
As an academic orthopedic surgeon and medical educator, the management of intertrochanteric fractures, particularly those with unstable patterns, represents a critical area of contemporary orthopedic practice. These fractures pose significant challenges due to their prevalence, the demographic of affected patients, and the biomechanical complexities inherent in achieving stable fixation and optimal functional outcomes. This discourse will provide a comprehensive, high-yield overview for orthopedic surgeons, residents, and medical students, covering the epidemiology, anatomy, evaluation, surgical strategies, complications, and rehabilitation protocols pertinent to these complex injuries.
Introduction and Epidemiology
Intertrochanteric fractures are a significant public health concern, accounting for nearly 50% of all proximal femoral fractures. In the United States, approximately 150,000 such fractures occur annually, with a pronounced demographic predisposition. The annual incidence is notably higher in elderly females (63 per 100,000 population) compared to elderly males (34 per 100,000 population). This sex disparity, with a women-to-men ratio ranging from 2:1 to 8:1, is largely attributed to postmenopausal metabolic changes in bone density and architecture, rendering women more susceptible to fragility fractures.
Factors independently associated with an increased risk of intertrochanteric fractures, as opposed to femoral neck fractures, include advancing age, a higher burden of medical comorbidities, increased dependency in activities of daily living, and a history of other osteoporosis-related fragility fractures. The rising global geriatric population projects a substantial increase in the incidence of these fractures, underscoring the imperative for effective management strategies to minimize morbidity, mortality, and socioeconomic burden. While high-energy mechanisms such as motor vehicle accidents or falls from height can cause intertrochanteric fractures in younger individuals, over 90% of these injuries in the elderly result from low-energy mechanisms, typically a simple fall directly impacting the greater trochanteric area. This highlights the underlying issue of bone fragility in the elderly population.
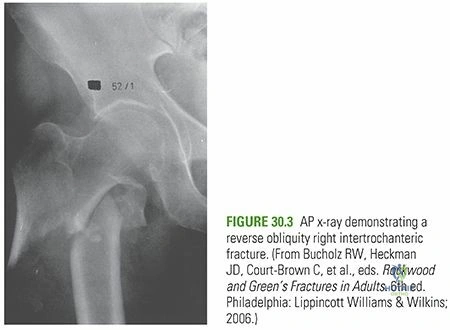
The classification of these fractures is paramount for determining stability and guiding implant selection. The AO/OTA classification divides trochanteric fractures (31A) into simple pertrochanteric (31A1), multifragmentary pertrochanteric (31A2), and intertrochanteric/reverse oblique (31A3). Unstable patterns generally include 31A2.2 and 31A2.3 (loss of posteromedial support and lateral wall comminution) as well as all 31A3 patterns. Recognizing these unstable configurations is the first critical step in preoperative planning.
Surgical Anatomy and Biomechanics
Intertrochanteric Region Morphology
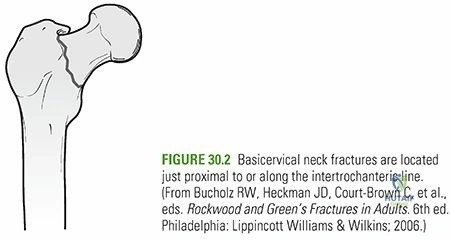
Intertrochanteric fractures occur within the extracapsular region of the proximal femur, specifically between the greater and lesser trochanters. This region encompasses a rich cancellous bone environment, which benefits from an abundant blood supply. Consequently, complications such as nonunion and osteonecrosis, which are more problematic in intracapsular femoral neck fractures, are significantly less common.
The greater trochanter serves as the insertion point for the gluteus medius and minimus, primary abductors of the hip. The lesser trochanter, conversely, is the insertion point for the iliopsoas, a powerful hip flexor and external rotator. The intertrochanteric line anteriorly and the intertrochanteric crest posteriorly connect these two trochanters. The medial femoral neck-shaft junction is reinforced by the calcar femorale, a dense vertical buttress of bone that extends from the posteromedial aspect of the femoral neck toward the lesser trochanter.
