Nail Unit Injuries: Advanced Orthopedic Management & Repair Decisions
Key Takeaway
Surgical repair for nail unit injuries isn't always required. The decision is multifaceted, balancing injury severity against intervention benefits. Meticulous anatomical restoration, particularly of the germinal matrix, is crucial to prevent permanent deformity and functional impairment. Judicious patient selection guides optimal operative versus non-operative management for best outcomes.
Introduction and Epidemiology
Trauma to the digital tip, particularly involving the nail unit, is a ubiquitous presentation in orthopedic practice. While seemingly superficial, these injuries, if inadequately managed, can lead to persistent pain, functional impairment, and significant cosmetic disfigurement. The nail unit is an intricate appendage serving crucial roles in digital protection, tactile discrimination, and precision grip. Thus, precise anatomical restoration is paramount for optimal outcomes.
Epidemiologically, distal phalangeal and nail unit injuries account for a substantial proportion of hand and foot trauma, with crush injuries being a predominant mechanism. Common scenarios include door crush injuries, industrial accidents, and sports-related trauma. Lacerations from sharp objects, avulsions, and punctures also contribute significantly to the injury burden. The decision regarding surgical intervention for nail unit injuries, particularly whether formal repair of the nail bed is indicated, represents a critical aspect of management that warrants a thorough understanding of relevant anatomy, biomechanics, and evidence-based principles. The core tenet of treatment is to minimize deformity, prevent infection, and restore the nail's natural growth pattern and adherence to the underlying matrix. The prevalence of these injuries, particularly in pediatric and active adult populations, underscores the need for a standardized, expert approach to ensure long-term digital health and function. Unrecognized or poorly treated nail bed lacerations, matrix avulsions, or associated distal phalangeal fractures are common precursors to debilitating sequelae such as split nails, non-adherent nails, or chronic pain, highlighting the necessity for accurate diagnosis and meticulous repair.
Surgical Anatomy and Biomechanics
A detailed understanding of the complex microanatomy and biomechanical function of the nail unit is fundamental for successful surgical intervention and prediction of outcomes. The nail unit is far more than a simple keratinized plate; it is a highly specialized mucocutaneous appendage.
Gross Anatomy of the Nail Unit
The nail unit is comprised of several distinct, yet interdependent, structures:
-
Nail Plate: The visible, semi-translucent, keratinized structure that provides protection to the distal phalanx and acts as a counterforce for the pulp, aiding in precision gripping and fine motor tasks. It is formed by the germinal matrix.
-
Nail Bed: This is further subdivided:
- Germinal Matrix (Proximal Matrix): Located beneath the eponychium, this crescent-shaped, opaque white structure is responsible for producing approximately 90% of the nail plate volume. Its cells undergo rapid mitosis and keratinization. Injury to the germinal matrix often results in permanent nail deformities such as a split nail or an absent nail. The lunula, the whitish crescent visible at the proximal nail plate, represents the distal extent of the germinal matrix.
- Sterile Matrix (Distal Matrix): Extends from the lunula to the hyponychium. It is transparent and provides adherence to the nail plate, contributing to the remaining 10% of nail plate thickness and determining its shape and contour. Injury to the sterile matrix can lead to nail plate dystrophy, non-adherence, or onycholysis.
-
Eponychium (Proximal Nail Fold): A fold of skin that covers the proximal portion of the nail plate, forming a protective seal. The ventral surface of the eponychium contains the germinal matrix.
-
Paronychium (Lateral Nail Folds): Skin folds located on either side of the nail plate, contributing to its lateral stability and protection.
-
Hyponychium: The junction between the distal nail plate and the volar skin of the fingertip, acting as a natural barrier against infection.
Microvasculature and Innervation
The nail unit boasts a remarkably rich vascular supply, originating primarily from the two proper digital arteries which form an elaborate arcade proximally, distal to the distal interphalangeal joint. These vessels anastomose to form a dorsal and a volar arch, supplying dense capillary networks throughout the germinal and sterile matrices. This robust vascularity contributes to the high metabolic demands of nail growth and often results in significant hemorrhage with trauma. Venous drainage parallels the arterial supply.
Innervation is provided by the dorsal and volar branches of the proper digital nerves. The volar digital nerves supply the nail bed, pulp, and volar skin, while the dorsal digital nerves supply the eponychium, paronychium, and dorsal skin. This intricate neurovascular network explains the exquisite sensitivity of the fingertip and the potential for persistent pain or paresthesia following injury.
