Anatomical Graft Reconstruction of the Thumb Ulnar Collateral Ligament
Key Takeaway
Anatomical graft reconstruction of the thumb metacarpophalangeal (MCP) joint ulnar collateral ligament (UCL) is the gold standard for chronic instability where primary repair is unfeasible. This technique, popularized by Glickel, utilizes a free tendon autograft routed through precise osseous tunnels in the proximal phalanx and metacarpal head. It restores both the proper and accessory collateral ligaments, providing robust biomechanical stability while preserving functional joint kinematics and preventing long-term degenerative arthrosis.
INTRODUCTION TO CHRONIC UCL INSTABILITY
Ulnar collateral ligament (UCL) injuries of the thumb metacarpophalangeal (MCP) joint are among the most common ligamentous injuries in the upper extremity, frequently resulting from forced hyperabduction and extension (classically termed "Skier's thumb" or "Gamekeeper's thumb"). While acute injuries are often amenable to direct anatomical repair, chronic insufficiency—typically defined as presenting more than 6 weeks post-injury—presents a distinct surgical challenge.
In the chronic setting, the native ligament is often retracted, atrophic, or encased in dense fibrotic scar tissue, rendering primary repair biomechanically inadequate or entirely impossible. Furthermore, the presence of a Stener lesion (interposition of the adductor aponeurosis between the torn UCL and its insertion) guarantees non-healing and necessitates surgical intervention. For these chronic presentations, anatomical graft reconstruction, as popularized by Glickel et al., is the gold standard. This technique utilizes a free tendon autograft to anatomically recreate both the proper and accessory components of the UCL, restoring multi-planar stability and preventing the rapid onset of degenerative joint disease.
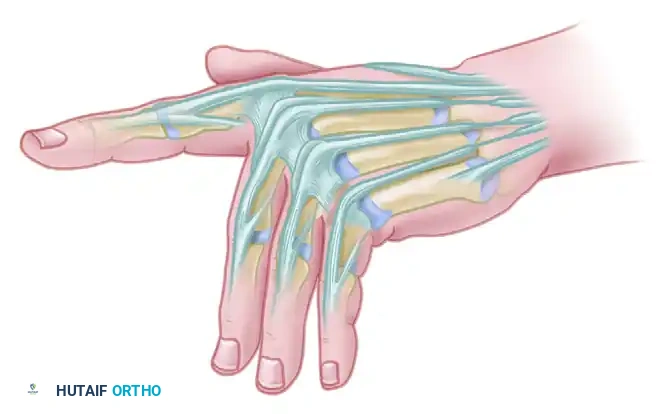
BIOMECHANICS AND SURGICAL ANATOMY
A profound understanding of thumb MCP joint kinematics is mandatory for successful reconstruction. The MCP joint is a diarthrodial condyloid joint with intrinsic stability provided by a complex capsuloligamentous box.
The Ulnar Collateral Ligament Complex
The UCL complex consists of two distinct functional bundles:
* Proper Ulnar Collateral Ligament (pUCL): Originates from the dorsal third of the metacarpal head and inserts onto the volar aspect of the proximal phalanx base. It is taut in flexion and is the primary restraint to valgus stress when the MCP joint is flexed at 30 degrees.
* Accessory Ulnar Collateral Ligament (aUCL): Originates volar to the pUCL and inserts onto the volar plate and sesamoid bones. It is taut in extension and provides primary valgus stability when the joint is fully extended.
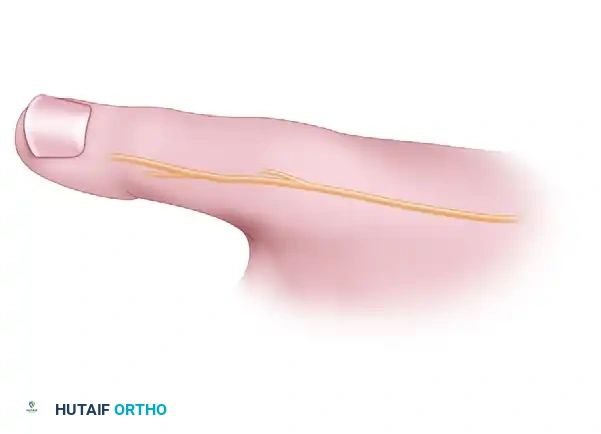
The Dorsal Sensory Branch of the Radial Nerve (SBRN)
The SBRN courses subcutaneously over the radial and dorsal aspects of the thumb. Its terminal branches are highly variable and exquisitely sensitive to traction or iatrogenic injury. Neuroma formation in this nerve is a devastating complication that can eclipse the functional benefits of a successful ligament reconstruction.