Deforming Muscle Forces and Fracture Instability
Upon fracture, predictable deforming muscle forces contribute to displacement. The abductors (gluteus medius and minimus) tend to displace the greater trochanter fragment laterally and proximally. The iliopsoas muscle exerts a strong pull, displacing the lesser trochanter fragment medially and proximally. Additionally, the collective action of hip flexors, extensors, and adductors pulls the entire distal femoral fragment proximally, resulting in shortening, external rotation, and varus positioning at the fracture site.
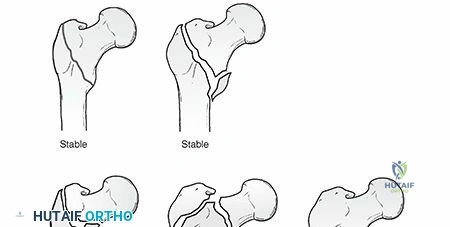
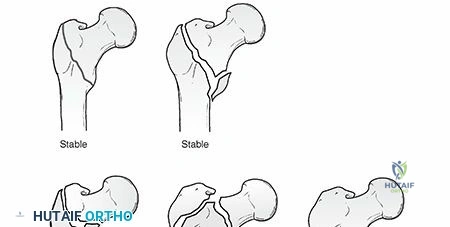
Fracture stability is critically determined by the integrity of the posteromedial cortex, which functions as a primary buttress against varus collapse and retroversion under physiological loading. Unstable intertrochanteric fracture patterns are characterized by the loss of this posteromedial support, significant comminution involving the greater trochanter, subtrochanteric extension, or a reverse obliquity fracture line.
The Concept of the Lateral Wall
In contemporary orthopedic biomechanics, the integrity of the lateral femoral wall has emerged as a paramount determinant of stability. The lateral wall is defined as the intact cortical bone extending from the vastus ridge to the tip of the greater trochanter. In the presence of a lateral wall fracture or insufficient lateral wall thickness (typically less than 20.5 mm), the fracture is inherently unstable. When a sliding hip screw (SHS) is utilized in such scenarios, the proximal fragment can slide laterally unchecked, leading to excessive collapse, medialization of the femoral shaft, and ultimate construct failure. Consequently, unstable patterns with lateral wall compromise necessitate intramedullary fixation to bypass the deficient lateral cortex and provide a stable medial buttress.
Indications and Contraindications
The overarching goal of managing intertrochanteric fractures is the rapid restoration of mobility to mitigate the cascade of systemic complications associated with prolonged recumbency in the geriatric population. These complications include deep vein thrombosis, pulmonary embolism, decubitus ulcers, pneumonia, and rapid deconditioning. Therefore, operative intervention is considered the gold standard for the vast majority of intertrochanteric fractures.

Non-operative management is exceptionally rare and is strictly reserved for a highly specific subset of patients. The decision to pursue non-operative treatment must be made collaboratively with the patient, their family, and the geriatric or internal medicine co-management team.
| Management Strategy | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Operative Fixation | Displaced or non-displaced intertrochanteric fractures in ambulatory patients; Reverse obliquity patterns; Subtrochanteric extension. | Active systemic infection; Moribund patient with unacceptable anesthetic risk (ASA V); Uncorrectable severe coagulopathy. | Active local soft tissue infection over the planned surgical site; Severe dementia where pain is minimal and surgery offers no quality-of-life improvement. |
| Non-Operative Management | Non-ambulatory, bedbound patients with minimal pain; End-of-life/hospice care patients; Patients with absolute medical contraindications to anesthesia. | Ambulatory patients with displaceable or unstable fracture patterns; Patients with severe pain exacerbated by conservative care. | Polytrauma patients requiring rapid mobilization; Younger patients with high functional demands. |
Pre Operative Planning and Patient Positioning
Radiographic Evaluation and Templating
Comprehensive preoperative planning begins with meticulous radiographic evaluation. Standard imaging includes an anteroposterior (AP) view of the pelvis and a cross-table lateral view of the affected hip. An AP view of the entire femur is also mandatory to assess for excessive anterior bowing, prior hardware, or distal pathological lesions that might dictate the length and radius of curvature of an intramedullary nail. In cases of severe comminution or when subtrochanteric extension is suspected but poorly visualized, a computed tomography (CT) scan with 3D reconstructions can be invaluable for defining fracture morphology and planning reduction trajectories.
