Femoral Neck Fractures: Comprehensive Diagnosis, Classification, and Surgical Management
Key Takeaway
Femoral neck fractures represent a critical orthopedic challenge, demanding precise anatomical reduction and stable fixation to mitigate risks of osteonecrosis and nonunion. This comprehensive guide details the biomechanical principles, diagnostic protocols, and surgical management of these injuries. From the Garden and Pauwels classifications to advanced reduction maneuvers and implant selection, it provides orthopedic surgeons with evidence-based strategies to optimize patient outcomes in both joint-preserving and arthroplasty procedures.
Introduction to Femoral Neck Fractures
Femoral neck fractures remain one of the most challenging and frequently encountered injuries in orthopedic traumatology. Often termed the "unsolved fracture," these injuries demand a profound understanding of hip biomechanics, vascular anatomy, and patient-specific physiological factors. The management of femoral neck fractures is strictly dictated by the patient's age, baseline functional status, bone quality, and the precise anatomical characteristics of the fracture.
In the young, high-energy trauma patient, a femoral neck fracture is an absolute orthopedic emergency requiring urgent anatomic reduction and stable internal fixation to preserve the native femoral head. Conversely, in the geriatric population, these fractures typically result from low-energy falls and are associated with significant morbidity and mortality, often necessitating arthroplasty to allow for immediate weight-bearing and rapid mobilization.
Vascular Anatomy and Biomechanics
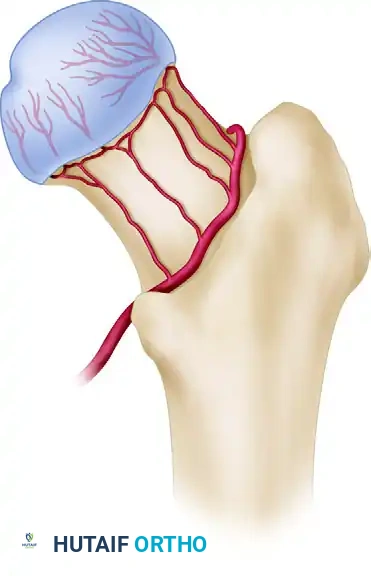
A thorough comprehension of the vascular supply to the proximal femur is paramount, as the disruption of this delicate network directly correlates with the high incidence of osteonecrosis (avascular necrosis) and nonunion following femoral neck fractures.
The primary blood supply to the femoral head is derived from the medial femoral circumflex artery (MFCA) and, to a lesser extent, the lateral femoral circumflex artery. The MFCA gives rise to the extracapsular arterial ring at the base of the femoral neck. From this ring, the ascending cervical arteries travel proximally along the femoral neck within the retinacular folds, ultimately penetrating the joint capsule to form the subsynovial intracapsular arterial ring. The lateral epiphyseal arterial group, a critical terminal branch, supplies the majority of the superior and lateral weight-bearing dome of the femoral head.
Surgical Warning: The intracapsular nature of femoral neck fractures means that the fracture hematoma is contained within the joint capsule, leading to a tamponade effect that can further compromise the tenuous epiphyseal blood supply. Prompt reduction and capsulotomy (or capsular decompression) are critical in joint-preserving surgeries to restore perfusion.
Classification Systems
Classification of femoral neck fractures is essential for standardizing communication, guiding treatment algorithms, and predicting clinical outcomes. Several systems are utilized based on anatomic location, displacement, and biomechanical orientation.
