Mastering Radial Nerve Palsy: Comprehensive Biomechanics, Indications, and Tendon Transfer Techniques

Key Takeaway
Radial nerve palsy results in the debilitating loss of wrist, finger, and thumb extension. Surgical management via tendon transfer restores functional grasp and dexterity. The most reliable combination involves transferring the pronator teres to the extensor carpi radialis brevis, the flexor carpi radialis to the extensor digitorum communis, and the palmaris longus to the rerouted extensor pollicis longus. Proper tensioning and postoperative rehabilitation are critical for optimal outcomes.
PERIPHERAL NERVE PALSIES: RADIAL NERVE PALSY
Radial nerve injuries present a profound functional deficit to the upper extremity, primarily characterized by the loss of wrist extension, finger metacarpophalangeal (MCP) joint extension, and thumb extension and radial abduction. While radial nerve injuries rarely occur at sites other than the humeral shaft or the proximal third of the forearm, the resulting paralysis severely compromises the hand's spatial positioning and power grip.
Understanding the nuanced differences between high and low radial nerve paralyses, the biomechanics of wrist motion, and the precise indications for tendon transfer is paramount for the reconstructive orthopedic surgeon.
Pathoanatomy and Biomechanics of the Paralyzed Hand
Injuries to the radial nerve at a high level (proximal to the elbow) typically spare triceps function, preserving elbow extension. However, predictable motor paralysis results in the complete loss of wrist extension, thumb extension/abduction, and finger MCP joint extension.
Clinical Pearl: Wrist extension is the biomechanical cornerstone for proper flexor tendon tensioning. Without it, the tenodesis effect is lost, grasp is profoundly reduced, and the hand suffers a significant functional deficit.
More distal nerve injuries (e.g., posterior interosseous nerve syndrome) result in a "low" radial nerve palsy. This is characterized by the preservation of wrist extension (due to an intact extensor carpi radialis longus [ECRL]); however, the loss of thumb extension/abduction and finger MCP joint extension prevents appropriate grasp posture, leading to striking awkwardness and clumsiness.
The Dart-Throwing Motion and Power Grip
Normal wrist motion operates along an oblique axis—from dorsoradial extension to volarulnar flexion—commonly referred to as the "dart-throwing motion." Elimination of the extensor carpi ulnaris (ECU) and extensor carpi radialis brevis (ECRB) balancing forces may accentuate radial deviation of the hand and disturb this normal flexion-extension arc.
Furthermore, the optimal wrist position for power grip requires ulnar deviation and extension. Sacrificing the flexor carpi ulnaris (FCU) as a donor tendon can severely compromise grip strength.
Surgical Warning: In patients who exhibit significant wrist radial deviation prior to tendon transfer, the use of the FCU as a donor is strictly contraindicated. The FCU is the major wrist flexor and the only remaining ulnar deviator of the wrist when the ECU is paralyzed.
Indications and Timing for Surgical Intervention
Observation is the gold standard for most radial nerve palsies associated with closed humeral shaft fractures, as spontaneous return of normal function can be anticipated in 70-80% of cases within 3 to 6 months.
Early surgical exploration for the classic Holstein-Lewis fracture pattern (a spiral fracture of the middle-distal third junction of the humerus) remains controversial but is generally not indicated acutely unless the palsy occurs after a closed reduction attempt. Studies demonstrate that patients with this pattern often achieve full recovery regardless of early nerve exploration. The indications for open reduction and internal fixation (ORIF) of acute closed humeral fractures should rely on orthopedic fracture parameters rather than the isolated status of the radial nerve.
Timing for Nerve Exploration:
* Closed Injuries: Surgical exploration is indicated at 3 to 4 months post-injury in the absence of clinical or electromyographic (EMG) nerve recovery, or an advancing Tinel's sign.
* Open Injuries: Nerve exploration should accompany the acute management of open humeral fractures and penetrating lacerations. Radial nerve neurorrhaphy should be performed primarily when possible. Outcomes are theoretically favorable because the nerve is largely motor, and the distance between the injury site and the motor endplates (brachioradialis, ECRL) is relatively short.
The Role of Early Tendon Transfer
When nerve repair is performed, tendon transfers are traditionally delayed for 6 to 12 months to allow for reinnervation. However, Burkhalter outlined three distinct indications for early tendon transfer (specifically, Pronator Teres to ECRB):
1. Internal Splinting: To act as a substitute during the prolonged regrowth of the nerve, eliminating the need for cumbersome external orthoses.
2. Motor Assistance: To act as a helper as reinnervation proceeds, maintaining cortical integration of wrist extension.
3. Definitive Salvage: To intervene early when the results of nerve repair are anticipated to be poor or the nerve is deemed irreparable.