Biomechanical Considerations
The nail unit, in conjunction with the distal phalanx and fingertip pulp, forms a critical functional complex. The rigid nail plate provides dorsal support, acting as a counterforce to the tactile pulp, which is essential for precision pinch, grip, and fine motor manipulation. Injuries that disrupt this counterforce mechanism, such as nail avulsion or distal phalangeal fracture malunion, can significantly impair hand function. The eponychial fold and paronychial folds create a sealed environment, protecting the underlying matrix from external pathogens. Loss of this protective barrier increases the risk of infection and chronic inflammatory conditions. Proper alignment and integrity of the germinal matrix are paramount, as even minor misalignments or scar tissue formation can lead to permanent structural and functional deformities of the growing nail.
Indications and Contraindications
The decision-making process for nail unit injuries requires a careful assessment of injury severity, patient factors, and potential outcomes. Surgical intervention is generally warranted for injuries that disrupt the structural integrity of the nail unit, threaten its function, or pose a risk for chronic deformity or infection.
Operative Indications
Operative management is indicated for injuries that typically involve significant nail bed damage, associated fractures, or compromise of the eponychial fold.
- Subungual Hematoma:
- Large, painful hematomas involving >50% of the nail plate. While simple trephination suffices for smaller, intact hematomas, larger collections often signify an underlying nail bed laceration, warranting nail plate removal and exploration.
- Hematomas with associated nail plate avulsion or disruption.
- Nail Bed Lacerations:
- Any laceration to the germinal or sterile matrix. These are primary indications for exploration and meticulous repair to prevent nail deformity.
- Stellate, complex, or avulsion lacerations where re-approximation is challenging.
- Nail Avulsion:
- Complete avulsion of the nail plate with underlying nail bed laceration or significant contamination.
- Avulsion of the nail unit from the eponychial fold.
- Distal Phalanx Fractures:
- Open fractures involving the nail unit, where the nail bed is compromised and requires repair or debridement.
- Displaced intra-articular fractures (Seymour fractures, P3 neck fractures) that threaten joint integrity or nail growth.
- Unstable transverse or comminuted tuft fractures with associated nail bed injury, potentially requiring stabilization.
- Eponychial Fold Lacerations:
- Lacerations that disrupt the protective seal and potentially involve the germinal matrix, requiring precise repair to prevent pterygium formation.
- Foreign Body:
- Retained foreign bodies within the nail unit or distal phalanx.
Non Operative Indications
Non-operative management is appropriate for stable injuries without significant structural disruption, or in cases where surgical intervention carries undue risk.
- Subungual Hematoma:
- Small, non-expanding, non-painful hematomas involving <50% of the nail plate with an intact nail plate and eponychial fold. Trephination via cautery or needle can provide symptomatic relief.
- Stable Distal Phalanx Fractures:
- Non-displaced tuft fractures without significant nail bed involvement.
- Closed, stable transverse shaft fractures without nail bed compromise.
- Simple Nail Avulsion:
- If the nail bed is entirely intact or minimally injured without laceration, and the nail plate is pristine and can be reimplanted as a biological splint.
- Minor Contusions:
- Without subungual hematoma or nail bed disruption.
Operative Versus Non Operative Indications Summary
| Operative Indications | Non-Operative Indications |
|---|---|
| Subungual hematoma > 50% nail plate, expanding, or painful | Subungual hematoma < 50% nail plate, non-expanding |
| Nail bed lacerations (germinal or sterile matrix) | Stable, non-displaced distal phalanx tuft fractures |
| Complete nail avulsion with nail bed injury | Simple nail avulsion with intact nail bed |
| Open distal phalanx fractures | Stable, closed distal phalanx fractures without nail bed injury |
| Displaced intra-articular distal phalanx fractures | Minor contusions to nail unit |
| Eponychial fold lacerations | |
| Retained foreign body in nail unit |
Contraindications to Surgical Repair
Absolute contraindications are rare and typically relate to the patient's overall health status rather than the injury itself. Relative contraindications include severe comorbidities precluding safe anesthesia, gross contamination with delayed presentation and established infection (requiring initial debridement and delayed definitive repair), or an unstable patient in a polytrauma setting where nail unit repair is not a life- or limb-threatening priority. Severely devitalized or extensively contaminated tissue may also contraindicate primary closure, necessitating staged debridement and delayed reconstruction.