Surgical Warning: The SBRN must be identified early, mobilized gently, and protected throughout the procedure. Avoid aggressive retraction, as neuropraxia can lead to debilitating complex regional pain syndrome (CRPS).
INDICATIONS AND CONTRAINDICATIONS
Indications
- Chronic symptomatic UCL instability (>6 weeks post-injury).
- Failed primary repair of the UCL.
- Acute injuries with severe mid-substance tissue loss or profound tissue attenuation precluding robust primary repair.
- Symptomatic valgus laxity >30 degrees in both flexion and extension, or >15 degrees of asymmetry compared to the contralateral uninjured thumb.
Contraindications
- Absolute: Advanced osteoarthritis of the thumb MCP joint. In the presence of significant degenerative changes (cartilage loss, osteophyte formation), ligament reconstruction will fail to relieve pain and may exacerbate stiffness. Arthrodesis is the procedure of choice in this scenario.
- Relative: Poor soft tissue envelope, active infection, or patient inability to comply with strict postoperative rehabilitation protocols.
PREOPERATIVE PLANNING AND PATIENT POSITIONING
Imaging
Standard posteroanterior (PA), lateral, and Robert's view radiographs of the thumb are mandatory to assess for avulsion fractures, joint subluxation, and degenerative arthrosis. Stress radiographs can quantify the degree of instability but are often unnecessary if clinical laxity is profound.
Anesthesia and Positioning
- Anesthesia: Regional block (axillary or supraclavicular brachial plexus block) combined with monitored anesthesia care (MAC) or general anesthesia.
- Positioning: The patient is positioned supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A well-padded upper arm pneumatic tourniquet is applied and inflated to 250 mm Hg after exsanguination with an Esmarch bandage.
- Equipment: Mini-C-arm fluoroscopy should be available in the surgical field.
SURGICAL TECHNIQUE: ANATOMICAL GRAFT RECONSTRUCTION (GLICKEL)
The following technique details the anatomical reconstruction utilizing a free tendon graft to recreate the native footprint of the UCL complex.
1. Surgical Approach and Nerve Protection
Expose the thumb metacarpophalangeal joint through a mid-axial or lazy-S incision centered over the ulnar joint line. The incision should allow adequate proximal and distal extension without crossing flexion creases at a perpendicular angle.
Carefully dissect through the subcutaneous tissues. The immediate priority is to isolate and protect the terminal branches of the radial nerve dorsal sensory branch (SBRN). Use blunt dissection and vessel loops to gently retract the nerve branches out of the surgical field.
FIGURE A: The mid-axial or lazy-S incision centered over the MCP joint, demonstrating the critical subcutaneous branches of the radial nerve that must be protected.
2. Extensor Mechanism Management
Once the soft tissue envelope is managed, identify the adductor aponeurosis and the extensor mechanism.
* Save the extensor mechanism sagittal band fibers.
* Release the extensor mechanism oblique fibers from the extensor pollicis longus (EPL) longitudinally, and vertically from the sagittal band proximally.
* This specific release leaves a triangular section of the extensor mechanism that can be reflected palmarward, providing excellent exposure of the underlying joint capsule and ligamentous remnants.
3. Joint Preparation and Assessment
Retract the sagittal band proximally to fully expose the base of the proximal phalanx and the metacarpophalangeal joint.
* Identify and excise the fibrotic, non-functional ulnar collateral ligament stumps.
* Perform a thorough arthrotomy to evaluate the articular cartilage.
Clinical Pearl: Direct visualization of the articular surface is a critical decision-making step. Note if significant degenerative changes are present. If full-thickness cartilage loss or severe osteophytosis is identified, abort the reconstruction and convert to an MCP joint arthrodesis.
4. Phalangeal Bone Tunnel Preparation
To anatomically recreate the UCL footprint on the proximal phalanx, two osseous tunnels are created.
* Make gouge holes in the ulnar base of the proximal phalanx.
* Place the first hole in the palmar aspect (the 7-o’clock position for a right thumb, or 5-o'clock for a left thumb).
* Place the second hole more dorsally (the 11-o’clock position for a right thumb, or 1-o'clock for a left thumb), just distal to the articular joint surface.
* Carefully connect these two holes using a small curette or burr, ensuring that a robust cortical bone bridge is preserved between them. This bridge will act as the distal fixation point for the tendon graft.
