Operative Management of Congenital Hand Duplication: Polydactyly and Triphalangism

Key Takeaway
Polydactyly, or digit duplication, is a conspicuous congenital hand anomaly requiring meticulous surgical reconstruction to optimize both function and aesthetics. Preaxial polydactyly (bifid thumb) is the most common variant. Successful management relies on accurate Wassel classification, preservation of the dominant ulnar digit, precise realignment of eccentric tendinous insertions, and robust collateral ligament reconstruction to prevent late angular deformity and Z-collapse.
DUPLICATION (POLYDACTYLY): PATHOPHYSIOLOGY AND CLASSIFICATION
Duplication of digits, commonly referred to as polydactyly, represents one of the most frequent and conspicuous congenital anomalies of the upper extremity. Documented in historical and biblical literature over 3,000 years ago, its prevalence remains significant, with approximately 9,000 to 10,000 new cases recorded globally each year. Embryologically, duplication arises from an abnormal induction of the apical ectodermal ridge (AER) or a disruption in the zone of polarizing activity (ZPA) during the critical period of limb bud formation (weeks 4 to 8 of gestation).
Polydactyly is broadly classified into three primary anatomical categories:
1. Preaxial Polydactyly: Duplication of the thumb (bifid thumb).
2. Central Polydactyly: Duplication involving the index, long, or ring fingers (often associated with syndactyly).
3. Postaxial Polydactyly: Duplication of the small finger (ulnar polydactyly).
Also included within the broader spectrum of duplication anomalies is ulnar dimelia (mirror hand), an exceedingly rare and complex anomaly characterized by the absence of the radial ray, duplication of the ulna, and symmetrical duplication of the ulnar digits.
Syndromic Associations and Differentials
While many duplications occur as isolated, sporadic events, the orthopedic surgeon must maintain a high index of suspicion for associated systemic syndromes. Preaxial polydactyly can be associated with visceral anomalies, most notably Holt-Oram syndrome (hand-heart syndrome) and Fanconi anemia.
Furthermore, complex hand anomalies, including severe syndactyly and broad thumbs, may present in craniosynostosis syndromes such as Apert syndrome.
Fig. 76-42 Apert syndrome. A, Characteristic facial features of high forehead and wide-set eyes. B, Complex syndactyly involving all fingers of both hands; left hand has had syndactyly release.
PREAXIAL POLYDACTYLY (BIFID THUMB)
The bifid thumb represents a complete or partial duplication of the first ray. It is the most prevalent duplication pattern in White and Asian populations, occurring in approximately 1 per 3,000 live births.
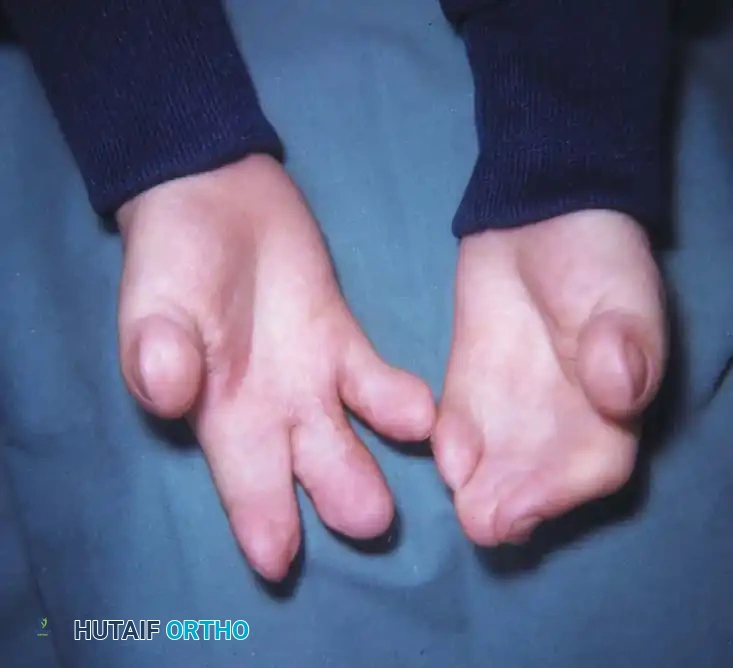
Clinical presentation of a bifid thumb demonstrating divergent duplication.