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is crucial for optimizing outcomes in nail unit injuries, which often benefit from a precise, controlled surgical environment.
Preoperative Assessment
- History: Detailed history of the injury mechanism (crush, avulsion, laceration, blast), time of injury, hand dominance, occupation, patient comorbidities, vaccination status (tetanus prophylaxis). Inquire about previous finger injuries or deformities.
- Physical Examination:
- Neurovascular Status: Assess digital nerve function (two-point discrimination, sensation to light touch) and vascularity (capillary refill, digital artery pulsation, Doppler assessment if concern for vascular compromise).
- Skin and Soft Tissue: Evaluate the extent of skin loss, contamination, swelling, and integrity of the eponychial and paronychial folds.
- Nail Unit Assessment: Determine the extent of nail plate avulsion, subungual hematoma size, and any obvious nail bed lacerations or exposed matrix. Note the condition of the avulsed nail plate if present.
- Associated Injuries: Evaluate for associated fractures of the distal phalanx, neighboring phalanges, or soft tissue injuries to the remainder of the digit or hand. Check for ligamentous stability of interphalangeal joints.
- Imaging Studies:
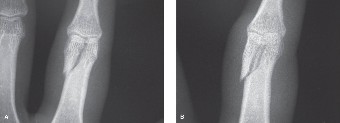
- Radiographs: Standard anteroposterior, lateral, and oblique views of the affected digit are mandatory to identify distal phalangeal fractures, evaluate fracture displacement, assess for intra-articular extension, and detect foreign bodies.
- Advanced Imaging: Rarely indicated, but computed tomography (CT) may be useful for complex comminuted intra-articular fractures or three-dimensional assessment of bone loss, while magnetic resonance imaging (MRI) could be considered for suspected tendon injuries or occult foreign bodies, though often unnecessary for typical nail unit trauma.
Anesthesia
Local or regional anesthesia is typically sufficient.
* Digital Block: A ring block at the base of the digit with plain lidocaine (1% or 2%) is generally safe and effective. While traditionally vasoconstrictors (epinephrine) were avoided in digital blocks due to theoretical ischemia risk, current evidence suggests their safe use in non-compromised digits, particularly in the presence of robust digital artery flow, to prolong anesthesia and reduce bleeding. However, many surgeons still prefer plain lidocaine for nail unit repair.
* Wrist Block or Axillary Block: May be preferred for more complex, prolonged cases, or for uncooperative patients.
* General Anesthesia: Reserved for pediatric patients, highly anxious adults, or complex multi-digit injuries.
Tourniquet Application
A digital tourniquet (e.g., Penrose drain, specialized finger tourniquet) applied at the base of the digit is highly recommended to achieve a bloodless field, which is critical for meticulous nail bed repair. The tourniquet time should be carefully monitored, typically not exceeding 60-90 minutes.
Equipment and Instrumentation
- Magnification: Surgical loupes (2.5x to 4.5x) are essential for precise visualization of the delicate nail matrix. A headlight further enhances illumination.
- Fine Instruments: Adson-Brown tissue forceps, delicate curved iris scissors, tenotomy scissors, mosquito hemostats, fine skin hooks, small needle holders (e.g., Castroviejo), small bone reduction forceps (if fracture present).
- Sutures: Fine absorbable monofilament sutures (e.g., 6-0 or 7-0 Chromic gut, PDS, Monocryl) for nail bed repair. Non-absorbable monofilament sutures (e.g., 5-0 or 6-0 Nylon) for skin closure.
- K-wires: 0.028 or 0.035 inch K-wires for distal phalanx fracture stabilization, if required.
- Nail Plate Management: Small curette or Freer elevator for gentle nail plate removal. Silicone sheeting or a foil packet can be used as a nail bed splint if the original nail plate is unusable.
Patient Positioning
The patient is typically positioned supine. For upper extremity injuries, the affected arm is placed on a dedicated hand table, with the elbow flexed and the shoulder abducted to provide comfortable access. For lower extremity (toe) injuries, appropriate foot draping and positioning are essential. The entire limb should be prepped and draped in a sterile fashion, allowing for potential extension of the incision or procurement of local flaps if necessary.
