Calcaneal Osteotomy: Dwyer & Crescentic Techniques

Key Takeaway
Calcaneal osteotomies, including the Dwyer lateral closing wedge and Samilson crescentic techniques, are powerful procedures for correcting complex hindfoot deformities such as cavovarus and calcaneocavus. This comprehensive surgical guide details the biomechanical principles, precise operative steps, and postoperative protocols required to achieve optimal multiplanar correction, restore plantigrade alignment, and mitigate complications in both neurogenic and traumatic foot deformities.
OSTEOTOMY OF THE CALCANEUS: PRINCIPLES AND BIOMECHANICS
The calcaneus is the foundational osseous structure of the hindfoot, dictating the alignment, biomechanics, and force transmission of the entire lower extremity during the gait cycle. Malalignment of the calcaneus—whether in varus, valgus, or severe cavus—profoundly alters the biomechanics of the subtalar and transverse tarsal joints. Calcaneal osteotomies are powerful, joint-sparing procedures designed to extra-articularly realign the mechanical axis of the hindfoot, thereby preserving subtalar motion while restoring a plantigrade foot.
Surgical intervention is primarily indicated for complex, multiplanar deformities such as the cavovarus foot (frequently seen in Charcot-Marie-Tooth disease) and the calcaneocavus foot (often a sequela of poliomyelitis or isolated triceps surae weakness). The two most historically significant and biomechanically sound extra-articular calcaneal osteotomies are the Dwyer lateral closing wedge osteotomy for hindfoot varus and the Samilson crescentic osteotomy for calcaneocavus deformities.
Thorough preoperative clinical and radiographic evaluation is mandatory. The Coleman block test is essential to differentiate between a flexible, forefoot-driven hindfoot varus (which may resolve with a first metatarsal dorsiflexion osteotomy) and a rigid, fixed hindfoot varus (which necessitates a calcaneal osteotomy).
THE DWYER LATERAL CLOSING WEDGE OSTEOTOMY
The Dwyer osteotomy is a lateral closing wedge osteotomy of the calcaneal tuberosity. It is specifically designed to correct fixed hindfoot varus by resecting a laterally based wedge of bone, thereby translating and angulating the calcaneal tuberosity into a neutral or slightly valgus position.
Indications and Preoperative Planning
The primary indication for a Dwyer osteotomy is a rigid hindfoot varus deformity. This is most commonly encountered in neurogenic cavovarus feet (e.g., Charcot-Marie-Tooth disease, Friedreich’s ataxia) or as a late complication of clubfoot overcorrection or trauma.
Clinical Pearl: The Dwyer procedure is highly effective at correcting coronal plane varus but offers limited correction of sagittal plane deformities. If severe multiplanar deformity exists, the Dwyer osteotomy must be combined with midfoot osteotomies, plantar fascia release, or tendon transfers (e.g., peroneus longus to brevis transfer).
🔪 Surgical Technique (Dwyer)
1. Plantar Fascia Release
The procedure frequently begins with a release of the plantar fascia. Divide the plantar fascia subcutaneously or through a small medial incision to reduce the drop of the forefoot and release the tethering effect on the medial longitudinal arch.
2. Incision and Exposure
Place the patient in the lateral decubitus position or supine with a large bump under the ipsilateral hip to internally rotate the leg.
- Expose the lateral aspect of the calcaneus through a curved incision paralleling the peroneus longus tendon, maintaining a distance of approximately 1 cm posterior and inferior to it.
- Meticulous dissection is required to avoid injury to the sural nerve, which courses in proximity to the surgical field.
- Turn the entire fasciocutaneous flap anteriorly until the tendon of the peroneus longus muscle is fully exposed.
- Strip the periosteum from the superior, lateral, and inferior surfaces of the calcaneus using a Cobb elevator, ensuring adequate exposure for the osteotomy cuts.
3. Execution of the Osteotomy
- Remove a laterally based wedge of bone from the calcaneus just inferior and posterior to the peroneus longus tendon, keeping the cuts parallel with the tendon's course.
- Make the base of the lateral wedge 8 to 12 mm wide, depending on the severity of the varus deformity.
- Taper the wedge medially to, but not through, the medial cortex. Preserving the medial periosteal hinge is critical for stability and to act as a fulcrum for closure.
4. Deformity Correction and Closure
- Carefully break the medial cortex using a greenstick fracture technique.
- Close the osteotomy gap; bring the bony surfaces snugly together by pressing the forefoot into dorsiflexion against the pull of the Achilles tendon.

