Tendon Transfers for Thumb Adduction and Index Finger Abduction
Key Takeaway
Restoration of thumb adduction and index finger abduction is critical for restoring key pinch and grip strength following ulnar nerve palsy or poliomyelitis. The Smith technique utilizes the extensor carpi radialis brevis (ECRB) prolonged with a tendon graft to reconstruct the adductor pollicis. Concurrently, restoring the first dorsal interosseous function via extensor indicis proprius (EIP) transfer stabilizes the index finger, providing a rigid post for effective thumb opposition and pinch kinematics.
INTRODUCTION TO INTRINSIC PARALYSIS OF THE HAND
The loss of intrinsic muscle function in the hand, most commonly secondary to ulnar nerve palsy, poliomyelitis, or severe brachial plexus trauma, results in profound biomechanical deficits. Among the most debilitating of these deficits is the loss of thumb adduction and index finger abduction. The adductor pollicis (AP) and the first dorsal interosseous (FDI) muscles work synergistically to provide the powerful key pinch required for activities of daily living.
Without the adductor pollicis, the thumb cannot forcefully approximate the index finger, leading to compensatory hyperflexion of the thumb interphalangeal (IP) joint via the flexor pollicis longus (Froment’s sign) and hyperextension of the metacarpophalangeal (MCP) joint (Jeanne’s sign). Furthermore, without the stabilizing force of the first dorsal interosseous, the index finger collapses under the pressure of the thumb, rendering pinch weak and ineffective.
Surgical restoration of these functions requires meticulous tendon transfer techniques. The Smith technique, utilizing the extensor carpi radialis brevis (ECRB) prolonged with a tendon graft, is a highly effective method for restoring thumb adduction. Concurrently, transferring a donor tendon to the first dorsal interosseous insertion restores index finger abduction, re-establishing the stable "post" necessary for functional pinch.
BIOMECHANICAL PRINCIPLES AND PREOPERATIVE EVALUATION
The Kinematics of Key Pinch
Key pinch (lateral pinch) relies on a stable kinematic chain. The adductor pollicis provides approximately 80% of the adduction force of the thumb. Its transverse and oblique heads originate from the third metacarpal and capitate, inserting onto the ulnar sesamoid and the base of the proximal phalanx of the thumb. This vector pulls the first metacarpal toward the third metacarpal.
The index finger serves as the anvil against which the thumb strikes. The first dorsal interosseous (FDI) abducts the index finger and stabilizes its MCP joint against the ulnarly directed force of the thumb. Paralysis of the FDI results in ulnar deviation of the index finger during pinch attempts.
Preoperative Assessment
Before proceeding with tendon transfer, the surgeon must ensure the following prerequisites are met:
* Supple Joints: The thumb and index finger MCP and IP joints must have full passive range of motion. Any contractures (e.g., first web space contracture) must be released prior to or concomitantly with the tendon transfer.
* Donor Muscle Strength: The proposed donor muscles (ECRB for thumb adduction; Extensor Indicis Proprius [EIP] or Palmaris Longus [PL] for index abduction) must be Medical Research Council (MRC) Grade 5.
* Tissue Equilibrium: The soft tissue envelope must be stable, well-vascularized, and free of active inflammation or infection.
💡 Clinical Pearl: Donor Selection
The ECRB is an excellent donor for thumb adduction because of its high excursion and force-generating capacity. However, utilizing the ECRB requires a tendon graft (usually the palmaris longus) to reach the adductor insertion. Ensure the palmaris longus is present preoperatively by having the patient perform the Schaeffer's test (opposing the thumb and small finger while flexing the wrist).
SURGICAL TECHNIQUE: ECRB TRANSFER TO RESTORE THUMB ADDUCTION (SMITH)
The Smith technique leverages the robust ECRB muscle, routing it through the intermetacarpal space to replicate the exact vector of the paralyzed adductor pollicis.
1. Patient Positioning and Preparation
The patient is placed supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Regional anesthesia (supraclavicular or axillary block) or general anesthesia is administered. The limb is prepped and draped in standard sterile fashion.
2. Incision and Exposure of the ECRB
- Make two dorsal transverse incisions over the extensor carpi radialis brevis tendon proximal to its insertion at the base of the third metacarpal.
- Carefully dissect through the subcutaneous tissue, preserving the dorsal sensory branches of the radial nerve.
- Identify the ECRB tendon. It is located central to the extensor carpi radialis longus (ECRL) and inserts onto the base of the third metacarpal.
3. Tendon Detachment and Retrieval
- Divide the ECRB tendon as distally as possible near its insertion on the third metacarpal base.
- Withdraw the tendon through the more proximal transverse incision, ensuring it is proximal to the dorsal retinaculum to allow for a straight line of pull without tethering.
4. Preparation of the Interosseous Window
- Make a third longitudinal incision on the dorsum of the hand between the second and third metacarpals.
- Dissect down to the interosseous fascia.