Burkhalter contended that early transfer of the pronator teres (PT) to establish wrist extension creates no donor site disability, as the transferred unit continues to function synergistically as a forearm pronator.
Tendon Transfer Options and Variations
Despite numerous historical variations, modern tendon transfer combinations for radial nerve paralysis rely on retaining at least one strong wrist flexor to prevent debilitating wrist hyperextension.
1. The Standard Transfer (PT, FCR, PL)
Most hand surgeons prefer utilizing the flexor carpi radialis (FCR) over the FCU to establish MCP joint extension. This preserves the FCU for power grip and ulnar deviation. Scuderi modified Starr’s original transfer by utilizing the palmaris longus (PL) to the extensor pollicis longus (EPL) to provide thumb extension and abduction.
2. The Boyes Transfer (Sublimis Transfer)
To achieve full and independent thumb and digital extension, Boyes devised transfers utilizing the flexor digitorum sublimis (FDS) tendons of the middle and ring fingers.
* PT to ECRL and ECRB
* FCR to EPB and APL
* Middle FDS to EDC
* Ring FDS to EPL and EIP
Critique: These transfers are technically demanding. A significant complication is the development of dense adhesions in the interosseous space through which the sublimis tendons are routed.
3. The Brand Modification
Brand suggested addressing the radial deviation seen in low radial nerve palsies by removing the insertion of the ECRL and transferring it to a centralized point between the ECRB and ECU. Today, most surgeons attempt to balance the wrist by transferring the PT directly into the more centrally located ECRB, rather than the ECRL.
SURGICAL TECHNIQUE: Standard Triple Transfer for Radial Nerve Palsy
Procedure: Transfer of the Pronator Teres (PT) to the Extensor Carpi Radialis Brevis (ECRB), the Flexor Carpi Radialis (FCR) to the Extensor Digitorum Communis (EDC), and the Palmaris Longus (PL) to the Extensor Pollicis Longus (EPL).
Anesthesia and Positioning:
All procedures are performed under general anesthesia or a regional axillary block with the patient positioned supine. A high arm pneumatic tourniquet is utilized. The hand, forearm, and elbow are prepped and draped widely to allow full excursion of the joints.
Step 1: Dorsal Exposure and Recipient Tendon Preparation
Make a gently curved incision in the middle third of the dorsal forearm to expose the extensor pollicis longus (EPL), the common extensor tendons (EDC), and the extensor indicis proprius (EIP) proximal to the extensor retinaculum.
Dorsal incision utilized for the exposure of the recipient extensor tendons.
Flex the fingers fully and hold the wrist in extension. Sequentially secure the EDC and EIP tendons together under equal tension proximal to the extensor retinaculum. Use 2-0 nonabsorbable braided sutures.
Surgical Pitfall: Ensure the suture site does not impinge on the proximal edge of the extensor retinaculum during maximal excursion, which would severely limit finger flexion when the wrist is flexed.
Place the wrist in neutral and evaluate synchronous MCP joint extension by placing traction on the EDC/EIP tendon composite. Additional extensor tendon balancing may be required by adjusting tension with mattress sutures between the individual slips. Inclusion of the extensor digiti minimi (EDM) may be necessary if small finger lag is noted.
Step 2: Volar Exposure and Donor Tendon Harvest
Make a gently curved volar incision, extending from the junction of the proximal-middle third of the forearm to 4 cm proximal to the distal wrist flexion crease. This exposes the PT, FCR, and PL musculotendinous units.

Volar incision extending along the forearm to harvest the Pronator Teres, Flexor Carpi Radialis, and Palmaris Longus.
Locate the interval between the brachioradialis and pronator teres. Trace the PT to its insertion on the radial shaft. Sharply free the PT from the radius, harvesting as much periosteal extension as possible (typically 2 to 3 cm) in continuity with the tendinous insertion to maximize length.
Transfer of the PT into the more centralized ECRB. Note the PT insertion is harvested with a crucial 2- to 3-cm periosteal extension strip to ensure adequate length for the weave.
Trace the FCR distally. With the wrist flexed to relieve tension, transect the FCR exactly at the level of the distal wrist crease. Verify the presence of the PL (absent in ~15% of the population), trace its tendon distally, and divide it at the distal wrist flexion crease.
Elevate and dissect these three motor units proximally, releasing their fascial attachments to ensure a straight line of pull toward their intended dorsal insertions.