Surgical Warning: Failure to obtain complete closure of the lateral gap is almost always caused by a small, retained piece of bone left behind at the medial apex of the wedge. Use a small curette or rongeur to clear the apex if resistance is met.
- Ensure that the varus deformity has been completely corrected and that the heel rests in a neutral or slightly valgus position. Failure to correct the varus deformity completely will inevitably lead to a recurrence or exacerbation of the deformity over time.
5. Fixation and Closure
- While Dwyer originally described the procedure without internal fixation, modern techniques highly recommend securing the osteotomy with one or two large-fragment cannulated screws (6.5 mm or 7.3 mm) or a dedicated calcaneal step-plate to prevent displacement.
- Close the wound in layers over a closed suction drain if necessary.
MANAGEMENT OF COMBINED CAVUS AND COMPLEX DEFORMITIES
Pathoanatomy of the Cavovarus Foot
In patients with Charcot-Marie-Tooth (CMT) disease, the cavovarus deformity is typically driven by a plantarflexed first ray (due to peroneus longus overpowering the tibialis anterior). Over time, this flexible forefoot pronation drives the hindfoot into a rigid compensatory varus.
While a Dwyer osteotomy can partially correct the varus and calcaneus posture of the hindfoot, it cannot correct midfoot or forefoot cavus. Therefore, a concomitant dorsal closing wedge osteotomy at the base of the first metatarsal is frequently required.
Initial small wedge (3 to 4 mm) is resected from the base of the first metatarsal.

The wedge is increased as necessary to bring the first metatarsal to a plantigrade position post-osteotomy.
Triple Arthrodesis for Severe, Fixed Deformities
Although joint-sparing osteotomies are preferred, severe, fixed equinocavovarus deformities—especially those with arthritic changes in the talonavicular or calcaneocuboid joints—are best managed with a triple arthrodesis. This allows for multiplanar correction and concomitant management of claw toe deformities.
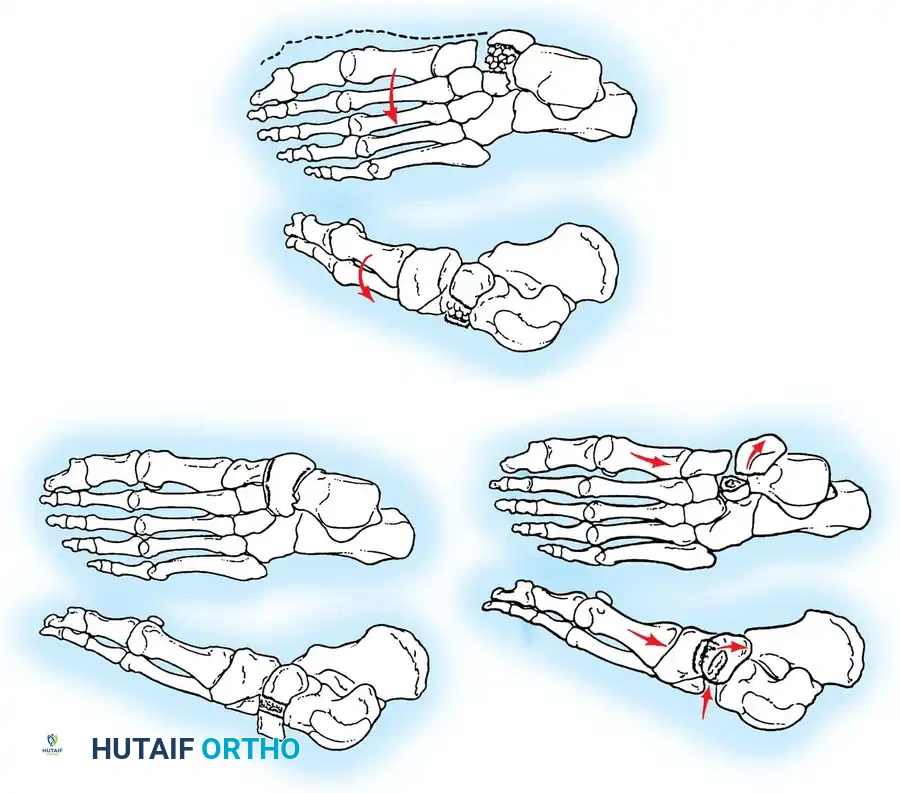
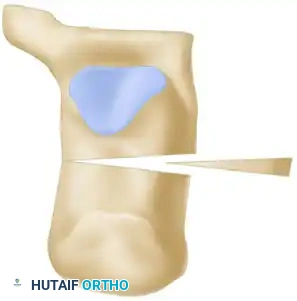
When performing a triple arthrodesis for a severe varus deformity, precise biplanar wedge resections are required:

