Intertrochanteric Femoral Fractures: Comprehensive Surgical Management

Key Takeaway
Intertrochanteric femoral fractures represent a significant portion of proximal femur trauma, demanding precise biomechanical understanding and surgical execution. This comprehensive guide details the AO/OTA classification, indications for dynamic hip screws versus intramedullary nailing, and step-by-step operative techniques. By mastering these evidence-based protocols, orthopedic surgeons can optimize implant stability, minimize complications such as osteonecrosis, and ensure early mobilization in both stable and highly comminuted fracture patterns.
Comprehensive Introduction and Patho-Epidemiology
Intertrochanteric femoral fractures represent a profound and escalating challenge within the realm of orthopedic traumatology, constituting approximately half of all proximal femur fractures. These injuries predominantly afflict the geriatric population, functioning as a sentinel event of underlying osteoporosis and frailty. In this demographic, the mechanism of injury is almost universally a low-energy event, typically a fall from a standing height directly onto the lateral aspect of the greater trochanter. Conversely, in younger, physiologically robust cohorts, intertrochanteric fractures are the sequelae of high-energy trauma, such as motor vehicle collisions or falls from significant heights, often presenting with concomitant polytrauma and severe soft tissue compromise. Because the intertrochanteric region is entirely extracapsular and composed of highly vascularized cancellous bone, these fractures boast a robust biological healing potential; however, the complex biomechanical forces acting across the proximal femur make achieving and maintaining stable surgical fixation a profound clinical challenge.
The epidemiological landscape of intertrochanteric fractures is shifting dramatically due to the global "silver tsunami." As the population ages, the incidence of these fragility fractures is projected to skyrocket, placing an unprecedented economic and logistical burden on healthcare systems worldwide. The one-year mortality rate following an intertrochanteric fracture in the elderly remains staggeringly high, ranging from 20% to 30%, largely driven by the exacerbation of pre-existing medical comorbidities and the physiological stress of the injury itself. This mortality risk is heavily front-loaded in the initial months following the fracture, underscoring the critical nature of the perioperative period. Furthermore, a significant percentage of patients who survive the injury fail to return to their pre-injury level of independence, often requiring transition to assisted living or skilled nursing facilities.
The primary, overriding goal of operative intervention is to achieve a biomechanically stable fixation construct that permits immediate, unrestricted postoperative mobilization. The historical approach of prolonged skeletal traction and recumbency has been entirely abandoned due to its unacceptably high rates of devastating systemic complications, including deep vein thrombosis (DVT), massive pulmonary embolism, hypostatic pneumonia, profound muscular deconditioning, and intractable decubitus ulcers. Modern orthopedic surgery dictates that the fracture must be stabilized expeditiously—ideally within 24 to 48 hours of presentation—to facilitate early weight-bearing, thereby mitigating these life-threatening complications and optimizing the patient's functional trajectory.
The evolution of surgical management for intertrochanteric fractures reflects a continuous refinement of biomechanical principles. From the early use of fixed-angle nail plates, which frequently failed due to an inability to accommodate fracture impaction, to the revolutionary introduction of the sliding hip screw (Dynamic Hip Screw), and finally to the widespread adoption of cephalomedullary nails, the armamentarium available to the orthopedic surgeon has vastly improved. However, this technological advancement demands a rigorous understanding of fracture morphology, implant biomechanics, and precise surgical execution. The surgeon must meticulously match the appropriate implant to the specific fracture pattern, recognizing that a failure to respect the inherent stability—or instability—of the fracture will inevitably lead to catastrophic hardware failure and profound patient morbidity.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy and biomechanics of the proximal femur is the absolute prerequisite for the successful management of intertrochanteric fractures. Osteologically, the intertrochanteric region is defined as the area extending from the extracapsular basilar neck to the distal extent of the lesser trochanter. This region represents the critical transition zone between the femoral neck and the diaphyseal shaft. It is characterized by a dense network of cancellous bone trabeculae that align precisely along the lines of principal mechanical stress. The primary compressive trabeculae extend from the medial calcar femorale into the superior aspect of the femoral head, while the primary tensile trabeculae arch from the lateral cortex into the inferior femoral head. The intersection of these trabecular patterns forms Ward's triangle, an area of relative radiolucency and structural weakness that becomes increasingly pronounced with advancing osteoporosis, predisposing the bone to failure under minimal load.