Etiology and Genetics
The majority of bifid thumbs occur sporadically and unilaterally. In Wassel’s landmark series, only 9 of 70 patients exhibited bilateral involvement. This sporadic nature strongly suggests environmental or teratogenic factors rather than a strict genetic predisposition. Experimental models have successfully reproduced preaxial polydactyly in the offspring of rats via the administration of cytosine arabinoside during pregnancy. However, when thumb duplication is associated with a triphalangeal thumb, an autosomal dominant inheritance pattern is frequently identified.
Clinical and Biomechanical Anatomy
The clinical appearance of a bifid thumb varies dramatically, ranging from a mild widening of the distal phalanx with a central nail groove to a complete duplication of the entire first ray.
Clinical Pearl: Typically, both duplicated digits exhibit some degree of hypoplasia. The radial duplicate is almost universally the more hypoplastic of the two. Therefore, surgical reconstruction generally favors the preservation of the ulnarmost digit to maintain the critical ulnar collateral ligament (UCL) complex necessary for pinch kinematics.
Pathoanatomy of the Bifid Thumb:
* Osteology: The phalanges may be angulated, and a delta phalanx (longitudinally bracketed epiphysis) may be present, driving progressive deviation. The articular surfaces of the shared joints are often widened and incongruous.
* Ligamentous Structures: The collateral ligaments of the duplicated joints are frequently shared. There is inherent insufficiency in the interdigital space along the adjacent sides of the duplicates.
* Intrinsic Musculature: The ulnar-innervated intrinsic muscles (adductor pollicis and deep head of the flexor pollicis brevis) typically insert on the ulnarmost duplicate. Conversely, the median-innervated intrinsics (abductor pollicis brevis, superficial head of the FPB, and opponens pollicis) insert on the radialmost duplicate.
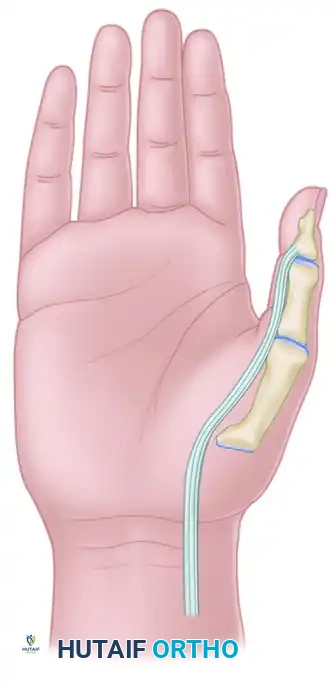
* Extrinsic Tendons: The flexor pollicis longus (FPL) and extensor pollicis longus (EPL) tendons are often duplicated or bifurcated, inserting eccentrically along the adjacent borders of each thumb. This eccentric pull is the primary driver of the classic "Z-collapse" deformity seen in untreated or inadequately reconstructed digits.
* Neurovascular Bundles: Wide anatomical variations exist. The radial and ulnar neurovascular bundles may be completely duplicated or shared, with small arborizing branches supplying the individual digits.

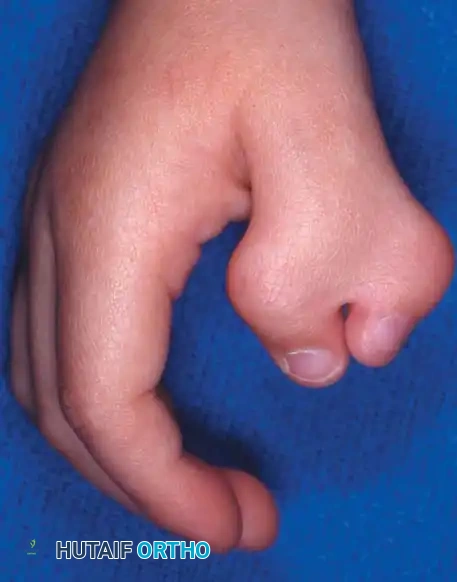
Fig. 76-43 Bifid thumb. A and B, Type II duplication demonstrating partial bifurcation at the distal phalanx.


Fig. 76-43 Bifid thumb. C and D, Type IV duplication (the most common variant), showing complete duplication of the proximal and distal phalanges.
The Wassel Classification
Wassel’s classification system (1969) remains the universal standard for categorizing thumb polydactyly based on the level of skeletal bifurcation.
- Type I: Partial duplication of the distal phalanx with a common epiphysis.
- Type II: Complete duplication of the distal phalanx, including its epiphysis.