A, Wedge with its base lateral (colored area) is resected from the midtarsal region to correct the adduction and cavus deformity of the forefoot.

B, Wedge with its base lateral (colored area) is resected from the subtalar region to correct the varus deformity of the hindfoot.



C and D, Position of the bones after surgery, demonstrating a restored plantigrade alignment and neutral hindfoot.
Traumatic Cavovarus and the Reverse Evans Osteotomy
In traumatic cavovarus feet characterized by forefoot adduction and supination, but with radiographically intact talonavicular and calcaneocuboid joints, a subtalar arthrodesis combined with a lateral closing wedge (7 to 10 mm) osteotomy of the anterior aspect of the calcaneus (1 cm proximal to the calcaneocuboid joint) may be indicated. This is known as a reverse Evans osteotomy. It corrects the lateral column overlength and hindfoot varus while preserving midtarsal motion.
CRESCENTIC CALCANEAL OSTEOTOMY (SAMILSON TECHNIQUE)
The calcaneocavus deformity is characterized by a steeply pitched calcaneus (increased calcaneal pitch angle) and a high longitudinal arch. It is most frequently seen in patients with poliomyelitis or isolated weakness of the triceps surae, leading to unopposed dorsiflexion and subsequent verticalization of the calcaneus.
Samilson recommended the crescentic calcaneal osteotomy for ambulatory patients with symptomatic calcaneocavus feet.
Indications and Biomechanics
The indications for an isolated crescentic calcaneal osteotomy are rare. On a lateral radiograph, the calcaneus must be relatively vertical, and the apex of the cavus must be located posterior to the midtarsus.
Surgical Pitfall: The Samilson operation does not correct midtarsal or forefoot cavus. It is strictly designed to correct hindfoot cavus (calcaneocavus) by translating the posterior tuberosity superiorly and posteriorly, thereby flattening the calcaneal pitch and restoring the lever arm of the Achilles tendon.
🔪 Surgical Technique (Samilson)
1. Positioning and Incision
- Operate under pneumatic tourniquet control. After preparation and draping in the usual sterile manner, position the patient in the lateral decubitus position.
- Make an obliquely placed lateral incision over the posterior tuberosity of the calcaneus, posterior to the subtalar joint.
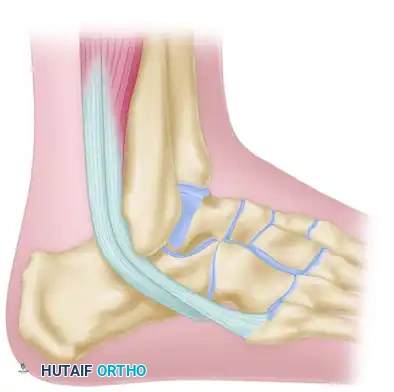
A, The oblique lateral incision is planned posterior to the subtalar joint and peroneal tendons.
2. Deep Dissection
- Ensure the peroneal tendons remain anterior to the posterior portion of the incision. Retract them gently to avoid tenosynovitis or iatrogenic subluxation.
- Carry the dissection down through the subcutaneous tissues to the lateral aspect of the calcaneus.
B, Exposure of the lateral calcaneal wall, preparing for the crescentic cut.
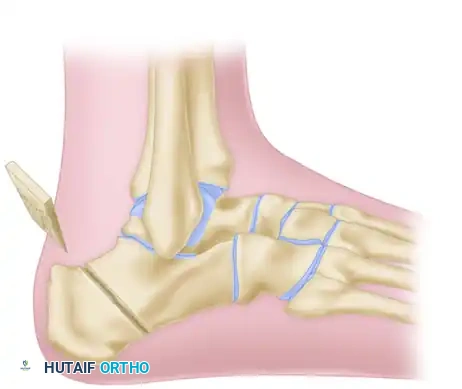
3. The Crescentic Osteotomy
- Using a crescentic saw blade, initiate the osteotomy posterior to the posterior facet of the subtalar joint. The concavity of the cut should face posteriorly and inferiorly.
C, The crescentic osteotomy is executed, ensuring the subtalar joint is not violated.
4. Displacement and Correction
- Once the osteotomy is complete through both the lateral and medial cortices, mobilize the posterior tuberosity fragment.
- Slide the posterior fragment superiorly and posteriorly along the crescentic arc. This maneuver decreases the calcaneal pitch angle and effectively lengthens the posterior lever arm of the heel.