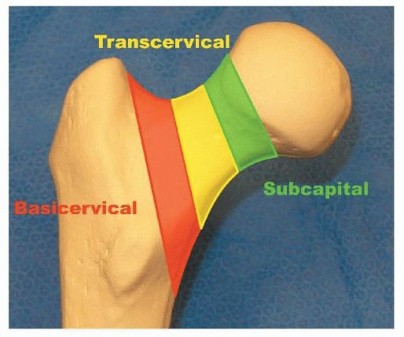
Anatomic Location
Fractures are initially described by their precise location along the femoral neck:
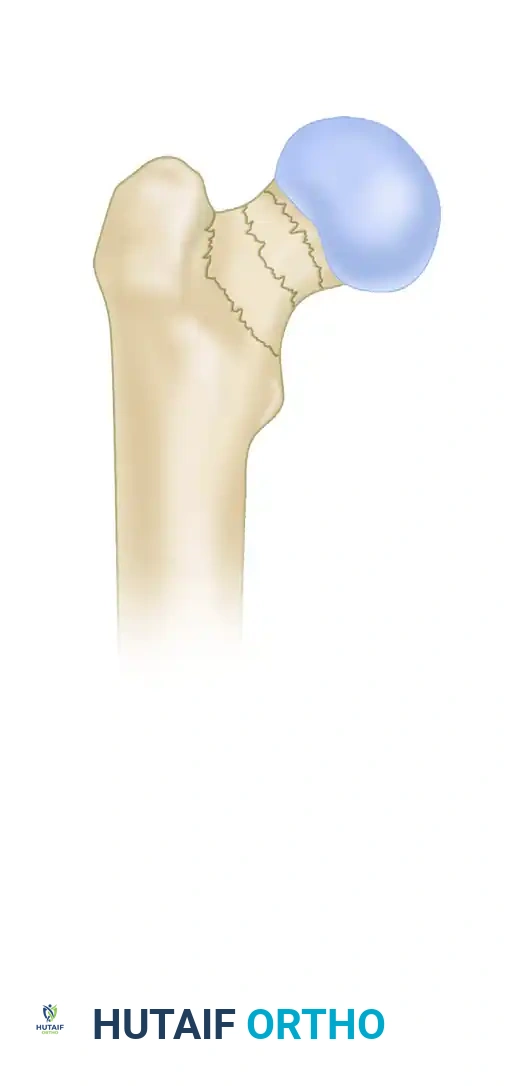
* Subcapital: Occurring immediately distal to the articular cartilage of the femoral head.
* Transcervical: Occurring through the mid-portion of the femoral neck.
* Basicervical: Occurring at the base of the femoral neck, at its junction with the intertrochanteric line. These fractures often behave biomechanically more like intertrochanteric fractures and may require different fixation strategies (e.g., sliding hip screws).
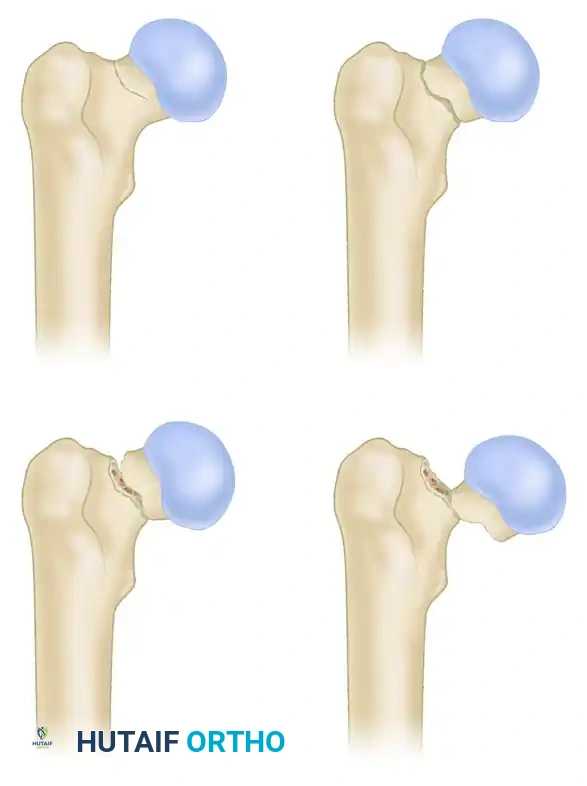
Garden Classification
The Garden classification is the most widely used system for subcapital and transcervical fractures. It is based on the degree of displacement observed on the anteroposterior (AP) radiograph and infers the integrity of the posterior retinacular vessels.