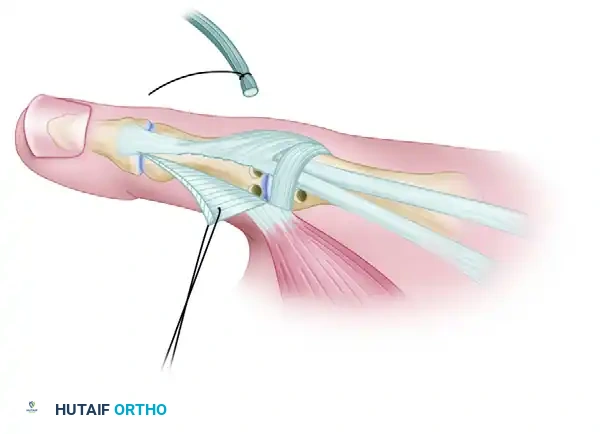
FIGURE B: Two gouge holes made on the ulnar side of the proximal phalangeal base (7-o'clock and 11-o'clock positions) connected to form a tunnel, preserving the cortical bone bridge.
5. Metacarpal Bone Tunnel Preparation
The metacarpal tunnel must replicate the isometric origin of the UCL.
* Identify the anatomical ligament fossa on the ulnar aspect of the metacarpal head.
* Make a hole in this fossa and direct the drill or gouge across the metacarpal head, aiming radially and slightly proximally to exit the radial cortex of the metacarpal neck.
* Make a separate 5-mm counter-incision over this radial exit site to facilitate tendon passage and eventual fixation.
6. Graft Harvest
A free tendon autograft is required. The palmaris longus (PL) is the graft of choice due to its expendability and ideal diameter. If the PL is absent, a strip of the flexor carpi radialis (FCR) or a slip of the abductor pollicis longus (APL) may be utilized. Harvest the graft using standard minimally invasive tendon stripper techniques, ensuring a minimum length of 10 to 12 cm.
7. Graft Passage and Fixation
Passage of the graft must be meticulous to ensure appropriate tensioning and anatomical routing.
* Pass the harvested tendon graft through the connected holes in the proximal phalangeal base. This can be facilitated using a stainless steel wire loop, a suture shuttle, or a small curved needle.
* Prior to passing the graft through the metacarpal, place a transarticular Kirschner wire (K-wire) across the MCP joint to hold it in slight flexion and slight ulnar deviation (overcorrecting the valgus deformity). Ensure this K-wire is placed centrally so as not to obstruct the metacarpal head tunnel.
* Pass the two free limbs of the tendon graft under the sagittal band.
* Shuttle both limbs through the ulnar-to-radial metacarpal neck tunnel so they exit through the radial counter-incision.
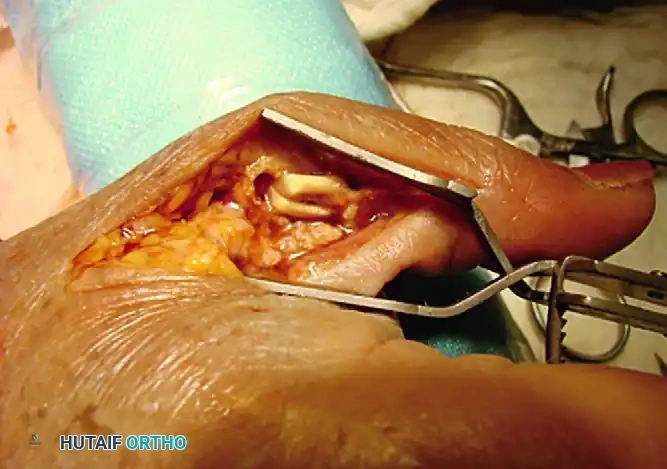
FIGURE C: Initial passage of the tendon graft through the proximal phalanx bone bridge.
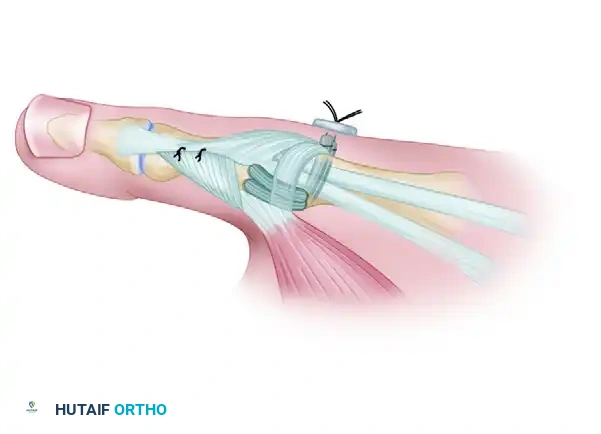
FIGURE D: Intraoperative view demonstrating the tendon graft routed through the osseous tunnels prior to final tensioning.