Digital templating is a critical step. The surgeon must determine the native neck-shaft angle from the contralateral uninjured hip to guide the selection of the cephalomedullary implant angle (typically 125, 130, or 135 degrees). Templating also dictates the anticipated lag screw length, nail diameter (assessing the narrowest portion of the isthmus), and nail length. For unstable patterns, particularly those with subtrochanteric extension or reverse obliquity, long cephalomedullary nails spanning the entire femur are often preferred to protect the entire bone from stress risers and subsequent peri-implant fractures.
Patient Positioning and Operating Room Setup
Proper patient positioning is arguably as critical as the surgical technique itself. The procedure is typically performed on a specialized fracture table, allowing for controlled traction and multi-planar fluoroscopic imaging. The patient is placed supine with the operative leg secured in a traction boot. The contralateral leg is placed in a hemilithotomy position or scissored posteriorly to allow unobstructed access for the C-arm to obtain true lateral views of the proximal femur.
Alternatively, some surgeons prefer a flat radiolucent table, utilizing manual traction or a femoral distractor. This technique is particularly advantageous in polytrauma patients or those with severe soft tissue contractures where fracture table positioning is contraindicated. Regardless of the table utilized, the C-arm must be positioned to easily toggle between AP and lateral views without compromising the sterile field. The surgeon must confirm adequate visualization of the femoral head, neck, trochanteric region, and the entire femoral shaft down to the knee before prepping and draping.
Detailed Surgical Approach and Technique
For unstable intertrochanteric fractures, the cephalomedullary nail (CMN) is the implant of choice. The technique requires meticulous attention to reduction, entry point, and implant positioning.
Fracture Reduction Strategies
Anatomic or near-anatomic reduction must be achieved prior to initiating the surgical approach. Fixation of an unreduced fracture guarantees a high rate of mechanical failure.
Closed reduction is attempted first via longitudinal traction, slight adduction (to clear the greater trochanter for the entry point), and internal rotation (to correct the external rotation deformity and profile the femoral neck). The reduction is evaluated fluoroscopically. In the AP plane, the medial cortex should be aligned or slightly valgus; varus alignment is unacceptable. In the lateral plane, the anterior cortex should be collinear without sag.
If closed reduction is inadequate, percutaneous or limited open reduction techniques must be employed. Sagittal plane sag can be corrected by placing a crutch or a specialized bump under the posterior thigh, or by using a percutaneous ball-spike pusher applied to the anterior cortex of the proximal fragment. Coronal plane malalignment can be addressed with a bone hook placed around the lesser trochanter or by inserting a Steinmann pin into the proximal fragment to serve as a joystick.
Surgical Approach and Entry Point
A longitudinal incision is made proximal to the greater trochanter, in line with the femoral shaft. The fascia lata is incised, and the gluteus maximus fibers are split bluntly to access the tip of the greater trochanter.
The entry point is the most critical step in intramedullary nailing. For a standard trochanteric entry nail, the ideal starting point on the AP view is exactly at the tip of the greater trochanter or slightly medial to it. A lateral starting point will result in varus malalignment upon nail insertion, a catastrophic error in unstable fractures. On the lateral view, the entry point should be centered in the anterior-posterior dimension of the greater trochanter, in line with the medullary canal.
Canal Preparation and Nail Insertion
A guide wire is advanced down the femoral shaft under fluoroscopic guidance. The proximal femur is opened with a rigid reamer. For long nails, the diaphyseal canal is sequentially reamed over a ball-tipped guide wire to a diameter 1.0 to 1.5 mm larger than the selected nail diameter to prevent incarceration and accommodate the anterior bow of the femur.
The selected cephalomedullary nail is inserted over the guide wire. The nail should be advanced manually; forceful impaction with a mallet can cause iatrogenic comminution or extension of the fracture into the subtrochanteric region. The depth of insertion is dictated by the planned trajectory of the proximal lag screw or helical blade, which should ideally sit in the center-center position of the femoral head.
