Masterclass in Flexor Tendon Examination and Advanced Repair Techniques
Key Takeaway
Evaluation of hand injuries requires meticulous neurovascular and biomechanical assessment. Flexor tendon injuries disrupt the normal resting cascade, necessitating precise surgical intervention. This guide details evidence-based tendon repair techniques, emphasizing Strickland’s principles, optimal suture materials, and advanced core configurations like the 4-strand cruciate and modified Kessler. Mastery of these techniques ensures robust repairs capable of withstanding early active motion protocols, minimizing adhesions, and optimizing functional recovery.
INTRODUCTION TO FLEXOR TENDON EVALUATION
The evaluation of a patient with an injured hand demands a systematic, highly disciplined approach. It begins with the standard Advanced Trauma Life Support (ATLS) assessment of the patient’s general condition to exclude life-threatening injuries, followed by a focused examination of the affected extremity. High-quality orthogonal radiographs are mandatory to exclude associated fractures, foreign bodies, or joint subluxations.
Crucially, a meticulous examination of the neurovascular status of the hand must precede any evaluation of tendon function. Digital nerve injuries frequently accompany flexor tendon lacerations due to their close anatomic proximity. Assessing two-point discrimination and digital perfusion before manipulating the hand prevents iatrogenic injury and establishes a vital baseline.
The Resting Cascade and Postural Clues
Even in the absence of gross deformity, the resting posture of the hand provides immediate, highly reliable clues regarding severed flexor tendons. Traditionally, in hand surgery, "the finger points the way" toward the injured structures.
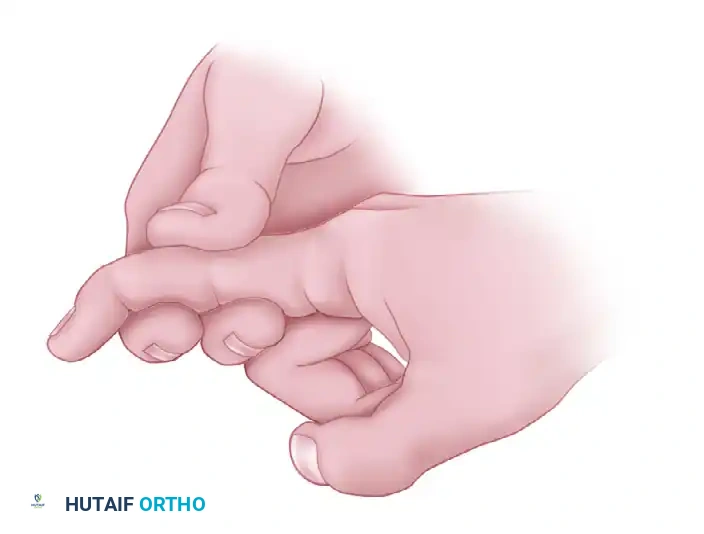
When a normal hand rests supinated, the fingers assume a natural cascade of increasing flexion from the index to the small finger, driven by the resting tone of the flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS).
When both flexor tendons of a finger are severed, this resting tone is lost. The affected digit lies in an unnatural position of relative hyperextension compared to the adjacent uninjured fingers.
Clinical Pearl: Errors are common when examining flexor tendon injuries. Active movements by the patient or passive manipulation by the examiner can elicit severe pain, limiting motion and creating false-positive functional deficits. Always interpret active motion tests in the context of the patient's pain tolerance.
Passive and Active Provocative Maneuvers
Flexor tendon injuries can be tentatively confirmed through passive maneuvers utilizing the tenodesis effect. Passive extension of the wrist normally produces spontaneous flexion of the fingers. If the flexor tendons are severed, this tenodesis flexion is absent.
To isolate and test specific tendons, active maneuvers are employed:
Testing the Flexor Digitorum Profundus (FDP):
The FDP is the sole flexor of the distal interphalangeal (DIP) joint. To test its integrity, the examiner must neutralize the FDS by stabilizing the proximal interphalangeal (PIP) joint in extension. If the patient can actively flex the DIP joint, the FDP is intact.
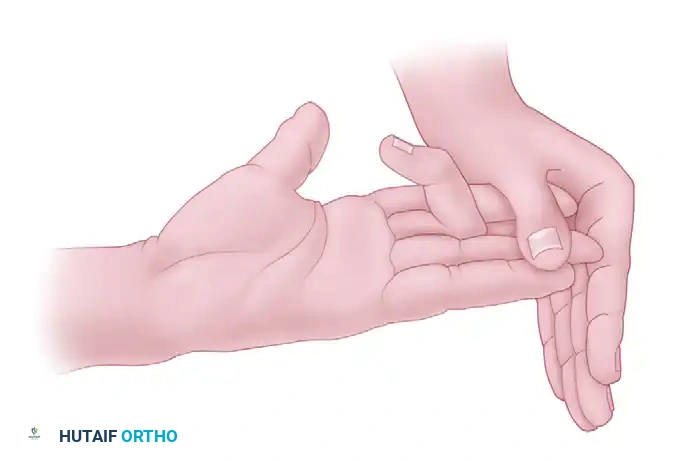
Testing the Flexor Digitorum Superficialis (FDS):
The FDS flexes the PIP joint. Because the FDP muscle bellies share a common origin and act en masse (especially to the middle, ring, and small fingers), the FDP must be neutralized to isolate the FDS. The examiner holds all adjacent, uninjured fingers in strict hyperextension. This tethers the common FDP muscle belly. The patient is then asked to flex the injured finger. If the PIP joint flexes, the FDS is intact.
