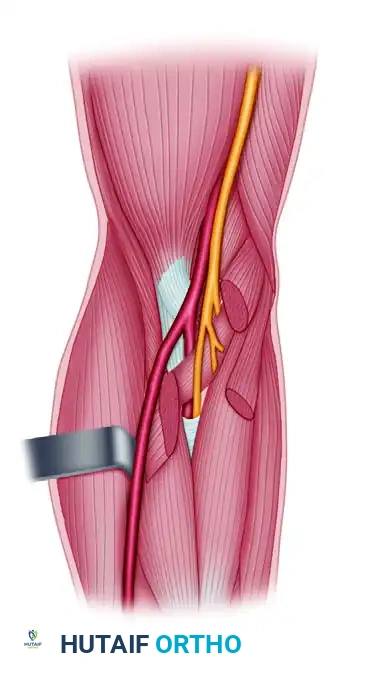
Meticulous Neurolysis:
- Identify the median and ulnar nerves in virgin tissue proximally and distally, then trace them into the zone of injury.
- The median nerve is typically the most severely affected. It is often found compressed beneath the lacertus fibrosus, between the heads of the pronator teres, and under the FDS arcade.
- Look for the classic "hourglass deformity" in the midforearm, indicating severe focal constriction. Perform an epineurotomy if the nerve feels indurated. If a dense neuroma-in-continuity is present with no distal conduction, segmental resection and secondary nerve grafting (using the sural nerve) may be necessary.
-
Correction of Deformities:
- Correct the rigid finger and wrist flexion deformities by dividing the involved, fibrotic flexor tendons at their musculotendinous junctions.
- Perform a complete release of the wrist and finger flexors until the hand can be brought into a functional, neutral position passively.
- Close the wound over drains. If skin closure is too tight, utilize split-thickness skin grafts to prevent recurrent compartment syndrome.
Stage 2: Reconstructive Tendon Transfers
Once passive range of motion is restored, soft tissues have healed, and maximal nerve recovery has been achieved (often 3 to 6 months post-Stage 1), reconstructive tendon transfers are performed to restore active prehension.
Biomechanical Prerequisite: At least one strong wrist extensor (usually the Extensor Carpi Radialis Brevis - ECRB) must be retained in its native position to stabilize the wrist during finger flexion. Without a stable wrist, the transferred tendons will suffer from active insufficiency.
-
Restoration of Thumb Flexion:
- The Brachioradialis (BR) is the motor of choice for the thumb. It has excellent strength and adequate excursion when fully mobilized.
- Transfer the BR to the Flexor Pollicis Longus (FPL) tendon. The BR must be mobilized proximally to the level of the elbow joint to maximize its excursion.
-
Restoration of Digital Flexion:
- The Extensor Carpi Radialis Longus (ECRL) is transferred to the Flexor Digitorum Profundus (FDP) tendons of all four fingers.
- The FDP tendons are sutured together side-to-side (pulvertaft weave or side-to-side tenodesis) to create a single functional unit, ensuring a synchronized mass flexion of the digits.
- The ECRL is routed volarly, superficial to the radius, and woven into the conjoined FDP tendons under appropriate tension (usually with the wrist in neutral and fingers in resting cascade).
-
Salvage Options for Severe Cases:
- If local extensor motors are unavailable or insufficient, a Free Functioning Muscle Transfer (FFMT) is indicated.
- The Gracilis muscle is harvested with its neurovascular pedicle (obturator nerve and ascending branch of the medial circumflex femoral artery).
- The muscle is inset into the forearm, the artery is anastomosed to the radial or ulnar artery, and the obturator nerve is coapted to the anterior interosseous nerve (AIN) or a viable fascicle of the median nerve.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of surgical intervention for Volkmann contracture relies heavily on rigorous, specialized hand therapy.
- Immobilization: Following tendon transfers, the upper extremity is immobilized in a bulky plaster splint. The wrist is positioned in 30 degrees of extension, the MCP joints in 70 degrees of flexion, and the IP joints in full extension to protect the transfers.
- Early Phase (Weeks 3-6): The cast is removed at 3 to 4 weeks. A thermoplastic dorsal blocking splint is fabricated. Active extension within the limits of the splint and passive flexion are initiated to allow the tendons to glide without placing tension on the anastomoses.
- Intermediate Phase (Weeks 6-10): The splint is gradually discontinued during the day. Active flexion exercises are initiated. Neuromuscular electrical stimulation (NMES) and biofeedback are highly beneficial to help the patient cognitively "remap" the transferred extensor muscles to perform flexor functions.
- Late Phase (Months 3+): Progressive strengthening and work-hardening programs are introduced. Sensory re-education is critical, especially if neurolysis or nerve grafting was performed during the first stage.
While a return to normal, pre-injury function is rare in established Volkmann contracture, meticulous surgical execution combined with dedicated rehabilitation can reliably restore a functional assist hand, providing the patient with meaningful grasp, pinch, and release capabilities.
You Might Also Like