- Type III: Duplication of the distal phalanx with bifurcation of the proximal phalanx.
- Type IV: Complete duplication of both the distal and proximal phalanges (Most common: 47%).
- Type V: Complete duplication of the distal and proximal phalanges with bifurcation of the metacarpal.
- Type VI: Complete duplication of the distal and proximal phalanges and the metacarpal.
- Type VII: Variable degrees of duplication associated with a triphalangeal thumb (20%).
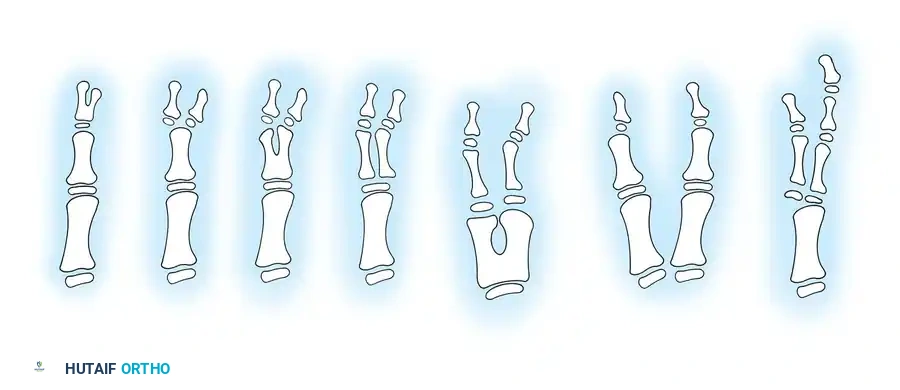
Fig. 76-44 Wassel classification of thumb polydactyly. (Redrawn from Wassel HD: The results of surgery for polydactyly of the thumb: a review, Clin Orthop Relat Res 64:175, 1969.)
SURGICAL MANAGEMENT OF PREAXIAL POLYDACTYLY
Indications and Timing
Surgical correction of the bifid thumb is almost universally indicated to optimize both cosmetic appearance and biomechanical function. The optimal timing for surgical reconstruction is between 12 to 18 months of age. Intervention before age 5 is highly recommended to allow for maximal cerebral plasticity and integration of the reconstructed thumb into functional pinch patterns.
Surgical Warning: Simple amputation or ablation of the hypoplastic radial digit is strictly contraindicated. Simple excision inevitably leads to progressive angular deformity, joint instability, and a functionally compromised thumb due to the loss of the abductor pollicis brevis insertion and radial collateral ligament insufficiency.
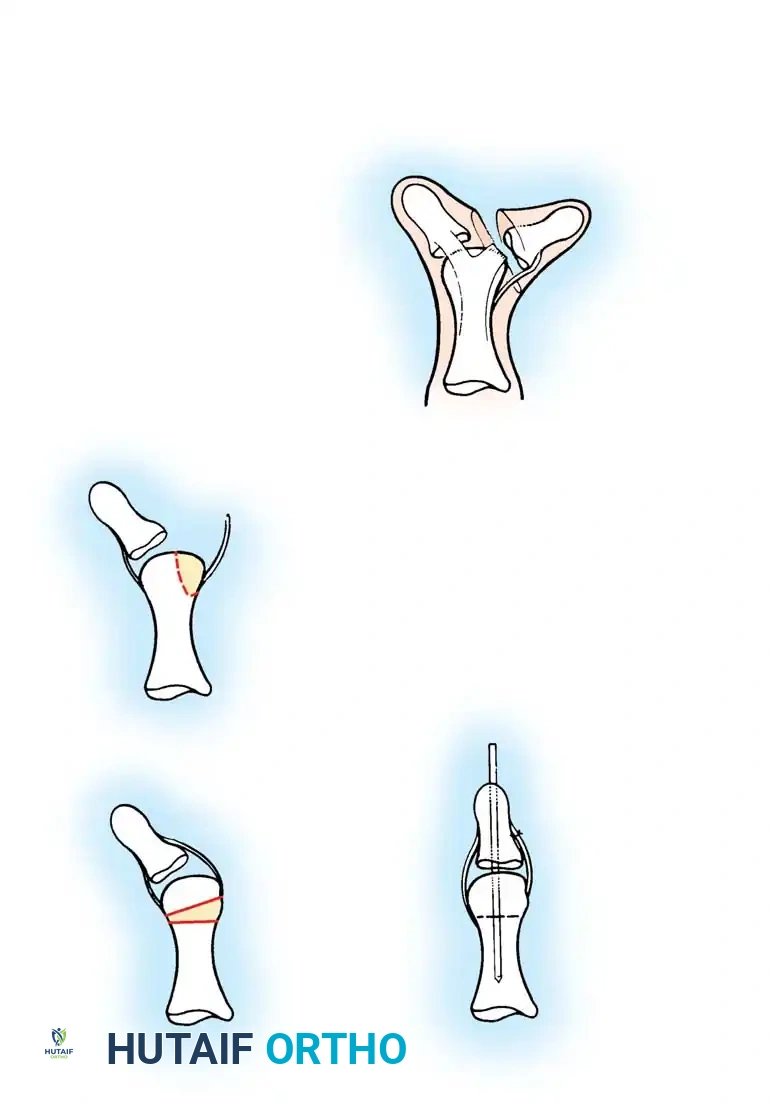
Technique 76-25: The Bilhaut-Cloquet Procedure (For Types I and II)
The Bilhaut-Cloquet procedure is a complex reconstructive option reserved primarily for symmetrical Type I and Type II bifid thumbs where neither digit alone possesses adequate soft tissue or osseous volume to create a functional, aesthetically pleasing thumb.
Surgical Steps:
1. Incision and Exposure: Under tourniquet control and loupe magnification, design a central, wedge-shaped incision extending from the dorsal nail fold to the palmar aspect of the thumb tip, continuing proximally to the level of the skeletal bifurcation. The dorsal component must precisely bisect the conjoined nail and nail bed.