Proximal and Distal Fixation
Once the nail is appropriately seated, the guide pin for the proximal fixation element is inserted. The trajectory must be evaluated in both AP and lateral planes. The goal is to place the lag screw or blade centrally in the femoral head on the AP view and centrally on the lateral view.
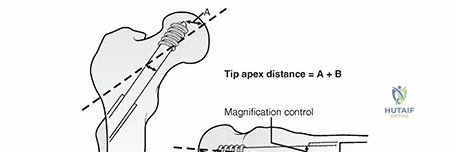
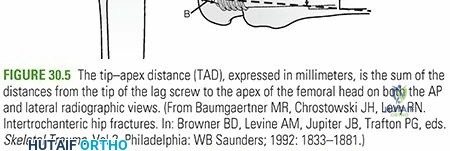
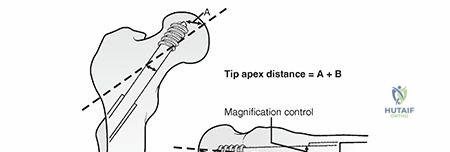
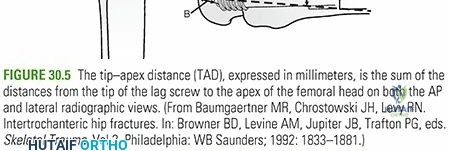
The concept of Tip-Apex Distance (TAD), described by Baumgaertner, is critical here. The TAD is the sum of the distance from the tip of the lag screw to the apex of the femoral head on the AP view and the lateral view. A TAD of less than 25 mm is strongly correlated with successful fixation and a minimized risk of lag screw cut-out. For helical blades, a slightly modified measurement may be used, but the principle of deep, central placement remains the same. Once the proximal element is deployed, compression can be applied across the fracture site if the pattern allows, though excessive compression in highly comminuted or reverse obliquity patterns should be avoided to prevent shortening.
Distal interlocking is performed to control rotation and maintain length. For short nails, dynamic or static locking can be utilized depending on fracture stability. For long nails, at least two distal locking screws are recommended, utilizing a freehand perfect-circle technique or an electromagnetic targeting system.
Complications and Management
Despite advances in implant design and surgical technique, the management of unstable intertrochanteric fractures carries a significant complication profile. Complications can be broadly categorized into mechanical failures and systemic medical issues.
Mechanical failure most commonly manifests as lag screw cut-out, varus collapse, or implant breakage. Cut-out occurs when the proximal fixation element migrates superiorly and anteriorly through the osteoporotic bone of the femoral head, eventually penetrating the articular cartilage. This is primarily driven by an uncorrected varus reduction, an eccentric lag screw position (high TAD), or severe intrinsic bone quality deficits.
When mechanical failure occurs, salvage strategies depend on patient physiology, remaining bone stock, and articular integrity. If the articular surface is destroyed by a cut-out screw, conversion to a total hip arthroplasty (THA) is required. This is a complex procedure often necessitating a calcar-replacing prosthesis or a long fully porous-coated diaphyseal engaging stem to bypass the compromised proximal bone.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Strategy |
|---|---|---|---|
| Lag Screw Cut-Out | 2% - 8% | TAD > 25mm; Varus malreduction; Superior/anterior screw placement; Severe osteoporosis. | Conversion to Total Hip Arthroplasty (THA) using a modular or calcar-replacing stem. |
| Varus Collapse / Malunion | 5% - 10% | Failure to restore medial buttress; Lateral entry point during nailing; Early weight-bearing in highly unstable patterns. | Corrective proximal femoral osteotomy (rare in elderly); Conversion to THA if symptomatic. |
| Peri-implant Fracture | 1% - 3% | Stress riser at the tip of a short nail; Excessive anterior bowing mismatch; Iatrogenic cortical breach during reaming. | Revision to a longer intramedullary nail; Open reduction and internal fixation with a locking plate spanning the defect. |
| Nonunion | < 2% | Infection; Inadequate stability; Distraction at the fracture site; Poor local biology. | Rule out infection; Exchange nailing with larger diameter; Bone grafting; Dynamic locking. |
| Deep Surgical Site Infection | 1% - 2% | Medical comorbidities (Diabetes, malnutrition); Prolonged operative time; Open fracture (rare). | Aggressive irrigation and debridement; Suppressive antibiotics; Implant removal once fracture heals; Resection arthroplasty if intractable. |
Systemic complications are closely tied to the patient's preoperative medical optimization. Deep vein thrombosis (DVT) and pulmonary embolism (PE) remain significant risks, necessitating aggressive chemical and mechanical prophylaxis. Delirium, pneumonia, and urinary tract infections are also highly prevalent, requiring a multidisciplinary approach to perioperative care.