D, The posterior tuberosity is displaced superiorly along the crescentic path to correct the calcaneocavus deformity.
5. Fixation
- Secure the osteotomy with rigid internal fixation. Typically, one or two large-fragment cannulated screws are directed from the posterior-inferior tuberosity into the anterior calcaneal body.
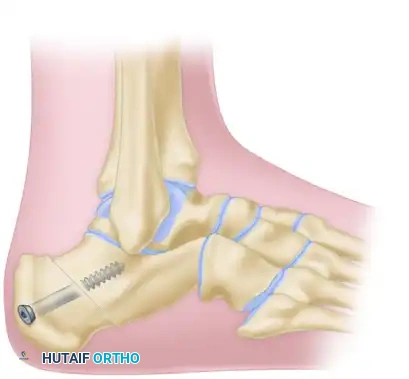
E, Final rigid internal fixation of the Samilson crescentic osteotomy.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Regardless of whether a Dwyer or Samilson osteotomy is performed, strict adherence to postoperative immobilization is critical to ensure osseous union and prevent displacement.
- Phase I (0-2 Weeks): The foot is immobilized in a well-padded, short-leg splint in a neutral position. The patient is strictly non-weight-bearing (NWB). Elevation is paramount to control edema and protect the lateral wound, which is prone to dehiscence.
- Phase II (2-6 Weeks): Sutures are removed at 2 weeks assuming the incision is fully healed. The patient is transitioned to a short-leg fiberglass cast or a rigid CAM boot, remaining strictly NWB.
- Phase III (6-10 Weeks): Radiographs are obtained at 6 weeks. If bridging callus and obliteration of the osteotomy line are visible, the patient may begin progressive partial weight-bearing in a CAM boot. Physical therapy is initiated to restore ankle and subtalar range of motion.
- Phase IV (10+ Weeks): Transition to regular footwear with supportive orthotics. Full athletic activity is generally restricted until 4 to 6 months postoperatively, depending on the return of triceps surae strength and complete radiographic union.
COMPLICATIONS AND SURGICAL PITFALLS
- Sural Nerve Injury: The sural nerve is highly vulnerable during the lateral approach to the calcaneus. It must be identified, mobilized, and protected throughout the procedure. Neuroma formation here is highly symptomatic and difficult to treat.
- Undercorrection: In the Dwyer procedure, undercorrection occurs if the medial cortex is not adequately hinged or if bone debris is left at the apex of the wedge. Always assess hindfoot alignment intraoperatively with a simulated weight-bearing view (axial heel view).
- Wound Dehiscence: The lateral skin over the calcaneus has a tenuous blood supply. Excessive retraction, thick flaps, or early weight-bearing can lead to skin necrosis and deep infection.
- Nonunion: While rare in the highly vascular cancellous bone of the calcaneus, nonunion can occur if the osteotomy is inadequately stabilized or if the patient is non-compliant with weight-bearing restrictions. Rigid internal fixation significantly mitigates this risk.
📚 Medical References
You Might Also Like