Detailed Surgical Approach and Technique
The surgical approach to nail unit injuries hinges on meticulous technique, precise anatomical restoration, and appropriate management of any associated bony trauma. A bloodless field and adequate magnification are paramount.
Anesthesia and Tourniquet
Following successful administration of digital block or regional anesthesia, a digital tourniquet is applied at the base of the digit to ensure optimal visualization. The tourniquet time is continuously monitored.
Nail Plate Removal
If a subungual hematoma exceeds 50% of the nail plate, or if there is any suspicion of nail bed laceration or avulsion, the nail plate should be carefully removed.
1. Gently separate the nail plate from the underlying nail bed using a Freer elevator or a small blunt dissector, starting from the lateral sulci.
2. Elevate the eponychium proximally to expose the germinal matrix and the proximal nail plate attachment.
3. Carefully dissect the nail plate from the eponychial fold and matrix, attempting to preserve the integrity of the nail plate for potential use as a physiological stent later.
4. Once the nail plate is removed, thoroughly irrigate the wound with sterile saline.
Wound Exploration and Debridement
- Thorough Inspection: With the nail plate removed, the entire nail bed (germinal and sterile matrices), eponychium, paronychium, and underlying distal phalanx are exposed and meticulously inspected.
- Debridement: Remove any devitalized tissue, foreign bodies, and hematoma. Preserve all viable nail bed tissue, as it is critical for long-term function and cosmesis. Irrigation with saline or an antiseptic solution is performed to minimize contamination.
Nail Bed Repair
Accurate reapproximation of the nail bed is the cornerstone of preventing permanent nail deformities.
- Laceration Identification: Clearly identify the edges of any germinal or sterile matrix lacerations. Stellate or complex lacerations require careful planning for closure.
- Suture Technique: Using fine absorbable monofilament sutures (e.g., 6-0 or 7-0 Chromic gut, PDS, or Monocryl) on a fine ophthalmic needle, meticulously reapproximate the nail bed edges.
- Place sutures precisely to align the matrix layers, ensuring that the epidermal and dermal components are in perfect apposition. Avoid excessive tension.
- Interrupted sutures are typically used. For stellate lacerations, start with the most significant linear component and then address secondary branches.
- The goal is to create a smooth, continuous surface that will allow the new nail plate to grow without obstruction or adherence issues.
- Avulsion Injuries: If a segment of the nail bed is avulsed but still attached, carefully reposition and suture it back into its anatomical location.
- Tissue Loss: For cases with significant nail bed tissue loss that cannot be primarily closed without tension, grafting may be necessary.
- Sterile Matrix Graft: Harvest a small, non-hair-bearing segment of sterile matrix from an adjacent non-critical toe (e.g., second toe) or from a discarded segment of the injured digit if available. Suture it precisely into the defect.
- Full-Thickness Skin Graft: A full-thickness skin graft from the hypothenar eminence or medial arm can be used as a last resort for large defects, although it will not produce nail and may lead to a permanent nail defect. The goal is primarily wound closure and protection of the underlying bone.
Distal Phalanx Fracture Management
Concomitant distal phalanx fractures must be addressed to provide a stable foundation for nail bed healing and prevent bony deformity.
- Reduction:
- Closed Reduction: For stable, non-displaced or minimally displaced fractures, often achieved by simple traction and manual manipulation.
- Open Reduction: For displaced or intra-articular fractures (e.g., Seymour fractures), direct visualization and reduction are necessary.
- Fixation:
- K-wire Fixation: Most common method.
- Trans-osseous: For tuft fractures or unstable comminuted fractures, K-wires (0.028 or 0.035 inch) can be drilled across the fracture fragments from the dorsal nail bed side or from the lateral skin.
- Percutaneous: For distal shaft fractures, K-wires can be inserted from the tip of the finger, through the distal phalanx, and into the middle phalanx to provide longitudinal stability. Care must be taken to avoid violating the DIP joint unless necessary for complex intra-articular fractures.
- Seymour Fractures (Physeal Fractures): These require meticulous reduction and often involve direct repair of the nail bed tear (germinal matrix) and percutaneous K-wire fixation across the physis to stabilize the distal fragment.
- Absorbable Pins: In selected cases, absorbable pins may be considered, though K-wires remain the gold standard for most distal phalanx fractures.
- Bone Grafting: Rarely needed for acute distal phalanx fractures unless there is significant bone loss, which is uncommon in simple crush injuries.