- Stage I: Incomplete or valgus-impacted fracture. The trabecular lines of the femoral head are tilted into valgus.
- Stage II: Complete fracture, but non-displaced. The trabecular lines are interrupted but not angulated.
- Stage III: Complete fracture, partially displaced. The femoral head tilts into varus, causing the trabecular lines to be out of alignment with the acetabulum.
- Stage IV: Complete fracture, fully displaced. The femoral head is completely dissociated from the neck and may realign itself within the acetabulum, paradoxically making the trabecular lines appear parallel to the pelvic trabeculae.
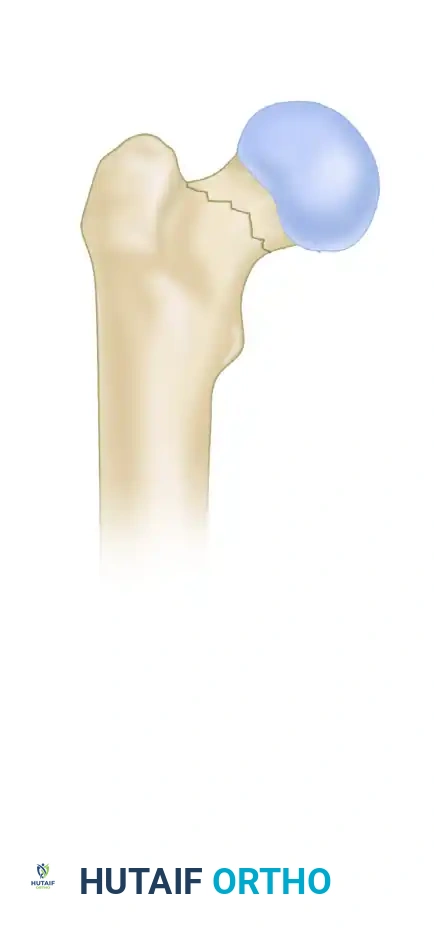
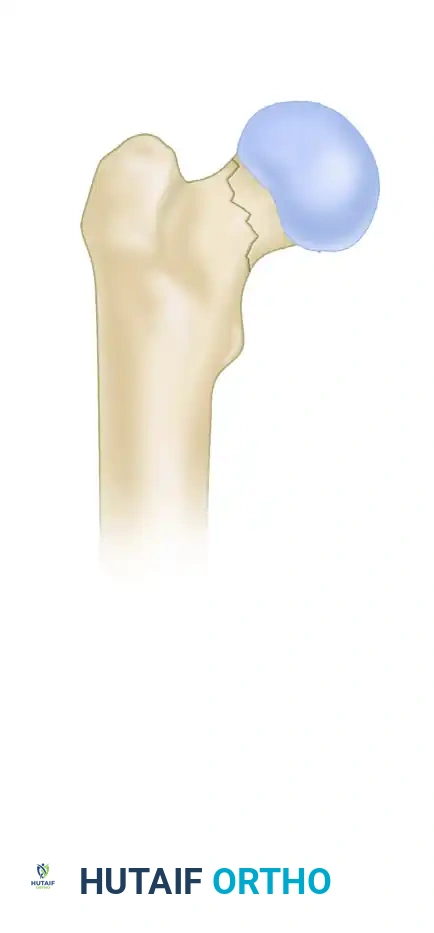
Pauwels Classification
The Pauwels classification evaluates the biomechanical stability of the fracture based on the angle of the fracture line relative to the horizontal plane. As the angle increases, the shear forces across the fracture site increase, elevating the risk of fixation failure and nonunion.
-
Type I: Fracture line is less than 30 degrees from the horizontal. Compressive forces predominate, making this a highly stable pattern.
-
Type II: Fracture line is between 30 and 50 degrees. A combination of shear and compressive forces exists.

-
Type III: Fracture line is greater than 50 degrees. Shear forces dominate, resulting in a highly unstable fracture that often requires more robust fixation constructs, such as a sliding hip screw or a proximal femoral locking plate, rather than standard cannulated screws.