2. Osteochondral Resection: Incise the central component of the underlying tendon and bone. Excise the adjacent (central) halves of the duplicated distal phalanges.
3. Articular Approximation: Carefully approximate the remaining lateral halves of the articular surface and the epiphysis.
4. Fixation: Secure the osteosynthesis with a transverse or longitudinal smooth Kirschner wire (K-wire). Note: Approximation may be difficult due to the tethering effect of the intact collateral ligaments.
5. Soft Tissue Closure: Meticulously repair the nail bed using 6-0 or 7-0 absorbable sutures (e.g., chromic gut) to prevent postoperative nail ridging. Close the skin with interrupted sutures.
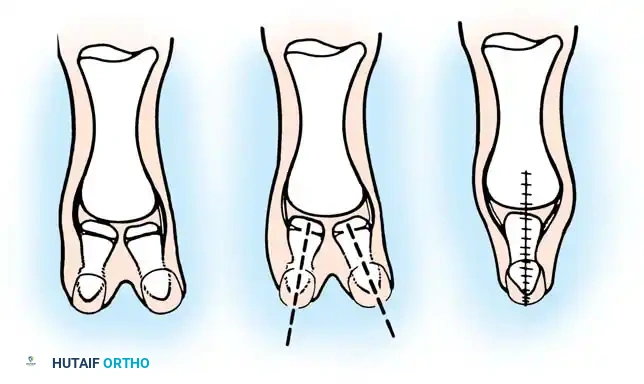



Fig. 76-45 A-D, Bilhaut-Cloquet technique for symmetrical thumb duplication. The duplicate digits are joined at the midline after excision of excess central soft and osseous tissue.
Postoperative Protocol:
Apply a well-padded short-arm or long-arm thumb spica cast (long-arm is preferred in younger children to prevent slippage). The cast is removed at 4 to 6 weeks, at which point the K-wire is extracted, and progressive mobilization is initiated.
Technique 76-26: Excision and Reconstruction (Lamb, Marks, and Bayne) (For Types III through VI)
For asymmetrical duplications (the vast majority of cases), preservation of the dominant ulnar thumb with transfer of the radial structures is the gold standard.

Preoperative surgical markings outlining the racquet-shaped incision designed to excise the hypoplastic radial duplicate while preserving local skin flaps for tension-free closure.
Surgical Steps:
1. Incision: Under tourniquet control, make a racquet-shaped incision over the most hypoplastic thumb (typically the radialmost digit).
2. Intrinsic Tendon Preservation: Carefully dissect and identify the abductor pollicis brevis (APB) tendon as it inserts into the proximal phalanx of the radial duplicate. Detach it with a generous sleeve of periosteum for later transfer.
