Tenodesis of the Extensor Carpi Ulnaris and Transfer of the Pronator Quadratus for Distal Ulna Instability

Key Takeaway
The Kleinman and Greenberg technique—comprising extensor carpi ulnaris (ECU) tenodesis and pronator quadratus transfer—is a highly effective salvage procedure for symptomatic distal ulna instability following a failed Darrach resection. By dynamically stabilizing the ulnar stump, the ECU prevents radioulnar impingement, while the pronator quadratus mitigates dorsal translation. This comprehensive guide details the biomechanics, indications, and step-by-step surgical execution required to restore wrist stability and function.
Introduction to Distal Ulnar Instability and Salvage Procedures
The distal radioulnar joint (DRUJ) is a complex articulation critical for forearm rotation and load transmission across the wrist. Historically, the Darrach procedure (resection of the distal ulna) was widely utilized to address DRUJ arthritis, trauma, and Madelung's deformity. However, a notorious and debilitating complication of the Darrach resection is painful instability of the remaining distal ulnar stump. Deprived of its ligamentous tethers—specifically the triangular fibrocartilage complex (TFCC) and the distal interosseous membrane—the ulnar stump becomes subject to the unopposed deforming forces of the forearm musculature.
This instability manifests clinically as radioulnar convergence (impingement of the ulnar stump against the radius during forceful grip) and dorsal translation or "winging" of the ulna. While various prosthetic replacements have been developed, silicone ulnar head implants have not been found to be durable enough for use in active patients applying significant forces to the ulnocarpal and radioulnar joints. Consequently, soft-tissue stabilization techniques remain the gold standard for high-demand patients.
The technique described by Kleinman and Greenberg—combining the tenodesis of the extensor carpi ulnaris (ECU) with the transfer of the pronator quadratus (PQ)—provides a robust, dynamic, and biologic solution to distal ulnar instability.
Biomechanics and Pathoanatomy
Understanding the biomechanical rationale of the Kleinman and Greenberg procedure requires a thorough appreciation of forearm kinematics following distal ulna resection.
The Role of the Pronator Quadratus
In the intact forearm, the pronator quadratus is a primary forearm pronator and a dynamic stabilizer of the DRUJ. Following a Darrach resection, the loss of the distal ulnar articulation alters the vector of the PQ. The muscle's contraction pulls the distal ulnar stump radiopalmarly, contributing to radioulnar convergence. Furthermore, the lack of skeletal support allows the ulnar stump to translate dorsally ("winging") during pronation.
* Surgical Rationale: Transferring the pronator quadratus and interposing it between the radius and the ulna serves a dual purpose. It provides a biologic soft-tissue buffer that retards radioulnar impingement, and its repositioning alters the vector of pull, effectively retarding dorsal translation ("winging") of the ulnar stump.
The Role of the Extensor Carpi Ulnaris (ECU)
The ECU resides within the sixth dorsal compartment of the extensor retinaculum. It is a powerful ulnar deviator and wrist extensor. In the setting of a resected distal ulna, the ECU loses its stable fulcrum.
* Surgical Rationale: Utilizing a distally based slip of the ECU tendon to tether the ulnar stump to the carpus or stabilizing the ECU via a retinacular sling creates a strong, dynamic checkrein. This tenodesis effectively retards radioulnar impingement by suspending the ulnar stump and preventing it from collapsing into the radius during power grip.
💡 Clinical Pearl: The Dynamic Interplay
The success of this procedure relies on the synergistic effect of both transfers. The ECU tenodesis acts as a longitudinal suspension system preventing transverse convergence, while the PQ transfer acts as a transverse spacer and dynamic depressor preventing dorsal winging. Omitting one component significantly increases the risk of recurrent symptomatic instability.
Indications and Contraindications
Indications
- Symptomatic instability of the distal ulnar stump following a previous Darrach resection.
- Painful radioulnar convergence (impingement) confirmed clinically and radiographically.