The vascular anatomy of the proximal femur is robust, which accounts for the excellent union rates observed in extracapsular fractures. The primary blood supply to the femoral head and neck is derived from the medial and lateral circumflex femoral arteries, which form an extracapsular arterial ring at the base of the femoral neck. Ascending cervical branches (retinacular vessels) pierce the capsule to supply the head. Because intertrochanteric fractures occur distal to this capsular attachment, the retinacular vessels are typically spared, rendering the risk of post-traumatic osteonecrosis (avascular necrosis) exceedingly low compared to intracapsular femoral neck fractures. However, the highly vascularized nature of the cancellous bone in this region means that intertrochanteric fractures are associated with significant, often concealed, hemorrhage. Patients frequently lose between one and two units of blood into the thigh compartments, necessitating rigorous perioperative hemodynamic monitoring and judicious blood product transfusion.
The muscular attachments surrounding the proximal femur dictate the characteristic displacement patterns observed in these fractures. The iliopsoas tendon inserts onto the lesser trochanter; when this fragment is avulsed or comminuted, the proximal fragment is pulled into flexion and external rotation. The powerful abductor musculature (gluteus medius and minimus) attaches to the greater trochanter, exerting a strong superior and lateral force. The short external rotators further contribute to the external rotation deformity. Meanwhile, the longitudinal pull of the massive thigh musculature (quadriceps and hamstrings) drives the distal diaphyseal fragment proximally, resulting in profound limb shortening and varus collapse. Overcoming these deforming muscular forces during closed reduction on the fracture table is a critical and often challenging step in the surgical procedure.
Biomechanically, the proximal femur is subjected to immense joint reaction forces, often exceeding three to four times body weight during normal ambulation. These forces create a massive bending moment across the intertrochanteric region. The medial cortex, specifically the calcar femorale, acts as the primary buttress against compressive forces, while the lateral wall functions as a critical tension band. The integrity of the lateral wall is the single most important determinant of fracture stability. If the lateral wall is incompetent or iatrogenically fractured during surgery, the proximal fragment will invariably collapse into varus, leading to medialization of the femoral shaft and catastrophic implant cut-out. Understanding the concept of the "lever arm" is also vital: sliding hip screws possess a longer lever arm, placing significant stress on the lateral cortex, whereas intramedullary devices offer a shorter lever arm, transferring weight-bearing loads more directly to the femoral diaphysis, thereby providing superior biomechanical stability in highly comminuted or reverse obliquity fracture patterns.
Exhaustive Indications and Contraindications
The decision-making process regarding the operative management of intertrochanteric fractures is heavily weighted toward surgical intervention, with non-operative management relegated to exceptionally rare, specific clinical scenarios. Operative fixation is the definitive standard of care, aimed at restoring the anatomical alignment of the proximal femur and establishing a construct stable enough to withstand the physiological loads of immediate weight-bearing. The selection of the specific surgical implant—primarily between a sliding screw-plate device (Dynamic Hip Screw) and a cephalomedullary nail—is strictly dictated by the morphological classification of the fracture, the integrity of the lateral femoral wall, and the presence of subtrochanteric extension.
Non-operative management is strictly reserved for patients who are entirely non-ambulatory, bedbound, and possess severe, uncorrectable medical comorbidities where the perioperative mortality risk unacceptably outweighs any potential benefit of surgery. In these rare instances, treatment focuses entirely on palliative measures, including aggressive pain management, meticulous nursing care to prevent decubitus ulcers, and pulmonary toilet. It must be explicitly understood that non-operative management in a previously ambulatory patient is a life-limiting decision, as the ensuing cascade of recumbency-related complications will almost certainly lead to rapid physiological decline and death.
The indications for a Dynamic Hip Screw (DHS) are narrow but well-defined within modern orthopedic practice. The DHS is indicated exclusively for stable intertrochanteric fracture patterns, specifically AO/OTA 31A1 (simple pertrochanteric) and select 31A2 (multifragmentary) fractures where the lateral femoral wall is definitively intact and robust. A lateral wall thickness of greater than 20.5 mm on the preoperative AP radiograph is generally considered the threshold for safe DHS utilization. The DHS relies on the biomechanical principle of controlled collapse, allowing the proximal fragment to impact along the axis of the lag screw until the fracture surfaces compress, thereby promoting primary bone healing.