- K-wire Fixation: Most common method.
Nail Plate Replacement or Splinting
After nail bed repair and fracture fixation, maintaining the patency of the eponychial fold and providing a scaffold for new nail growth is critical.
- Original Nail Plate: If the original nail plate is clean and intact, it is the ideal splint. Trim it to fit the nail bed, gently slide it back into the eponychial fold, and secure it with a single non-absorbable suture (e.g., 5-0 Nylon) passed through the distal nail plate and then through the distal aspect of the paronychial skin or hyponychium. This keeps the fold open and prevents synechiae.
- Alternative Splint: If the original nail plate is too damaged or contaminated, a non-adherent material (e.g., silicone sheeting, aluminum foil cut to shape, Xeroform gauze) can be used as a stent. It is similarly tucked into the eponychial fold and secured. This alternative splint should remain in place for 3-4 weeks.
Skin Closure
Close any remaining skin lacerations (paronychial, eponychial) with fine non-absorbable sutures (e.g., 5-0 or 6-0 Nylon) to ensure a smooth transition and protective barrier. Ensure the eponychial fold is not overly constricted.
Tourniquet Release and Dressing
Release the tourniquet and achieve hemostasis. Apply a sterile, non-adherent dressing (e.g., Xeroform, Adaptic) directly over the nail bed, followed by soft bulky gauze and a protective splint if required for fracture management. Avoid tight circumferential dressings that could impede digital circulation.
Complications and Management
Despite meticulous surgical technique, complications can arise following nail unit injuries. Understanding their incidence and appropriate salvage strategies is paramount for long-term patient satisfaction and functional outcomes.
Common Complications and Salvage Strategies
| Complication | Incidence | Salvage Strategy |
|---|---|---|
| Nail Deformity | High (20-50%) | |
| Split Nail (Onychoschisis) | Common (10-30%) | Excision of scar tissue causing the split, meticulous primary repair of the nail bed defect (with local advancement flaps or free matrix grafts if needed), and sometimes permanent nail ablation (matricectomy) if recurrent and symptomatic. |
| Ridging / Dystrophy | Common (15-40%) | May resolve spontaneously. For persistent issues: nail matrix biopsy to rule out tumor, surgical revision of scar tissue, or complete matricectomy with skin graft. |
| Non-Adherence / Onycholysis | Moderate (10-20%) | Surgical exploration to identify and debride underlying scar tissue, revision of the nail bed, possibly sterile matrix grafting. Regular trimming of non-adherent portion. |
| Hook Nail (Pterygium Inversum) | Moderate (5-15%) | Often associated with underlying bone malunion. Surgical correction of bone deformity, wedge ostectomy, or nail bed revision. Excision of the thickened hyponychial tissue. |
| Infection | Moderate (5-10%) | Oral antibiotics for mild cases. Incision and drainage for abscess formation (paronychia, subungual abscess). Debridement and IV antibiotics for osteomyelitis (confirmed by imaging and culture), potentially necessitating removal of hardware or necrotic bone. |
| Pain / Hypersensitivity | Moderate (10-25%) | Conservative management (desensitization therapy, topical agents). Steroid injections for neuromas. Surgical neuroma excision or transposition if refractory. |
| Decreased Sensation | Moderate (5-15%) | Often temporary. Observation. Nerve repair considered for sharp transections in larger digital nerves. |
| Restricted Range of Motion (ROM) | Low (2-5%) | Physiotherapy (active and passive ROM exercises) for adjacent joints. Splinting. Tenolysis if severe adhesion. |
| Chronic Paronychia | Low (2-5%) | Address underlying causes (e.g., retained foreign body, nail spicule). Surgical marsupialization or excision of affected nail fold. |
| Subungual Epidermoid Cyst | Low (1-3%) | Surgical excision of the cyst and careful nail bed repair. |
| Nail Loss | Low (1-5%) | If entire nail unit is non-viable or severely damaged. Complete matricectomy (surgical or chemical) for permanent ablation, followed by skin grafting or allowing secondary intention healing. Prosthetic nail options. |
| Flexor/Extensor Tendon Adhesion | Rare (0.5-2%) | Release of adhesions, tenolysis, and post-operative hand therapy. |
| Growth Arrest / Brachyonychia | Rare (0.5-1%) | Particularly in pediatric physeal injuries. Management is challenging; often requires surgical release of physeal bars or reconstruction in severe cases. |
General Management Principles for Complications
- Early Recognition: Prompt identification of developing complications is crucial for effective intervention. Regular follow-up examinations are essential.