- Dorsal "winging" of the distal ulna causing pain or extensor tendon irritation.
- High-demand or active patients for whom silicone or metallic ulnar head arthroplasty is contraindicated due to the risk of catastrophic implant failure or loosening.
Contraindications
- Active surgical site infection.
- Severe global wrist instability or advanced radiocarpal arthritis (may require total wrist arthrodesis).
- Inadequate ECU tendon integrity (e.g., previous rupture or severe tendinopathy).
- Lack of patient compliance with strict postoperative immobilization and rehabilitation protocols.
Preoperative Evaluation and Planning
Clinical Examination
Patients typically present with ulnar-sided wrist pain, weakness in grip strength, and a visible dorsal prominence of the distal ulna. The "squeeze test" (compressing the distal radius and ulna together) often reproduces the patient's pain, indicating radioulnar impingement. Evaluate the integrity of the ECU by resisting ulnar deviation and wrist extension.
Imaging
- Standard Radiographs: Posteroanterior (PA), lateral, and oblique views of the wrist. Look for scalloping or sclerosis on the ulnar aspect of the distal radius, which is a hallmark of chronic radioulnar impingement.
- Dynamic Views: Grip-loaded PA views can accentuate radioulnar convergence, demonstrating the dynamic nature of the instability.
- Advanced Imaging: MRI or CT may be utilized to assess the quality of the soft tissues (ECU, PQ) and to rule out other sources of ulnar-sided wrist pain, such as residual TFCC pathology or ulnocarpal abutment.
Surgical Technique: Kleinman and Greenberg Procedure
Patient Positioning and Preparation
- Place the patient in the supine position on the operating table.
- Extend the operative arm onto a well-padded radiolucent hand table.
- Apply a well-padded pneumatic tourniquet to the proximal arm.
- Sit on the cephalad side of the hand table. This position allows optimal ergonomic access to the ulnar aspect of the wrist.
- Pronate the patient’s forearm for ease of access to the ulnar side of the forearm and wrist.
- Prepare the skin with standard surgical solutions and apply sterile drapes to the hand and arm, ensuring the elbow and wrist can be freely manipulated.
- Exsanguinate the extremity using an Esmarch bandage and inflate the tourniquet to the appropriate pressure (typically 250 mm Hg or 100 mm Hg above systolic blood pressure).
Step 1: Incision and Exposure
Make a curvilinear dorsoulnar skin incision at the wrist level. The incision should be centered over the distal ulna, allowing access to both the dorsal and palmar aspects of the ulnar stump.
Figure 1: The planned curvilinear dorsal skin incision over the distal ulna.
Extend the incision proximally along the distal ulnar shaft.
🚨 Surgical Warning: The Dorsal Sensory Branch of the Ulnar Nerve (DSBUN)
Extreme caution must be exercised during the superficial dissection. The dorsal sensory branch of the ulnar nerve (DSBUN) crosses from palmar to dorsal around the ulnar neck approximately 5 cm proximal to the ulnar styloid. Injury to this nerve will result in a painful neuroma that can completely negate the functional benefits of the surgery. Identify, mobilize, and protect the DSBUN with a vessel loop early in the dissection.
Approach the ulna through the internervous plane between the extensor carpi ulnaris (ECU, innervated by the posterior interosseous nerve) and the flexor carpi ulnaris (FCU, innervated by the ulnar nerve).
If additional palmar exposure is required to adequately mobilize the pronator quadratus, a supplementary palmar incision can be utilized, though the procedure can often be completed through a single extensile dorsoulnar approach.

Figure 2: Optional palmar skin incision for extended access to the pronator quadratus.
Step 2: Preparation of the Ulnar Stump
- Identify and expose the distal end of the previous Darrach resection of the distal ulna. The stump is often encased in dense scar tissue and may exhibit osteophytic spurring due to chronic impingement against the radius.