Conversely, cephalomedullary nailing is the absolute implant of choice for all unstable intertrochanteric fracture patterns. This includes AO/OTA 31A2 fractures with lateral wall comminution or a thickness of less than 20.5 mm, and all AO/OTA 31A3 (reverse obliquity and transverse) fractures. In these unstable patterns, the lateral wall is incompetent and cannot act as a lateral buttress. The use of a DHS in such scenarios is strictly contraindicated, as it will inevitably result in uncontrolled medialization of the femoral shaft, excessive sliding of the lag screw, and rapid construct failure. Cephalomedullary nails bypass the compromised lateral wall, functioning as load-sharing devices with a shorter lever arm, thereby providing the necessary stability for early mobilization in complex fracture morphologies.
Table: Indications and Contraindications for Intertrochanteric Fracture Management
| Modality / Implant | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Non-Operative Management | Moribund patients; non-ambulatory, bedbound patients with terminal illness; unacceptable anesthetic risk. | Ambulatory patients; medically optimized patients; presence of severe pain not controlled by conservative means. | Severe cognitive impairment (dementia) where compliance is poor (though surgery is still preferred for pain control). |
| Dynamic Hip Screw (DHS) | Stable patterns (AO/OTA 31A1); select 31A2 with intact lateral wall (>20.5mm thickness). | Reverse obliquity patterns (31A3); subtrochanteric extension; incompetent/comminuted lateral wall. | Severe osteoporosis where screw purchase is questionable; pathological fractures. |
| Cephalomedullary Nail (Short) | Unstable patterns (AO/OTA 31A2 with lateral wall comminution); reverse obliquity (31A3) without significant subtrochanteric extension. | Active femoral medullary canal infection; narrow intramedullary canal preventing nail insertion. | Excessive anterior bowing of the femur (risk of anterior cortical perforation). |
| Cephalomedullary Nail (Long) | Fractures with subtrochanteric extension; pathological fractures; highly comminuted reverse obliquity patterns. | Same as short cephalomedullary nail. | Severe diaphyseal deformity preventing passage of a long straight/bowed nail. |
Pre-Operative Planning, Templating, and Patient Positioning
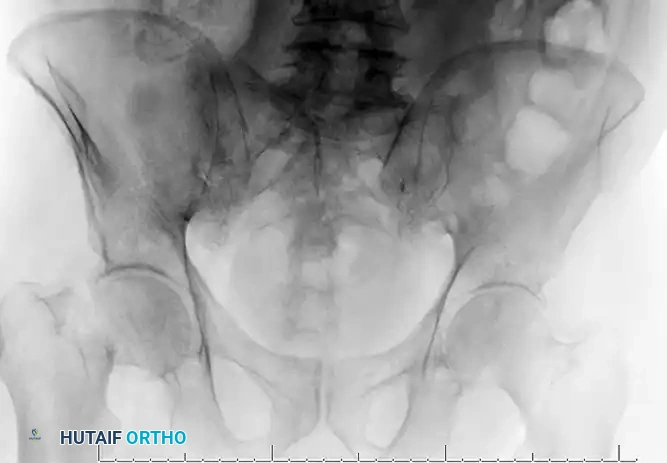
Meticulous preoperative planning is the foundation upon which successful surgical execution is built. The standard radiographic series must include an anteroposterior (AP) view of the pelvis, an AP view of the affected hip with the leg internally rotated 10 to 15 degrees (if tolerated) to profile the femoral neck, and a cross-table lateral view. In the contemporary management of complex proximal femur fractures, the threshold for obtaining a computed tomography (CT) scan with 3D reconstruction should be extremely low. A CT scan is invaluable for assessing the precise degree of posteromedial comminution, the exact thickness and integrity of the lateral wall, and the presence of occult subtrochanteric extension—factors that definitively dictate the choice between a side-plate device and an intramedullary nail.
Digital templating is a mandatory step that must not be bypassed, regardless of the surgeon's experience level. Utilizing calibrated digital radiographs, the surgeon must determine the patient's native neck-shaft angle, which typically ranges from 125 to 135 degrees. For a DHS, templating determines the appropriate angle of the side plate and estimates the required length of the lag screw. For a cephalomedullary nail, templating is critical for selecting the correct nail diameter (ensuring adequate fill without excessive cortical chatter), the nail length (short vs. long), and the appropriate distal locking configuration. The goal of templating is to mentally rehearse the operation, anticipating potential pitfalls, such as a narrow medullary canal that may require sequential reaming, or excessive anterior bowing of the femur that might necessitate a specific nail design to avoid anterior cortical perforation.