- Remove a generous "window" of tissue from the paralyzed dorsal interosseous muscles. This window must be large enough to allow the tendon graft to pass freely without friction or adherence to the surrounding fibrotic muscle tissue.
5. Exposure of the Adductor Pollicis Insertion
- Make a longitudinal incision on the ulnar side of the metacarpophalangeal (MCP) joint of the thumb.
- Identify the ulnar sesamoid and the tendinous insertion of the adductor pollicis onto the base of the proximal phalanx.
6. Tunneling and Graft Harvest
- Using a curved hemostat or tendon passer, create a tunnel deep to the adductor pollicis muscle belly, passing from the thumb MCP incision, through the first web space, and out through the prepared window in the second interosseous space.
- Harvest an appropriate tendon graft. The palmaris longus tendon is the graft of choice due to its length and expendability. If the palmaris longus is absent, a strip of fascia lata or the plantaris tendon may be utilized.
7. Graft Routing and Distal Fixation
- Draw the tendon graft through the created tunnel from the thumb incision to the dorsum of the hand.
- At the thumb MCP joint, weave the distal end of the graft into the tendinous insertion of the adductor pollicis. Secure it using a non-absorbable braided suture (e.g., 3-0 or 4-0 polyester) utilizing a Pulvertaft weave or a robust figure-of-eight technique.
8. Proximal Fixation and Tensioning
- Pass the proximal end of the tendon graft subcutaneously from the intermetacarpal incision to the most proximal incision where the ECRB tendon is resting.
- Tensioning the Transfer: This is the most critical step of the procedure. Suture the graft to the ECRB tendon using a Pulvertaft weave.
- Take up all slack in the system, but apply no excessive tension. The resting posture of the hand should dictate the tension: with the wrist held in a neutral position, the thumb should lie just palmar to the index finger.
⚠️ Surgical Warning: Tensioning
Over-tensioning the ECRB transfer will result in an adduction contracture of the thumb, severely limiting the patient's ability to grasp large objects (loss of span). Under-tensioning will result in a weak pinch. Rely on the tenodesis effect to confirm appropriate tension.
9. Intraoperative Tenodesis Test
- Dorsiflex the wrist: Observe the thumb. It should be pulled smoothly into adduction against the index finger.
- Flex the wrist: The thumb should relax and lie firmly against the palm, allowing for first web space clearance.
- Once tension is confirmed, complete the suturing of the Pulvertaft weave. Close all incisions in layers and apply a sterile dressing.
ALTERNATIVE TECHNIQUES: MODIFIED ROYLE-THOMPSON TRANSFER
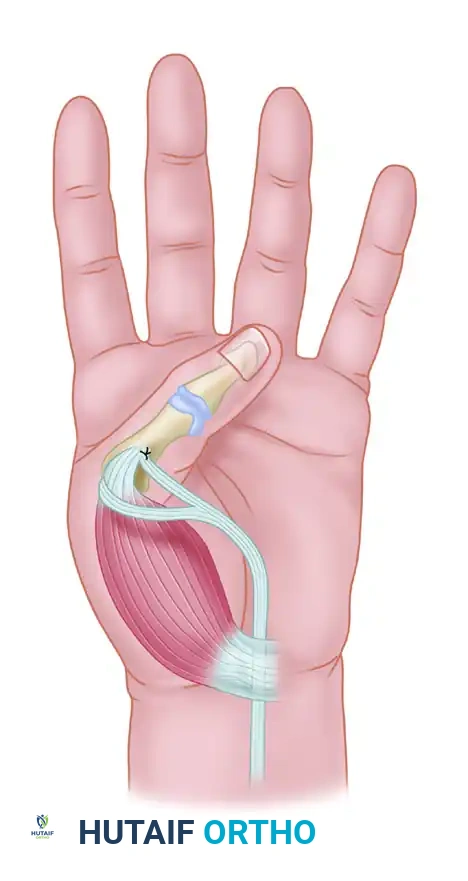
While the Smith technique is highly effective, alternative routing methods exist depending on the availability of donor tendons and the specific anatomical deficits of the patient. The modified Royle-Thompson transfer is another classic technique utilized to restore thumb adduction, often employing the flexor digitorum superficialis (FDS) of the ring finger routed across the palm.
In the modified Royle-Thompson transfer (as illustrated above), the donor tendon is passed deep to the flexor tendons and neurovascular bundles in the palm, utilizing the palmar fascia or a pulley created from the flexor retinaculum to direct the vector of pull transversely toward the adductor insertion on the thumb.
RESTORATION OF ABDUCTION OF THE INDEX FINGER
Biomechanical Rationale
The index finger is the primary digit against which the thumb is brought during pinch. A strong index finger-thumb pinch relies entirely on the stability of the index finger MCP joint. Furthermore, independent abduction of the index finger is especially useful in fine motor activities such as playing a piano, using a keyboard, or manipulating small instruments.