Clinical Diagnosis and Imaging
The diagnosis of a femoral neck fracture relies on a meticulous history, physical examination, and appropriate radiographic imaging.
Clinical Presentation
Most patients present following a traumatic event. In the elderly, this is typically a low-energy fall from a standing height. In younger patients, high-energy trauma (e.g., motor vehicle collisions, falls from height) is the usual mechanism, and these patients must be evaluated according to Advanced Trauma Life Support (ATLS) protocols.
Physical examination classically reveals an extremity that is shortened and externally rotated. This deformity occurs because the iliopsoas muscle pulls the lesser trochanter anteriorly and proximally, while the gluteus medius and minimus abduct the proximal fragment.
Clinical Pearl: Patients with stress fractures or non-displaced (Garden I/II) fractures may not exhibit classic deformity and may even be able to bear weight. The index of suspicion must remain extremely high, as a missed non-displaced fracture can catastrophically displace, drastically altering the surgical options and prognosis.
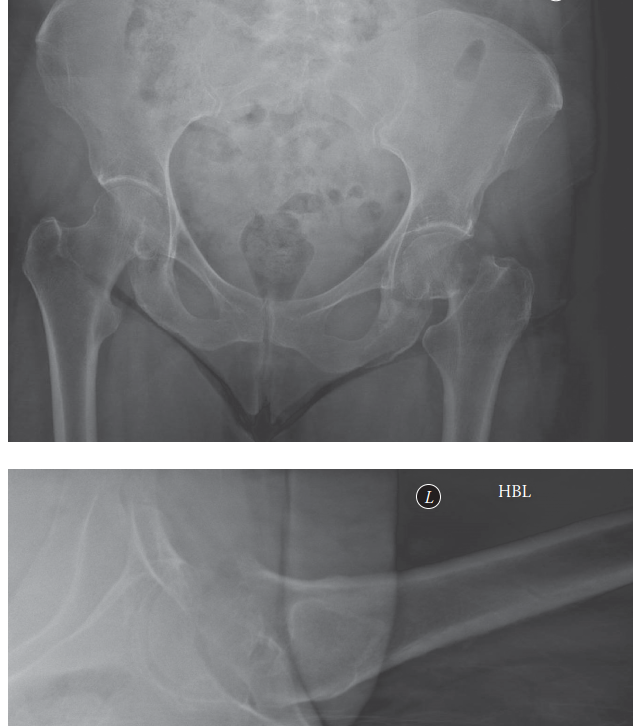
Radiographic Evaluation
Standard imaging includes:
1. Anteroposterior (AP) Pelvis: Allows for comparison with the contralateral normal hip.
2. Cross-table Lateral View: Essential for evaluating anterior or posterior displacement and comminution.
3. Traction Internal Rotation View: Often helpful to overcome the external rotation deformity and better delineate the fracture pattern and true neck length.
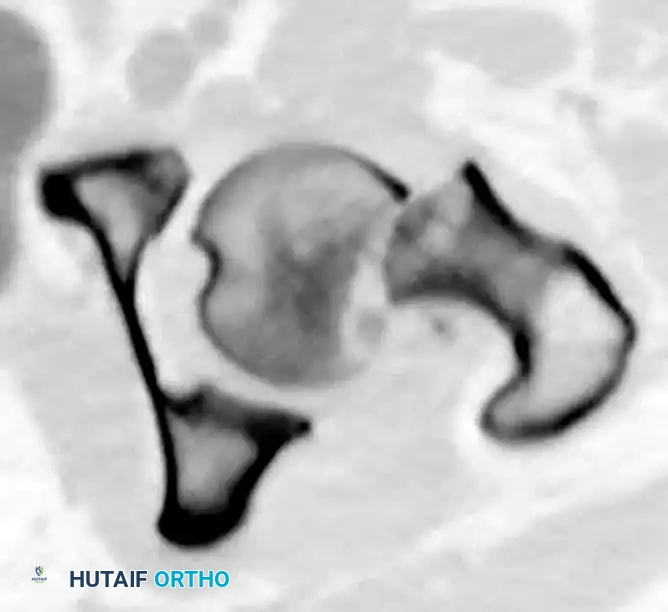
If radiographs are negative but clinical suspicion remains high (occult fracture), Magnetic Resonance Imaging (MRI) is the gold standard. It is highly sensitive and specific for detecting trabecular edema and occult fracture lines. While Computed Tomography (CT) is not routinely ordered for isolated femoral neck fractures, it is highly valuable for assessing comminution, particularly in basicervical patterns, or when evaluating a polytrauma patient where a pan-scan has already been obtained.