Patient optimization requires a rapid, multidisciplinary approach, often involving an ortho-geriatric co-management model. The goal is to optimize the patient for surgery within the critical 48-hour window. This involves rapid correction of electrolyte imbalances, assessment of cardiac and pulmonary status, and the management of anticoagulation. For patients on direct oral anticoagulants (DOACs) or warfarin, specific reversal protocols must be initiated immediately upon admission to prevent unnecessary surgical delays. The choice of anesthesia—typically a regional spinal block versus general anesthesia—is made in conjunction with the anesthesia team, though regional anesthesia is often preferred to minimize postoperative delirium and pulmonary complications in the geriatric population.
Patient positioning on the radiolucent fracture table is arguably the most critical step of the entire procedure; a poor reduction cannot be salvaged by excellent hardware placement. The patient is placed supine, and the perineal post is carefully positioned and heavily padded to prevent devastating pudendal nerve palsies or soft tissue necrosis. The operative leg is secured in a traction boot. Reduction is achieved through a precise sequence: first, gross longitudinal traction is applied to restore limb length and overcome the pull of the massive thigh musculature. Next, the limb is internally rotated 10 to 15 degrees to correct the natural anteversion of the femoral neck, bringing it parallel to the floor. The unaffected leg is typically placed in a hemilithotomy position or extended and abducted in a "scissor" configuration to allow unimpeded access for the C-arm fluoroscope. Perfect AP and lateral fluoroscopic views of the femoral head and neck must be confirmed before the patient is prepped and draped; accepting suboptimal imaging at this stage will guarantee a suboptimal surgical outcome.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of intertrochanteric fracture fixation demands extreme precision, strict adherence to biomechanical principles, and a deep respect for the compromised soft tissues of the geriatric patient. While the cephalomedullary nail has become the dominant implant for most patterns, the insertion of a Dynamic Hip Screw (DHS) remains a highly tested and clinically vital technique for stable fractures. The procedure begins with a standard lateral approach to the proximal femur. A straight lateral incision is made, originating at the palpable tip of the greater trochanter and extending distally along the femoral shaft for approximately 8 to 10 centimeters. The fascia lata is sharply incised in line with the skin incision, exposing the vastus lateralis muscle belly.
The handling of the vastus lateralis is a point of technical nuance. The muscle can either be split longitudinally in the direction of its fibers or elevated posteriorly off the lateral intermuscular septum. Elevating the muscle generally provides a more robust soft tissue envelope for subsequent closure and minimizes bleeding from the perforating branches of the profunda femoris artery. Once the lateral femoral cortex is exposed, a retractor is placed anteriorly over the femoral shaft to maintain exposure. Routine capsulotomy is generally unnecessary for standard extracapsular fractures; however, if an intracapsular extension is suspected or if a massive hematoma is causing severe capsular distension, a capsulotomy may be performed.
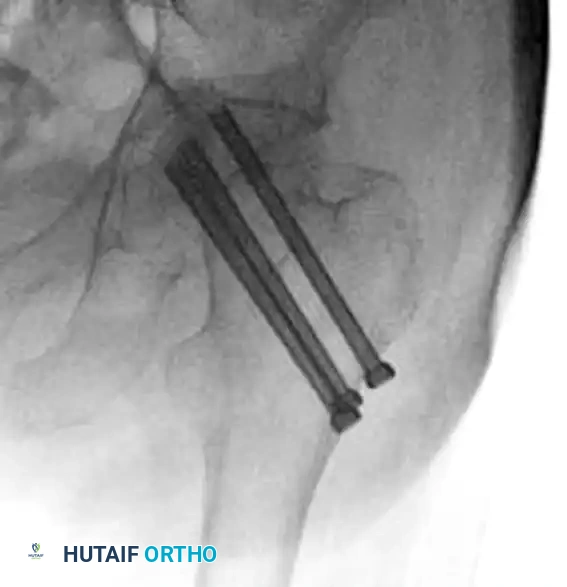
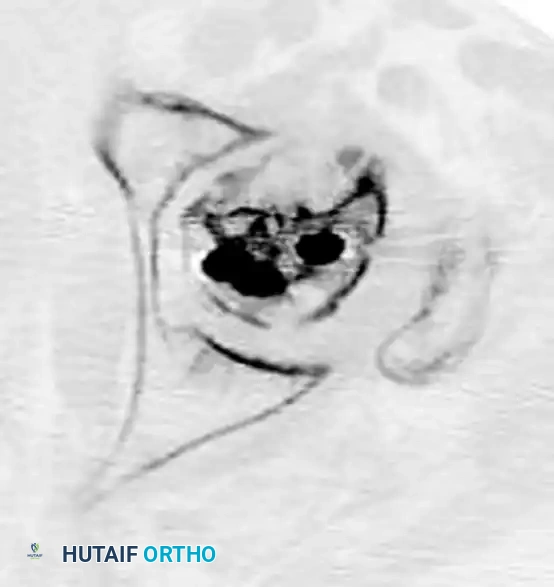
The most critical phase of the DHS procedure is the placement of the guide wire. An angle guide, matching the templated neck-shaft angle (typically 135 degrees), is positioned against the lateral cortex. A 2.8 mm threaded guide wire is then advanced through the lateral cortex, traversing the femoral neck, and into the subchondral bone of the femoral head. The trajectory of this wire must be absolutely flawless: it must be perfectly centered within the femoral head on both the AP and lateral fluoroscopic views. The surgeon must rigorously calculate the Tip-Apex Distance (TAD), as described by Baumgaertner. The TAD is the sum of the distance from the tip of the lag screw to the apex of the femoral head on both the AP and lateral views. A combined TAD of less than 25 mm is the gold standard; exceeding this threshold exponentially increases the risk of mechanical failure and lag screw cut-out.