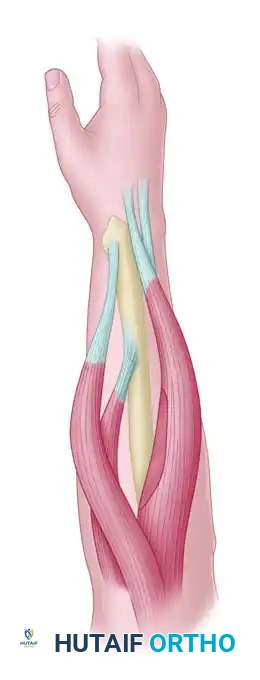
Step 3: Rerouting the Extensor Pollicis Longus (EPL)
Transect the EPL at its musculotendinous junction in the dorsal wound. Make a separate 2-cm transverse incision dorsally, just proximal to the thumb MCP joint. Release fascial attachments to deliver the distal EPL stump into this wound.
Make another 2-cm transverse incision in the distal wrist flexion crease at the base of the thenar eminence. Create a subcutaneous tunnel to pass the EPL volar and radial to the thumb carpometacarpal (CMC) joint.

Preparation for the transfer of the PL to the rerouted EPL. The EPL is transposed out of the third dorsal compartment.
By rerouting the EPL out of its native third extensor compartment and positioning it volarly, the new line of pull will provide simultaneous interphalangeal joint extension and palmar abduction.
Completion of the PL to EPL transfer. The combination of thumb abduction and extension is achieved through this modified vector.
Tunnel the EPL tendon proximally to the main volar wound. Effortless excursion must be achieved; release any residual fascial bands. Assess the desired thumb radial abduction and IP joint extension by placing traction on the free rerouted EPL tendon in line with the PL toward the medial epicondyle. Wrap the tendon in a moist sponge.
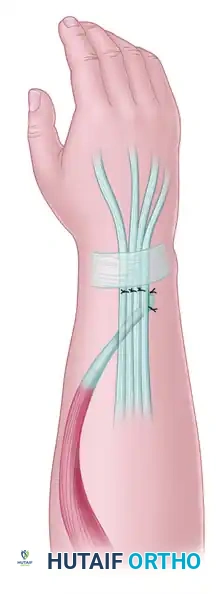
Step 4: Tendon Routing and Weaving
Develop wide subcutaneous tunnels from the proximal volar incision to the distal dorsal incision. Maintain a straight-line approach for the PT and FCR motors.
Surgical Warning: Route the tendons dorsally around the radial shaft with extreme care to avoid compressing the radial artery or the superficial sensory branch of the radial nerve (SBRN).

Subcutaneous routing of the donor tendons from the volar to the dorsal aspect of the forearm, ensuring a straight line of pull.
Place the FCR tendon through the EDC/EIP tendon composite in a proximal-radial to distal-ulnar direction. Adjust the tension meticulously: with full passive wrist flexion, the MCP joints must extend fully; with full passive wrist extension, the fingers must be able to be passively flexed into the palm.
Because a traditional Pulvertaft weave is often impossible due to the bulk of the EDC, use multiple horizontal mattress sutures (2-0 braided nonabsorbable) to anchor the FCR tendon to each individual slip of the EDC/EIP composite at a 45-degree angle.
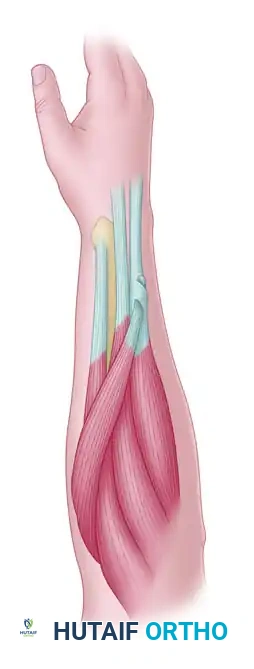
FCR transfer to the EDC. The FCR motor tendon is attached at a 45-degree angle into the recipient tendon composite using multiple mattress sutures.
Next, weave the PT tendon and its periosteal slip through the ECRB tendon. The PT and ECRB can be joined by several passes of the PT through the recipient ECRB. Secure the weave with the wrist held in 40 degrees of extension, placing the PT under near-maximal tension.

Final construct demonstrating the centralized pull of the PT to ECRB, restoring robust wrist extension without inducing radial deviation.
Finally, weave and suture the EPL and PL tendons together. Place traction on the construct in line with the PL and verify thumb palmar abduction and IP extension. The tension should permit passive flexion of the thumb across the palm when the wrist is in a neutral position.
Deflate the tourniquet, achieve meticulous hemostasis, and close the wounds in a routine layered fashion.