In conditions like poliomyelitis or isolated ulnar nerve palsy, abduction of the index finger is lost. Because its restoration is so critical to overall hand function, it is often considered separately from the intrinsic functions of the other fingers.
Donor Tendon Selection
A transfer to restore index finger abduction acts as a substitute chiefly for the first dorsal interosseous (FDI) muscle. Therefore, the transferred tendon must be attached to the FDI tendon insertion, which is located primarily on the radial base of the index proximal phalanx and the lateral band of the extensor mechanism.
The tendons most frequently transferred include:
1. Extensor Indicis Proprius (EIP): The most common and reliable donor. It provides excellent excursion, appropriate force, and its harvest does not significantly compromise independent index finger extension (as the extensor digitorum communis remains intact).
2. Extensor Pollicis Brevis (EPB): Can be used if the EIP is unavailable, provided thumb extension is fully supported by the extensor pollicis longus.
3. Palmaris Longus (PL): Requires a tendon graft extension (e.g., plantaris) to reach the insertion site, making it a secondary choice.
4. Flexor Digitorum Superficialis (FDS): A sublimis tendon has been used historically; however, this is generally contraindicated unless the hand is otherwise exceptionally strong. Removing an FDS tendon from a hand already weakened by intrinsic paralysis can severely compromise power grip. Note: If thumb opposition must also be restored concurrently, the FDS to the ring finger is often reserved for the opposition transfer (e.g., Burkhalter or Royle-Thompson techniques).
Surgical Technique: EIP to FDI Transfer
- Incision and Harvest: Make a short transverse incision over the dorsal MCP joint of the index finger. Identify the EIP tendon (located ulnar to the EDC tendon). Divide the EIP tendon just proximal to the extensor hood.
- Proximal Retrieval: Make a longitudinal incision over the distal forearm at the level of the extensor retinaculum. Withdraw the EIP tendon into the forearm wound.
- Routing: Create a subcutaneous tunnel from the forearm incision, passing radially around the second metacarpal, to the radial aspect of the index finger MCP joint.
- Fixation: Weave the EIP tendon into the tendinous insertion of the first dorsal interosseous at the radial base of the proximal phalanx.
- Tensioning: Suture the transfer with the index finger held in maximum abduction and the wrist in neutral. The tension should be set slightly tighter than resting tension, as the transfer will stretch slightly during rehabilitation.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
The success of tendon transfers for intrinsic paralysis relies as much on meticulous postoperative rehabilitation as it does on surgical execution.
Phase I: Immobilization (Weeks 0 to 3)
- Immediately postoperatively, the hand and forearm are immobilized in a custom plaster splint or cast.
- Positioning: The wrist is immobilized in 40 degrees of dorsiflexion. The thumb is held in a neutral position (slight palmar abduction and adduction to protect the ECRB-to-AP transfer). The index finger is immobilized in maximum abduction to protect the EIP-to-FDI transfer.
- Elevation and strict edema control are mandatory during this phase.
Phase II: Early Active Motion (Weeks 3 to 6)
- The plaster cast is removed at exactly 3 weeks postoperatively.
- The patient is transitioned to a thermoplastic removable splint that maintains the protective positioning but allows for controlled exercise sessions.
- Active Motion: Active motion is encouraged. The patient is instructed to perform active wrist flexion (which will passively adduct the thumb via the tenodesis effect) and active thumb adduction.
- Biofeedback: Motor relearning is critical. The patient must learn to fire the ECRB (normally a wrist extensor) to achieve thumb adduction. Mirror therapy and surface EMG biofeedback can be highly beneficial.
Phase III: Strengthening and Integration (Weeks 6 and Beyond)
- At 6 weeks, passive stretching is cautiously introduced if joint stiffness is present.
- Progressive resistance exercises are initiated. Pinch gauges and putty are used to strengthen the newly reconstructed key pinch.
- Splinting is gradually discontinued during the day but may be maintained at night until 8-10 weeks postoperatively to prevent stretching of the transfers.
- Full integration into heavy activities of daily living is typically achieved by 12 to 16 weeks.
COMPLICATIONS AND PITFALLS
- Adhesions: The most common complication, particularly where the tendon graft passes through the interosseous window. Ensuring a wide window and initiating early active motion at 3 weeks mitigates this risk.
- Stretching of the Transfer: Often caused by premature aggressive passive stretching or non-compliance with splinting. If the graft stretches, the pinch will remain weak, necessitating potential revision and plication.
- Over-Tensioning: Results in a fixed adducted thumb, preventing the patient from grasping large objects. This is a severe functional deficit that is difficult to correct postoperatively. Strict adherence to the intraoperative tenodesis test is required to prevent this.
- Donor Site Morbidity: Loss of independent index extension (if EIP is used) or slight weakness in wrist extension (from ECRB harvest). These are generally well-tolerated and clinically insignificant if preoperative muscle grading was accurate.
You Might Also Like