Once the guide wire is perfectly positioned, a measuring device determines the appropriate length of the lag screw. A specialized triple reamer is then assembled, set to the measured length, and passed over the guide wire. This reamer simultaneously prepares the lateral cortex for the plate barrel, reams the channel for the lag screw, and countersinks the cortex. In young patients with dense cancellous bone, tapping the femoral head is required to prevent the lag screw from acting as a wedge and distracting the fracture during insertion. However, in the severely osteoporotic bone typical of the geriatric population, tapping is strictly avoided to preserve bone stock and maximize the purchase of the lag screw threads.

The selected lag screw is inserted over the guide wire until the threads are fully engaged in the subchondral bone of the femoral head, ensuring the T-handle is parallel to the femoral shaft to allow the plate barrel to slide over the screw flats. The side plate is then guided over the back of the lag screw and impacted firmly against the lateral femoral cortex. The plate is secured to the diaphyseal shaft using 4.5 mm cortical screws. Finally, traction on the fracture table is released, and the fracture is allowed to dynamically compress. A compression screw may be inserted into the back of the lag screw to apply immediate interfragmentary compression, though the primary compression will occur dynamically as the patient bears weight postoperatively.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and the advent of advanced implant designs, the management of intertrochanteric femoral fractures remains fraught with potential complications. These failures are primarily driven by the severe osteoporosis inherent to the patient population, highly unstable fracture morphologies, and technical errors during surgical execution. The most devastating and frequently encountered mechanical complication is the cut-out of the lag screw or helical blade through the superior aspect of the femoral head. This phenomenon occurs when the implant migrates superiorly and anteriorly, eventually breaching the articular cartilage and destroying the acetabulum.
Cut-out is almost exclusively the result of a biomechanical failure, specifically a failure to achieve a Tip-Apex Distance (TAD) of less than 25 mm, or a failure to recognize and respect an incompetent lateral wall. When a DHS is inappropriately utilized in a reverse obliquity pattern or a fracture with a deficient lateral wall, the proximal fragment collapses into varus. This varus collapse shifts the vector of the joint reaction force, driving the implant superiorly. The incidence of cut-out has decreased significantly with the widespread adoption of the TAD concept and the increased use of cephalomedullary nails for unstable patterns, but it still occurs in approximately 1% to 3% of cases.
Nonunion and malunion are less common but equally debilitating complications. Intertrochanteric fractures occur in highly vascularized cancellous bone, making true nonunion relatively rare (less than 1-2%). When nonunion does occur, it is typically associated with catastrophic hardware failure, deep infection, or severe biological compromise. Malunion, conversely, is much more frequent. The classic malunion pattern is varus angulation, shortening of the limb, and excessive external rotation. This deformity severely alters the biomechanics of the hip joint, shortening the abductor lever arm, resulting in a profound Trendelenburg gait, chronic pain, and an accelerated progression of post-traumatic osteoarthritis.