- Carefully perform a subperiosteal dissection to free the distal 2 to 3 cm of the ulnar stump.
- Contour the distal end of the ulna with a high-speed burr or a rongeur as needed. The goal is to create a smooth, rounded stump that will not abrade the transferred soft tissues or the adjacent radius. Remove any sharp cortical edges.
Step 3: Pronator Quadratus Mobilization and Transfer
- Identify the pronator quadratus muscle on the palmar aspect of the distal forearm.
- Dissect the pronator quadratus free from its palmar-medial attachment to the ulna. This requires meticulous elevation to preserve the muscle's integrity and its neurovascular pedicle (anterior interosseous nerve and artery), which enters the muscle on its deep, radial aspect.
- Mobilize the pronator quadratus radially. The muscle flap is then passed through the interosseous space or draped over the contoured ulnar stump.
- The transferred PQ acts as an interpositional arthroplasty, cushioning the space between the radius and ulna, while its new vector of pull actively retards dorsal translation ("winging") of the ulna during forearm rotation.
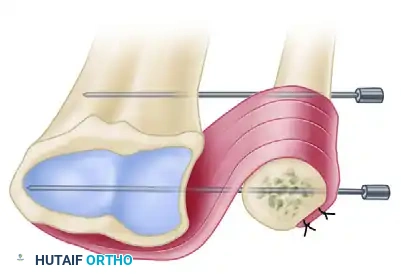
Figure 3: The pronator quadratus is mobilized and transferred to stabilize the distal ulnar stump, often secured with temporary K-wire fixation to maintain the radioulnar interval during healing.
Step 4: ECU Tenodesis and Sling Creation
The ECU is located within the sixth dorsal compartment. To prevent radioulnar impingement, the ECU is utilized to tether the ulnar stump.
- Open the sixth dorsal compartment longitudinally, preserving the extensor retinaculum.
- Sling Technique: A sling can be created from a strip of the extensor retinaculum to stabilize the ECU tendon over the dorsal aspect of the ulna, preventing it from subluxating palmarward and utilizing its tension to hold the ulna dorsally and ulnarly.
Figure 4: The Extensor Carpi Ulnaris (ECU) stabilized by a robust sling created from the extensor retinaculum.
- Formal Tenodesis Technique: Alternatively, a distally based strip of the ECU tendon (approximately half its width) is harvested.
- Drill a transverse hole through the distal ulnar stump.
- Pass the harvested ECU tendon strip through the drill hole in the ulna.
- Tension the tendon strip with the forearm in neutral rotation and the wrist in slight extension. Suture the tendon back onto itself or to the adjacent periosteum using non-absorbable braided sutures (e.g., 2-0 Ethibond or FiberWire). This tenodesis creates a powerful checkrein that retards radioulnar convergence.
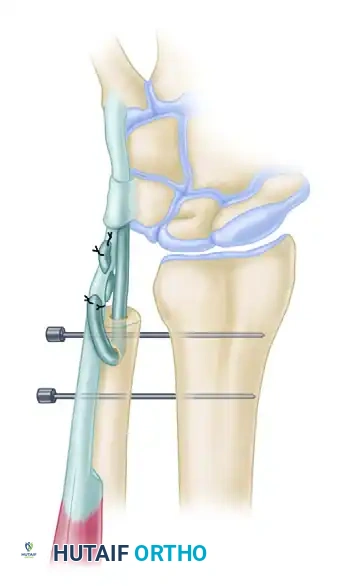
Figure 5: Formal ECU tenodesis. A strip of the ECU is passed through a drill hole in the contoured ulnar stump and sutured to itself. Note the temporary transverse K-wires maintaining the radioulnar space.
Step 5: Temporary Osseous Stabilization
To protect the soft-tissue transfers while they heal, the radioulnar relationship must be rigidly maintained postoperatively.
- Position the forearm in neutral to slight supination (the position of maximum DRUJ stability).