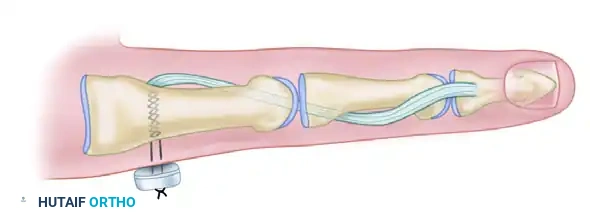
8. Tensioning and Final Fixation
- Take tension off the graft by slightly overcorrecting the joint reduction. Ensure any palmar subluxation of the proximal phalanx is fully reduced.
- With the joint pinned in the optimized position, apply firm, equal tension to both limbs of the graft exiting the radial metacarpal cortex.
- Fix the graft on the radial side. This can be achieved by suturing the graft limbs to the adjacent periosteum, tying them over a sterile surgical button on the radial cortex, or utilizing a modern biotenodesis screw if the tunnel diameter permits.

FIGURE E: Final passage and fixation of the tendon graft. The limbs are tensioned and secured over the radial cortex, restoring the anatomical footprint of the UCL.
9. Closure
- Repair the adductor aponeurosis and the reflected triangular section of the extensor mechanism using non-absorbable or slowly absorbable sutures (e.g., 4-0 Ethibond or PDS).
- Deflate the tourniquet, achieve meticulous hemostasis, and close the skin with interrupted non-absorbable sutures (e.g., 5-0 Nylon).
- Apply a sterile dressing and a rigid, well-molded thumb spica splint.
POSTOPERATIVE REHABILITATION PROTOCOL
The success of an anatomical graft reconstruction relies heavily on strict adherence to a phased postoperative rehabilitation protocol to balance graft healing with the prevention of joint stiffness.
Phase I: Immobilization (Weeks 0-4)
- The thumb is immobilized in a rigid cast or custom thermoplastic thumb spica splint.
- The interphalangeal (IP) joint is left free to prevent extensor tendon adhesions.
- The transarticular K-wire remains in place to protect the graft during the initial phase of biological incorporation.
Phase II: Early Mobilization (Weeks 4-6)
- At 4 weeks postoperatively, the transarticular K-wire is removed in the clinic.
- The patient is transitioned to a removable custom thumb spica orthosis.
- Active range of motion (AROM) exercises for the MCP joint are initiated under the guidance of a certified hand therapist.
- Passive range of motion (PROM) and any valgus stress are strictly prohibited.
Phase III: Strengthening (Weeks 6-10)
- Wean the patient from the daytime splint, though night splinting may continue until week 8.
- Initiate gentle passive stretching and progressive strengthening exercises (e.g., putty squeezing, pinch grip training).
- Avoid heavy lifting or forceful pinch activities.
Phase IV: Return to Activity (Weeks 10-12+)
- Unrestricted activities are generally permitted by 12 weeks.
- For contact athletes or heavy manual laborers, a protective taping or a soft functional brace may be recommended during high-risk activities for up to 6 months postoperatively.
COMPLICATIONS AND PITFALLS
While highly successful, the Glickel anatomical reconstruction carries specific risks that the operating surgeon must anticipate and mitigate.
- Radial Sensory Nerve Injury: The most debilitating complication. Meticulous dissection and avoidance of aggressive retraction are paramount. If a neuroma develops, it may require surgical excision and nerve burying.
- Bone Tunnel Blowout: Occurs if the gouge holes in the proximal phalanx are placed too close together or too close to the articular surface. Prevention: Ensure a minimum 3-4 mm cortical bridge. If blowout occurs, alternative fixation (e.g., suture anchors) must be utilized.
- Joint Stiffness: Some loss of terminal flexion is common and often an acceptable trade-off for a stable joint. Prolonged immobilization beyond 4 weeks significantly increases the risk of severe stiffness.
- Recurrent Instability: Usually results from inadequate graft tensioning, premature removal of the K-wire, or patient non-compliance with the postoperative protocol.
- Progression of Osteoarthritis: If subtle degenerative changes were missed preoperatively, the altered kinematics of a reconstructed joint can accelerate arthrosis, eventually necessitating arthrodesis.
CONCLUSION
The anatomical graft reconstruction of the thumb UCL is a highly durable and biomechanically sound procedure for chronic instability. By meticulously recreating the native footprints of the proper and accessory ligaments using a free tendon autograft, surgeons can restore pinch strength, eliminate pain, and halt the progression of degenerative joint disease. Mastery of the surgical anatomy, precise tunnel placement, and rigorous postoperative rehabilitation are the cornerstones of achieving excellent, long-lasting clinical outcomes.
You Might Also Like