Principles of Treatment and Reduction
A satisfactory, anatomic reduction is paramount in minimizing the complications associated with the treatment of femoral neck fractures. Malreduction, particularly varus malalignment, exponentially increases the risk of fixation failure, nonunion, and osteonecrosis.
Closed Reduction Techniques
A closed reduction should be attempted in every patient for whom internal fixation is planned. The classic Whitman technique is performed on a fracture table:
1. Apply longitudinal traction to the limb.
2. Abduct and extend the hip to disengage the fracture fragments.
3. Internally rotate the limb to lock the fracture into place.
Surgical Warning: Reduction attempts must be gentle and controlled. Forceful or repeated manipulations (more than two or three attempts) can cause further iatrogenic damage to the remaining intact retinacular vessels, sealing the fate of the femoral head to osteonecrosis. If closed reduction fails, the surgeon must proceed immediately to an open reduction.
Evaluating the Reduction
Intraoperative fluoroscopy is used to critically evaluate the reduction before any hardware is placed.
The Garden Alignment Index
This index evaluates the alignment of the compressive trabeculae of the femoral head relative to the medial cortex of the femoral shaft.
* Ideal Alignment: On the AP view, the angle should measure exactly 160 degrees.
* Valgus Malalignment: An angle greater than 180 degrees indicates excessive valgus, which can lead to superior joint penetration by hardware as the fracture settles.

* Varus Malalignment: An angle less than 160 degrees (e.g., 150 degrees) indicates varus. This is the most dangerous malreduction, as it converts compressive forces into shear forces, almost guaranteeing fixation failure.

On the lateral image, the angulation should be approximately 180 degrees. Deviation of more than 20 degrees indicates excessive anteversion or retroversion and is unacceptable.
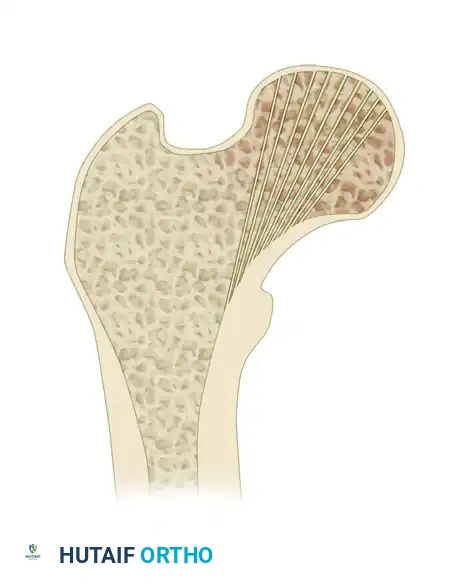
Trabecular Alignment and Lowell's S-Curves
Beyond the Garden Index, the trabecular alignment pattern must be scrutinized. The medial compressive trabeculae should flow seamlessly from the femoral head into the calcar femorale.

Lowell et al. described the fluoroscopic appearance of an anatomically reduced femoral neck as forming "shallow S- or reverse S-shaped curves" along the superior and inferior cortices. These curves are highly sensitive indicators of rotational alignment and may be more practically useful intraoperatively than measuring specific angles.
Operative Treatment Strategies
Operative intervention is the standard of care for nearly all femoral neck fractures. Non-operative management is strictly reserved for non-ambulatory, severely infirm patients at high risk for perioperative mortality, or for stable, compression-sided stress fractures.