- Manually reduce the ulnar stump to ensure an adequate radioulnar space (preventing convergence) and correct dorsal-palmar alignment.
- Drive two smooth 0.062-inch (1.6 mm) Kirschner wires (K-wires) transversely from the ulna into the radius. Ensure the wires engage both cortices of the radius for maximum stability.
- Cut the K-wires beneath the skin to prevent pin-tract infections, or leave them protruding through the skin with protective caps, depending on surgeon preference and patient reliability.
- Deflate the tourniquet, achieve meticulous hemostasis, and close the subcutaneous tissues and skin in layers.
- Apply a sterile dressing and a well-padded long-arm sugar-tong splint or cast with the forearm in neutral to slight supination and the wrist in neutral.
Postoperative Protocol and Rehabilitation
The success of the ECU tenodesis and PQ transfer relies heavily on strict adherence to the postoperative rehabilitation protocol. Premature mobilization will lead to stretching or rupture of the soft-tissue transfers, resulting in recurrent instability.
Phase 1: Immobilization (Weeks 0 to 6)
- The patient remains in a long-arm cast or rigid sugar-tong splint.
- The forearm is maintained in neutral to slight supination.
- Digital range of motion (ROM) exercises are initiated immediately to prevent tendon adhesions and reduce edema.
- Shoulder and elbow ROM (within the confines of the cast) are encouraged.
Phase 2: Pin Removal and Early Motion (Weeks 6 to 8)
- At 6 weeks postoperatively, radiographs are obtained to confirm maintenance of the radioulnar interval.
- The transverse radioulnar K-wires are removed in the clinic.
- The patient is transitioned to a short-arm Muenster-style splint or a custom thermoplastic wrist splint that limits extremes of forearm rotation but allows wrist flexion and extension.
- Active and active-assisted forearm pronation and supination are initiated under the guidance of a certified hand therapist.
Phase 3: Strengthening and Return to Function (Weeks 8 to 12+)
- At 8 weeks, the splint is gradually weaned for daily activities.
- Progressive strengthening exercises for grip, wrist extension/flexion, and forearm rotation are introduced.
- Heavy lifting, power gripping, and forceful rotational activities are restricted until at least 12 weeks postoperatively.
- Maximum medical improvement and final functional outcomes are typically realized between 6 and 9 months post-surgery.
Complications and Pitfalls
While highly effective, the Kleinman and Greenberg procedure is technically demanding and carries specific risks:
- Neuroma Formation: As emphasized, injury to the dorsal sensory branch of the ulnar nerve is the most devastating complication. Meticulous dissection and protection are mandatory.
- Recurrent Instability: Failure to adequately tension the ECU tenodesis, failure to secure the PQ transfer, or premature postoperative mobilization can lead to stretching of the reconstruction and recurrent radioulnar impingement.
- Loss of Forearm Rotation: Over-tensioning the ECU tenodesis or prolonged K-wire fixation can result in severe stiffness and loss of pronation/supination. The K-wires must be placed with the forearm in a neutral position, not in extreme supination, to balance the soft tissues.
- Pin-Tract Infection: If K-wires are left percutaneous, meticulous pin care is required. Deep infection may necessitate premature pin removal, jeopardizing the soft-tissue repair.
- Ulnar Stump Fracture: Drilling holes that are too large or placed too close to the cortical edge of the contoured ulnar stump can create a stress riser, leading to fracture during the tenodesis or postoperatively.
Conclusion
The Kleinman and Greenberg technique of ECU tenodesis combined with pronator quadratus transfer is a masterclass in applied biomechanics. By addressing both the transverse convergence and the dorsal translation of the unstable distal ulnar stump, this procedure offers a durable, biologic salvage for the failed Darrach resection. For the active patient where silicone implants are destined to fail, meticulous execution of this soft-tissue reconstruction restores stability, alleviates pain, and significantly improves upper extremity function.
You Might Also Like