- Imaging: Repeat radiographs are indicated for suspected osteomyelitis or malunion. MRI can be useful for soft tissue assessment.
- Multidisciplinary Approach: Collaboration with hand therapists, pain management specialists, and plastic surgeons can optimize outcomes for complex or refractory complications.
- Patient Education: Manage patient expectations regarding the potential for residual deformity, even with optimal surgical management, particularly in severe crush injuries.
Post Operative Rehabilitation Protocols
Postoperative rehabilitation for nail unit injuries focuses on protecting the repair, promoting healing, preventing infection, and restoring digital function. Protocols vary slightly depending on the extent of injury and associated distal phalanx fractures.
Immediate Postoperative Period (Days 0-7)
- Dressing Management:
- Maintain a sterile, bulky, non-compressive dressing to protect the surgical site and absorb exudate.
- The initial dressing typically includes a non-adherent layer over the nail bed (e.g., Xeroform, Adaptic), followed by soft gauze and an outer protective bandage.
- Change dressings every 2-3 days, or as instructed by the surgeon. Inspect the wound for signs of infection (erythema, swelling, purulent discharge) and skin integrity.
- Elevation: Keep the hand or foot elevated above heart level continuously (especially for the first 48-72 hours) to minimize swelling and throbbing pain.
- Pain Management: Administer oral analgesics as prescribed.
- Immobilization (if fracture present): If a distal phalanx fracture was stabilized, a dorsal or volar splint may be used to protect the repair and provide stability. Maintain the interphalangeal joints in a position of comfort and slight flexion.
- Antibiotics: Oral antibiotics may be prescribed for a short course, particularly for open fractures, contaminated wounds, or patients at high risk of infection.
- Adjunctive Care: Encourage gentle, active range of motion of unaffected joints (e.g., wrist, MCP joints) to prevent stiffness.
Early Healing Phase (Weeks 1-4)
- Suture Removal: Skin sutures are typically removed at 10-14 days post-op. Nail plate sutures (if used to secure the original nail plate or a splint) are typically removed at 3-4 weeks.
- Splint/Nail Plate Removal: If an artificial splint was used, it is typically removed at 3-4 weeks. If the original nail plate was used as a splint, it may be left in place longer (up to 6-8 weeks) as the new nail starts to grow underneath.
- Wound Care: Continue with gentle cleansing and dressing changes as needed. Advise patients to keep the digit dry and clean.
- Early Mobilization:
- If no fracture, or once fracture stability is adequate (typically 3-4 weeks for simple fractures), begin gentle active and passive range of motion exercises for the distal interphalangeal (DIP) joint.
- Focus on gentle flexion and extension to prevent stiffness. Avoid forceful gripping or pinching activities.
- New Nail Growth Monitoring: Educate the patient that the new nail plate will typically appear at the eponychial fold around 2-4 weeks post-injury and will take 4-6 months to completely replace the old nail plate.
- Desensitization: If hypersensitivity or nerve irritation is noted, begin desensitization techniques (e.g., textured rubbing, tapping, vibration).
Intermediate to Late Rehabilitation (Weeks 4-12+)
- Full Range of Motion: Gradually increase the intensity and duration of range of motion exercises for all digital joints.
- Strengthening: Once comfortable, initiate gentle strengthening exercises using soft putty or resistance bands.
- Functional Activities: Progress to activities of daily living (ADLs) and work-related tasks, emphasizing protection of the healing digit.
- Scar Management: For hypertrophic scarring, consider silicone gel sheets or massage therapy.
- Protection: Advise patients to protect the new, growing nail from further trauma. Avoid activities that place direct stress on the nail unit until the new nail is fully mature.
- Monitoring for Complications: Continue to monitor for signs of nail deformity, infection, or chronic pain. Referral to a hand therapist or pain specialist may be indicated for persistent issues.
Return to Activity
- Light Activities/ADLs: Typically 6-8 weeks, once good wound healing, pain control, and basic range of motion are achieved.
- Sport/Heavy Labor: May require 3-6 months, depending on the severity of the initial injury, presence of fracture, and full recovery of strength and function. Protective splinting or taping may be advised for contact sports.