Implant Choice and Surgical Decision Making
The choice of implant is dictated primarily by the patient's physiological age, bone quality, and fracture pattern.
1. Internal Fixation (Joint Preservation)
Younger patients (typically < 60-65 years) with displaced or non-displaced fractures, and older patients with strictly non-displaced (Garden I/II) fractures, are treated with internal fixation. The goal is absolute stability to allow for revascularization and bony union.
Cannulated Screw Fixation:
The standard construct involves three 6.5mm or 7.0mm partially threaded cannulated screws placed in an inverted triangle configuration.
* The inferior screw is placed first, resting directly on the dense bone of the calcar femorale to resist varus collapse.
* The anterior and posterior screws are placed superiorly to resist rotational forces.
Sliding Hip Screws (SHS):
For basicervical fractures or vertical shear patterns (Pauwels Type III), a sliding hip screw with a derotational screw provides superior biomechanical stability against shear forces compared to multiple cannulated screws.
Surgical Progression for Internal Fixation:
The following diagrams illustrate the progression of guide wire placement, measurement, and final screw insertion to achieve stable osteosynthesis.

Initial guide wire placement targeting the inferior calcar and central femoral head.
Placement of the superior guide wires to form the inverted triangle configuration.

Measuring for screw length. Screws must be advanced to within 5mm of the subchondral bone to maximize purchase in the dense trabeculae.

Final seating of the partially threaded cannulated screws, allowing for dynamic compression across the fracture site.
2. Arthroplasty (Joint Replacement)
Older patients (typically > 65-70 years) with displaced (Garden III/IV) fractures are best treated with arthroplasty. Internal fixation in this demographic carries an unacceptably high failure rate (up to 30-40%) due to poor bone stock and compromised healing capacity.
- Hemiarthroplasty: Historically the workhorse for the elderly, low-demand community ambulator. It replaces the femoral head while retaining the native acetabulum. Controversy exists regarding the use of unipolar versus bipolar heads, and cemented versus cementless stems. However, cemented stems generally demonstrate fewer periprosthetic fractures and less thigh pain in osteoporotic bone.
- Total Hip Arthroplasty (THA): Recent high-level evidence indicates that active, independent community ambulators have superior functional outcomes, less pain, and lower reoperation rates with THA compared to hemiarthroplasty.
Surgical Approaches for Arthroplasty:
While the posterior approach is traditional and provides excellent exposure, it carries a higher risk of postoperative dislocation in the fracture population. Consequently, the anterior (Smith-Petersen) or anterolateral (Watson-Jones) approaches have gained significant traction, as they exploit internervous planes and theoretically reduce dislocation rates by preserving the posterior capsular restraints.
Postoperative Protocols and Complications
Rehabilitation
- Internal Fixation: Patients are typically restricted to toe-touch or partial weight-bearing for 6 to 12 weeks to prevent hardware cutout and varus collapse, particularly in Pauwels III patterns.
- Arthroplasty: Patients are allowed immediate weight-bearing as tolerated. Early mobilization is critical to prevent deep vein thrombosis (DVT), pulmonary embolism, pneumonia, and decubitus ulcers.
Complications
- Osteonecrosis (AVN): Occurs in 10-30% of internally fixed displaced fractures. It may present months to years postoperatively with groin pain and segmental collapse. Treatment usually requires conversion to THA.
- Nonunion: Occurs in up to 15% of cases. Risk factors include varus malreduction, inadequate fixation, and smoking.
- Failure of Fixation: Hardware cutout or back-out, often secondary to unrecognized varus settling or severe osteoporosis.
- Dislocation: A significant risk following THA for fracture, necessitating meticulous surgical technique, capsular repair, and appropriate postoperative precautions.
In conclusion, the successful management of femoral neck fractures requires a synthesis of biomechanical knowledge, precise surgical execution, and tailored patient care. Whether performing joint-preserving osteosynthesis or arthroplasty, adherence to strict anatomic and biomechanical principles is the cornerstone of optimizing patient outcomes.
You Might Also Like