Post Operative Rehabilitation Protocols
The immediate postoperative goal is the mobilization of the patient. The modern standard of care dictates that patients with cephalomedullary fixation for intertrochanteric fractures should be allowed weight-bearing as tolerated (WBAT) immediately following surgery. Restricting weight-bearing in the geriatric population is generally ineffective, as these patients often lack the upper body strength and cognitive reserve to comply with partial or non-weight-bearing instructions. Furthermore, the biomechanical strength of a well-placed intramedullary device is sufficient to withstand physiological loads, and early weight-bearing promotes secondary bone healing through micromotion.
Physical therapy should commence on postoperative day one, focusing on bed-to-chair transfers, ambulation with an assistive device (walker or cane), and progressive resistance exercises for the hip abductors and quadriceps. Occupational therapy is equally important for assessing the patient's ability to perform activities of daily living and determining the appropriate discharge disposition, whether that be home with assistance or a subacute rehabilitation facility.
Medical co-management is a cornerstone of the postoperative protocol. Ortho-geriatric care models have been definitively shown to reduce mortality, decrease length of hospital stay, and improve functional outcomes. This includes meticulous management of polypharmacy, optimization of glycemic control, aggressive pain management utilizing multimodal opioid-sparing pathways, and early intervention for postoperative delirium.
Crucially, the occurrence of an intertrochanteric fracture is a sentinel event indicating severe underlying osteoporosis. Initiation of secondary fracture prevention protocols is mandatory. This involves a comprehensive metabolic bone health evaluation, optimization of Vitamin D and calcium levels, and the initiation of appropriate antiresorptive (e.g., bisphosphonates, denosumab) or anabolic (e.g., teriparatide, romosozumab) pharmacological therapy prior to or shortly after hospital discharge.
Summary of Key Literature and Guidelines
The management of unstable intertrochanteric fractures is heavily guided by established orthopedic literature and clinical practice guidelines. The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines strongly recommend regional analgesia to reduce the risk of delirium and strongly advocate for surgery within 48 hours of admission to reduce mortality.

Key biomechanical and clinical studies have shaped our current understanding of fixation failure. Baumgaertner's seminal work established the Tip-Apex Distance (TAD) as the most powerful predictor of lag screw cut-out, setting the standard threshold at less than 25 mm. Subsequent literature by Cleveland et al. refined this by mapping the femoral head into zones, confirming that center-center placement (Zone 5) provides the most robust fixation.
The superiority of intramedullary nailing over sliding hip screws for unstable patterns has been validated extensively. Haidukewych et al. demonstrated unacceptably high failure rates when utilizing sliding hip screws for reverse obliquity fractures, cementing the cephalomedullary nail as the standard of care for 31A3 patterns. Furthermore, Palm et al. highlighted the critical role of the lateral wall, showing that preoperative lateral wall thickness is a primary determinant of postoperative stability, and that iatrogenic fracture of the lateral wall during SHS insertion converts a stable fracture into an unstable one, necessitating intramedullary fixation.
In conclusion, the successful management of unstable intertrochanteric fractures requires a profound understanding of proximal femoral anatomy, rigorous preoperative planning, and meticulous surgical execution. By respecting the biomechanical principles of the lateral wall, achieving anatomic reduction, and adhering to strict parameters for implant placement, orthopedic surgeons can reliably restore function and minimize the substantial morbidity associated with these complex fragility fractures. Continuous integration of ortho-geriatric co-management and secondary osteoporosis prevention remains essential for optimizing long-term patient survival and quality of life.
Clinical & Radiographic Imaging

Detailed Chapters & Topics
Dive deeper into specialized chapters regarding intertrochanteric-fractures