Iatrogenic fractures during the index procedure represent a significant technical hazard. During the insertion of a DHS, aggressive reaming or impaction of the side plate can cause a "blowout" of the lateral wall, instantly converting a stable fracture into a highly unstable one, necessitating an immediate intraoperative switch to a cephalomedullary nail. During intramedullary nailing, a mismatch between the radius of curvature of the implant and the patient's native femoral bow can lead to anterior cortical perforation, particularly when using short, straight nails in patients with excessive anterior bowing.
Table: Complications, Incidence, Prevention, and Salvage Management
| Complication | Estimated Incidence | Primary Prevention Strategy | Salvage Management / Treatment |
|---|---|---|---|
| Implant Cut-Out | 1% - 3% | Strict adherence to TAD < 25mm; appropriate implant selection (avoid DHS in unstable lateral wall patterns). | Conversion to Total Hip Arthroplasty (THA); requires complex reconstruction, often with diaphyseal-fitting stems. |
| Varus Malunion | 5% - 10% | Anatomic reduction on the fracture table prior to fixation; use of IM nail for unstable patterns. | Corrective valgus-producing proximal femoral osteotomy; THA if symptomatic osteoarthritis is present. |
| Nonunion | < 2% | Stable fixation; avoidance of excessive fracture distraction; optimization of biological factors. | Revision internal fixation with bone grafting; conversion to THA in older, lower-demand patients. |
| Iatrogenic Fracture | 1% - 4% | Careful reaming; avoiding excessive force during nail insertion; matching nail curvature to femoral bow. | Intraoperative recognition and fixation with cerclage wires or longer intramedullary nail spanning the defect. |
Salvage of a failed intertrochanteric fracture fixation is one of the most technically demanding procedures in orthopedic surgery. When catastrophic failure occurs—whether through cut-out, nonunion, or severe post-traumatic osteonecrosis—conversion to a Total Hip Arthroplasty (THA) is typically the definitive salvage procedure. This is not a standard primary THA. The anatomy is profoundly distorted, the greater trochanter is often ununited or severely comminuted, and the bone stock of the proximal femur is severely compromised by the retained hardware and osteolysis.
When executing a salvage THA, the surgeon must be prepared for extensive hardware removal, which can result in further bone loss. The femoral stem selection is critical. Standard primary stems will almost certainly fail due to the lack of proximal metaphyseal support and the presence of stress risers created by the previous screw holes. Therefore, the surgeon must utilize diaphyseal-fitting, fully porous-coated, or fluted tapered long stems that bypass the compromised proximal bone and achieve rigid fixation in the femoral diaphysis. If the medial calcar is entirely absent, a calcar replacement stem may be necessary to restore leg length and soft tissue tension.

Phased Post-Operative Rehabilitation Protocols
The surgical fixation of an intertrochanteric fracture is merely the first step in a comprehensive, multidisciplinary continuum of care. The postoperative rehabilitation protocol is as critical to the patient's ultimate survival and functional recovery as the precise execution of the surgery itself. The overarching philosophy of postoperative care is aggressive, immediate mobilization. The historical paradigm of "toe-touch" or "partial" weight-bearing has been entirely discarded for these patients. Regardless of whether a DHS or a cephalomedullary nail was utilized, provided that an acceptable, stable fixation was achieved intraoperatively, the patient must be instructed to bear weight as tolerated (WBAT) immediately on postoperative day zero or one.
The immediate postoperative phase (Days 0 to 3) is focused on medical stabilization and the initiation of physical therapy. Early mobilization is the absolute most effective prophylaxis against the deadly triad of deep vein thrombosis, pulmonary embolism, and hypostatic pneumonia. However, mechanical mobilization alone is insufficient. Rigorous chemical venous thromboembolism (VTE) prophylaxis is mandatory. Current guidelines dictate the use of Low Molecular Weight Heparin (LMWH) or Direct Oral Anticoagulants (DOACs) for a minimum of 28 to 35 days postoperatively, barring absolute contraindications such as active gastrointestinal hemorrhage. This chemical prophylaxis must be combined with mechanical sequential compression devices while the patient is in bed.
The subacute rehabilitation phase (Weeks 1 to 6) transitions the focus toward restoring independent ambulation and muscular strength. Patients will typically require a walker or crutches during this phase. Physical therapy must specifically target the abductor musculature (gluteus medius), which is frequently traumatized by the surgical approach and the initial injury. Weakness in the abductors leads to a persistent Trendelenburg gait and increased stress on the fixation construct. Additionally, aggressive stretching protocols must be implemented to prevent hip flexion contractures, a common sequela of