3. Ligamentous Dissection: Detach the radial collateral ligament (RCL) distally from the phalanx to be excised. Strip the RCL proximally off the metacarpal or phalanx, preserving it as a robust osteoperiosteal flap.
4. Ablation: Excise the supernumerary radial digit along with its corresponding articular facet.
5. Joint Contouring: If the metacarpal head is excessively broad or bifurcated, perform a longitudinal shaving osteotomy to narrow the articular surface, ensuring it matches the base of the preserved proximal phalanx.
6. Realignment and Fixation: Centralize the remaining ulnar digit over the newly contoured articular surface. Secure the alignment with a longitudinal K-wire driven retrograde across the joint.
7. Ligament and Tendon Reconstruction: Advance and suture the preserved RCL and the APB tendon securely to the radial base of the preserved proximal phalanx. This step is critical to prevent late ulnar deviation.
8. Tendon Centralization: Inspect the FPL and EPL tendons. If their insertion is eccentric, perform a partial resection, centralization, or transfer to ensure a perfectly central line of pull.
9. Closure: Close the skin with simple interrupted sutures. A Z-plasty may be required in the first web space or along the ulnar border to prevent scar contracture.
Post-ablation closure demonstrating meticulous skin approximation. Note the centralized alignment of the preserved ulnar digit.
Postoperative Protocol:
The thumb is immobilized in a cast for 4 weeks. Following K-wire removal, a custom thermoplastic protective splint is utilized for an additional 3 to 4 weeks during active play to protect the ligamentous reconstruction.
Complications and Salvage Procedures
Despite meticulous surgical technique, complications can occur. Long-term follow-up studies (e.g., Ogino et al.) indicate that unsatisfactory results are most common in Wassel Types III, V, VI, and triphalangeal variants.
- Z-Collapse Deformity: The most frequent late complication, characterized by interphalangeal joint hyperflexion and metacarpophalangeal joint hyperextension. It is driven by inadequate centralization of the extrinsic tendons and failure to reconstruct the collateral ligaments.
- Salvage: Miura described a successful salvage procedure for Z-collapse utilizing a rotation skin flap on the concave side of the deformity, combined with excision of the radial half of the extensor tendon and transfer of the flexor tendon to the ulnar side of the distal phalanx. Severe late instability may necessitate corrective closing-wedge osteotomies or arthrodesis in children older than 8 to 10 years.
TRIPHALANGEAL THUMB
A triphalangeal thumb is defined by the presence of three phalanges instead of the normal two. This rare anomaly is frequently inherited as an autosomal dominant trait and has historical associations with maternal thalidomide exposure.
Triphalangeal thumbs frequently coexist with other congenital anomalies, including cleft foot, tibial hemimelia, congenital heart disease, and gastrointestinal malformations.

Radiograph demonstrating a triphalangeal thumb with a distinct extra phalanx interposed between the proximal and distal phalanges.
Pathoanatomy and Classification
Triphalangeal thumbs are broadly categorized into two major morphological types based on the shape of the extra ossicle:
1. Type I (Delta Phalanx / Wedge-Shaped Ossicle):
The extra phalanx is small and wedge-shaped (a delta phalanx with a longitudinally bracketed epiphysis). This asymmetrical growth plate causes a progressive, severe angular deformity (clinodactyly) without significantly increasing the overall length of the thumb. The thumb is typically deviated ulnarward at the interphalangeal joint level.
2. Type II (Five-Fingered Hand / Rectangular Phalanx):
The extra phalanx is rectangular and nearly normal in appearance, creating the illusion of a five-fingered hand. The thumb is abnormally long and lies in the same plane as the other digits (loss of pronation).
Clinical photograph of a Type II triphalangeal thumb (five-fingered hand). Note the excessive length and the lack of normal thenar pronation, placing the digit in the same plane as the fingers.
Clinical Pearl: Patients with Type II deformities are often unable to perform true opposition. Because the digit lacks normal pronation and is frequently associated with severe hypoplasia of the thenar intrinsic musculature, patients resort to compensatory side-to-side (key) prehension.
Buck-Gramcko Transitional Type:
A transitional variant exists wherein a trapezoidal extra phalanx causes both an increase in longitudinal length and a progressive angular deformity.