Patient education throughout the rehabilitation process is critical for compliance and managing expectations regarding the often prolonged course of nail regrowth and potential for long-term cosmetic changes.
Summary of Key Literature and Guidelines
The management of nail unit injuries, while often perceived as minor, has evolved significantly with a greater appreciation for meticulous repair and a focus on long-term functional and aesthetic outcomes. A robust body of literature supports the principles outlined, emphasizing the importance of accurate diagnosis and surgical technique.
Foundational Principles and Evidence
- Nail Bed Repair: The cornerstone of modern management, underscored by numerous clinical studies. Reports by Zook et al. (1976) and more recent systematic reviews consistently demonstrate that meticulous repair of nail bed lacerations significantly reduces the incidence of long-term nail deformities such as split nails, ridging, and non-adherence compared to simple drainage or non-repair. The use of fine absorbable sutures and adequate magnification are critical technical points widely supported in the literature.
- Subungual Hematoma: The debate surrounding exploration for hematomas covering less than 50% of the nail plate has largely settled. While some older literature advocated for routine nail plate removal and nail bed repair for all large hematomas, current consensus, supported by studies like those by Zook et al. (1984) and more recent evidence syntheses, suggests that simple trephination is adequate for hematomas under an intact nail plate, provided there is no associated fracture or eponychial fold disruption. However, any suspicion of underlying nail bed laceration, especially with an avulsed or extensively damaged nail plate, warrants exploration.
- Distal Phalanx Fractures: The management of associated distal phalanx fractures is intimately linked to nail bed outcomes. Studies on Seymour fractures (Salter-Harris Type I or II physeal fractures with nail bed laceration) highlight the critical need for prompt reduction, repair of the germinal matrix, and stabilization to prevent growth arrest and chronic nail deformity. Work by Ashbell et al. (1967) and more recent pediatric orthopedic literature emphasizes the specific challenges and management principles for these injuries. Tuft fractures generally heal well with conservative management, but displaced or open fractures, particularly with nail bed involvement, benefit from surgical stabilization to provide a stable platform for nail matrix healing.
- Nail Plate Stenting: The practice of replacing the original nail plate or using an artificial stent (e.g., silicone sheet, aluminum foil) to maintain the eponychial fold's patency is widely accepted. Studies have shown this technique helps prevent synechiae formation between the eponychial fold and the germinal matrix, thereby facilitating unimpeded new nail growth. While evidence comparing different stent materials is limited, the primary goal of maintaining the sulcus patency is consistently emphasized.
Evolving Concepts and Controversies
- Digital Anesthesia with Epinephrine: The long-held dogma of avoiding epinephrine in digital blocks has been challenged by recent evidence. Multiple prospective studies and meta-analyses, particularly in emergency medicine and hand surgery literature, suggest that the judicious use of lidocaine with epinephrine is safe for digital blocks in non-compromised digits, offering prolonged anesthesia and a bloodless field. However, many orthopedic surgeons still prefer plain lidocaine for nail unit repair to mitigate any perceived, albeit low, risk.
- Advanced Imaging: While plain radiographs remain the gold standard, the role of advanced imaging (CT, MRI) is continually being refined. For complex distal phalangeal fractures or when retained foreign bodies are suspected, CT scans can provide superior detail. MRI is generally reserved for rare instances of suspected underlying soft tissue pathology not evident on plain film.
- Biologics and Growth Factors: Research into the use of biologics or growth factors to enhance nail bed healing and regeneration is ongoing, but currently, no definitive clinical recommendations exist for routine use in acute nail unit trauma.
- Permanent Nail Ablation (Matricectomy): For cases of irreparable nail bed damage leading to intractable pain or recurrent severe deformity, permanent nail ablation remains a viable option. Techniques include surgical excision, chemical matricectomy (phenol), or CO2 laser ablation. The choice depends on surgeon preference and the specific clinical scenario.
Guidelines and Consensus
Expert consensus from organizations such as the American Academy of Orthopaedic Surgeons (AAOS) and the American Society for Surgery of the Hand (ASSH) generally supports the principles of careful debridement, meticulous nail bed repair, and appropriate management of associated fractures. These guidelines emphasize individualized treatment based on injury characteristics, patient factors, and the goal of restoring form and function. Ongoing education for residents and fellows in the nuances of nail unit anatomy and repair techniques remains crucial to improving outcomes for this common yet challenging spectrum of injuries.
You Might Also Like