Alternative: Utilizing the Flexor Carpi Ulnaris (FCU)
When the FCU is selected instead of the FCR for digital extension (only if no radial deviation is present), the volar forearm incision must extend to the distal wrist flexion crease over the ulnar aspect. The FCU is detached near the pisiform. The proximal dissection is more tedious as the FCU is muscular throughout its length. In thin patients, transferring the bulky FCU around the subcutaneous border of the ulna can be cosmetically objectionable; this can be mitigated by resecting the distal muscle belly prior to transfer.
POSTOPERATIVE CARE AND REHABILITATION
The success of a tendon transfer relies as much on meticulous postoperative rehabilitation as it does on surgical execution.
Phase I: Immobilization (Weeks 0-3)
* The upper extremity is immobilized in a bulky, rigid cast or custom orthosis.
* Positioning: The wrist is immobilized in 40 to 45 degrees of extension. The finger MCP joints are placed in full extension (0 degrees), with the interphalangeal joints left free to prevent intrinsic contractures. The thumb is immobilized in maximal radial abduction and extension.
* Sutures are removed at 10 to 14 days, but strict immobilization is maintained for a full 3 weeks to allow for primary tendon healing at the weave sites.
Phase II: Early Active Motion (Weeks 3-6)
* At 3 weeks, supervised hand therapy is initiated.
* A removable, custom-molded thermoplastic splint is fabricated, maintaining the wrist, fingers, and thumb in the postoperative extended position.
* The splint is worn at all times, including at night, and is only removed for targeted therapy sessions.
* Therapy focuses on active synergistic motion. Patients are taught to flex the wrist to achieve passive finger extension (tenodesis training) and to actively fire the transferred muscles (e.g., pronating the forearm to facilitate wrist extension).
Phase III: Strengthening and Weaning (Weeks 6-12)
* At 6 weeks, passive stretching and gentle strengthening exercises are introduced.
* The daytime splint is gradually weaned, though night splinting may continue until 12 weeks postoperatively to prevent stretching of the transfers.
* Full unrestricted activity and heavy lifting are generally restricted until 3 to 4 months postoperatively, ensuring the tendon weaves have achieved maximal tensile strength.
📚 Medical References
- Radial nerve palsy associated with humeral shaft fracture: evaluation with US— initial experience, Radiology 219:811, 2001.
- Chapman JR, Henley B, Agel J, et al: Randomized prospective study of humeral shaft fracture fi xation: intramedullary nails versus plates, J Orthop Trauma 14:162, 2000.
- Cox MA, Dolan M, Synnott K, et al: Closed interlocking nailing of humeral shaft fractures with the Russell-Taylor nail, J Orthop Trauma 14:349, 2000.
- Dabezies EJ, Banta CJ II, Murphy CP, et al: Plate fi xation of the humeral shaft for acute fractures, with and without radial nerve injuries, J Orthop Trauma 6:10, 1992.
- Dijkstra S, Stapert J, Boxma H, et al: Treatment of pathological fractures of the humeral shaft due to bone metastases: a comparison of intramedullary locking nail and plate osteosynthesis with adjunctive bone cement, Eur J Surg Oncol 22:621, 1996.
- Ekholm R, Adami J, Tidermark J, et al: Fractures of the shaft of the humerus: an epidemiological study of 401 fractures, J Bone Joint Surg 88B:1469, 2006.
- Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: a review, J Orthop Trauma 13:258, 1999.
- Fernandez FF, Matschke S, Hülsenbeck A, et al: Five years’ clinical experience with the unreamed humeral nail in the treatment of humeral shaft fractures, Injury 35:264, 2004.
- Fjalestad T, Stromsoe K, Salvesen P, et al: Functional results of braced humeral diaphyseal fractures: why do 38% lose external rotation of the shoulder? Arch Orthop Trauma Surg 120:281, 2000.
- Flinkkilä T, Hyvönen P, Siira P, et al: Recovery of shoulder joint function after humeral shaft fracture: a comparative study between antegrade intramedullary nailing and plate fi xation, Arch Orthop Trauma Surg 124:537, 2004.
- Foster RJ, Dixon GL Jr, Bach AW, et al: Internal fi xation of fractures and non-unions of the humeral shaft. Indications and results in a multi-center study, J Bone Joint Surg 67A:857, 1985.
- Franck WM, Olivieri M, Jannasch O, et al: Expandable nail system for osteoporotic humeral shaft fractures: preliminary results, J Trauma 54:1152, 2003.
- Gerber C, Schneeberger AG, Vinh TS: The arterial vascularization of the humeral head: an anatomical study, J Bone Joint Surg 72A:1486, 1990.
- Gerwin M, Hotchkiss RN, Weiland SJ: Alternative operative exposures of the posterior aspect of the humeral diaphysis, with reference to the radial nerve, J Bone Joint Surg 78A:1690, 1996.
- Gustilo RB: Current concepts in the management of
You Might Also Like