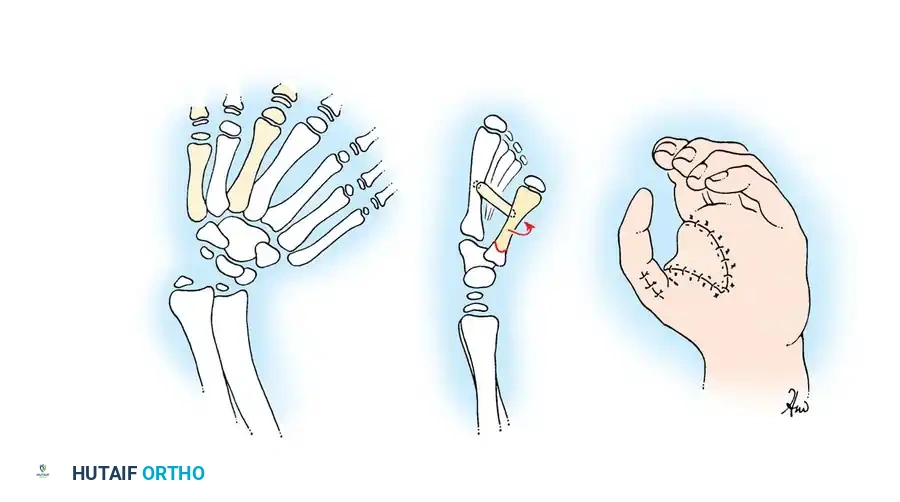
Preoperative and postoperative clinical images demonstrating the correction of a complex duplication and angular deformity associated with triphalangism.
Surgical Management of Triphalangism
The surgical approach to the triphalangeal thumb is dictated by the shape of the extra phalanx and the degree of thenar hypoplasia.
- For Delta Phalanx (Type I): Early surgical intervention is critical. Treatment involves excision of the wedge-shaped delta phalanx and reconstruction of the collateral ligaments. If the remaining joints are unstable, or if the child presents late with severe deformity, a closing-wedge osteotomy of the adjacent phalanx or an arthrodesis of the abnormal joint may be required.
- For Five-Fingered Hand (Type II): Management is highly complex. It often requires shortening of the ray (via excision of the extra rectangular phalanx or a diaphyseal shortening osteotomy), deepening of the first web space (Z-plasty or dorsal rotational flaps), and an opponensplasty (e.g., Huber transfer using the abductor digiti minimi, or an FDS transfer) to restore functional opposition and pinch kinematics.
📚 Medical References
- Thumb polydactyly with symphalangism, J Hand Surg 30B:346, 2005.
- Andrew JG, Sykes PJ: Duplicate thumbs: a survey of results in twenty patients, J Hand Surg 13B:50, 1988.
- Bilhaut M: Guerison d’un pouce bifi de per un nouveau procede operatoire, Cong Fren Chir 4:576, 1890.
- Dobyns JH, Lipscomb PR, Cooney WP: Management of thumb duplication, Clin Orthop Relat Res 195:26, 1985.
- Iwasawa M, Matsuo K, Hirose T, et al: Improvement in the surgical results of treatment of duplicated thumb by preoperative splinting, J Hand Surg 14A:941, 1989.
- Kawabata H, Tada K, Masada K, et al: Revision of residual deformities after operations for duplication of the thumb, J Bone Joint Surg 72A:988, 1990.
- Kemnitz S, De Smet L: Pre-axial polydactyly: outcome of the surgical treatment, J Pediatr Orthop B 11:79, 2002.
- Larsen M, Nicolai JPA: Long-term follow-up of surgical treatment for thumb duplication, J Hand Surg 30B:276, 2005.
- Manske PR: Treatment of duplicated thumb using a ligamentous/periosteal fl ap, J Hand Surg 14A:728, 1989.
- Marks TW, Bayne LG: Polydactyly of the thumb: abnormal anatomy and treatment, J Hand Surg 3A:107, 1978.
- Miura T: Non-traumatic fl exion deformity of the proximal interphalangeal joint—its pathogenesis and treatment, Hand 15:25, 1983.
- Ogino T, Ishii S, Minami M: Radially deviated type of thumb polydactyly, J Hand Surg 13B:315, 1988.
- Ogino T, Ishii S, Takahata S, et al: Long-term results of surgical treatment of thumb polydactyly, J Hand Surg 21A:478, 1996.
- Wassel HD: The results of surgery for polydactyly of the thumb: a review, Clin Orthop Relat Res 64:175, 1969.
- Wood VE: Polydactyly and the
You Might Also Like