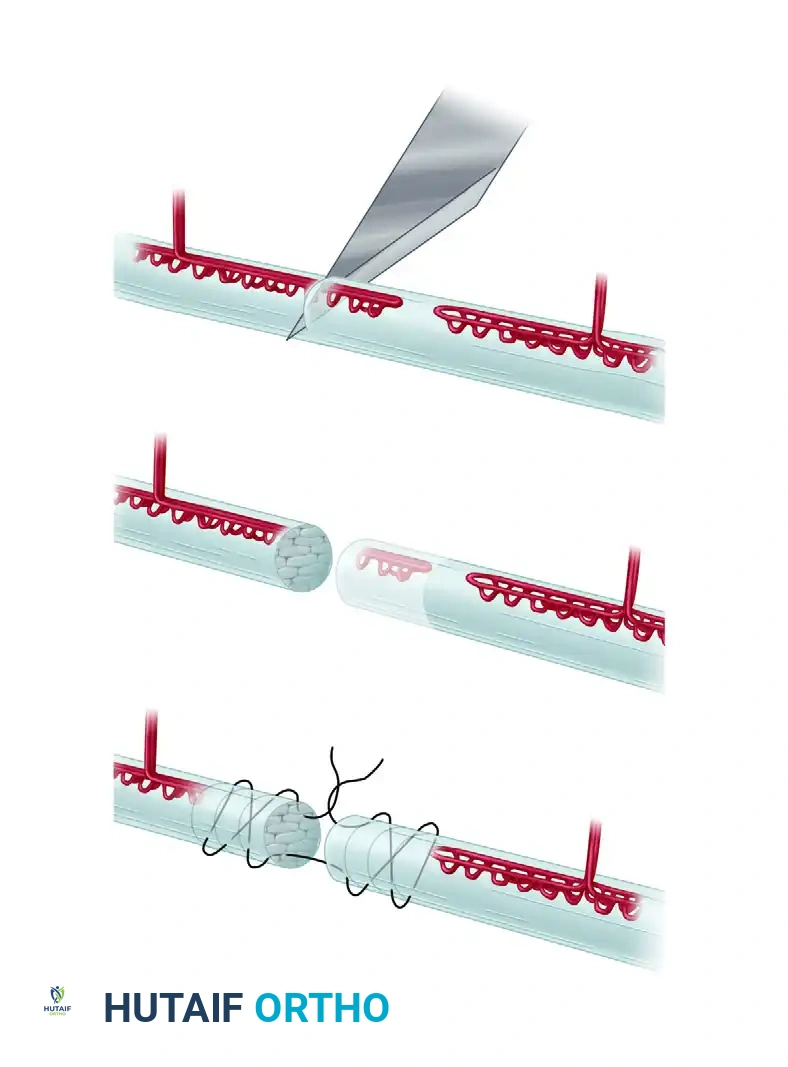
BIOMECHANICS AND PRINCIPLES OF TENDON REPAIR
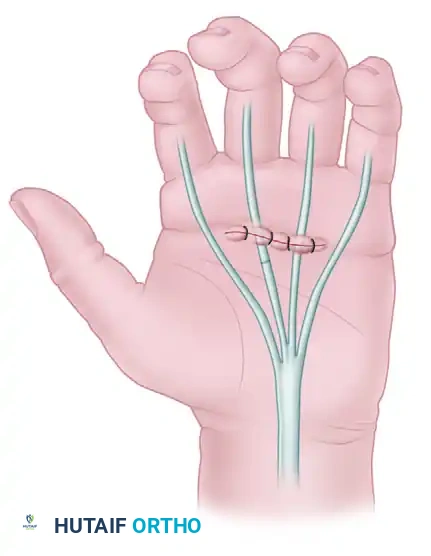
The fundamental purpose of a tendon suture is to precisely approximate the tendon ends—or fasten a tendon to bone—and maintain this apposition against physiological loads during the critical phases of healing.
Strickland’s Six Characteristics of an Ideal Tendon Repair
Handling of the tendon must be exceptionally gentle. Pinching or crushing the epitenon with forceps causes localized necrosis and robust adhesion formation, severely compromising glide. Strickland defined the gold standard for tendon repair through six essential characteristics:
- Easy placement of sutures in the tendon.
- Secure suture knots that resist unraveling under cyclic loading.
- Smooth juncture of tendon ends to allow unhindered gliding within the flexor sheath.
- Minimal gapping at the repair site (gaps >1.5 mm significantly increase rupture risk and adhesion formation).
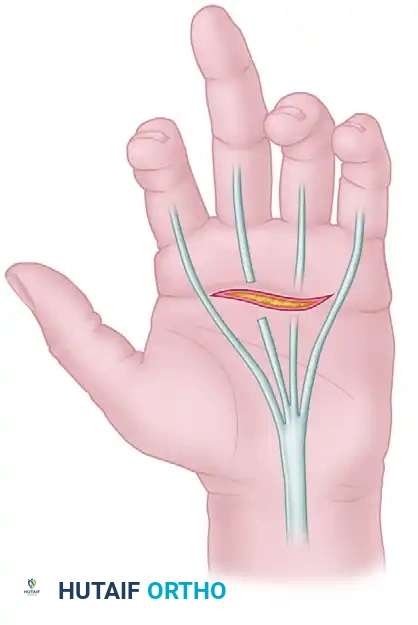
- Minimal interference with tendon vascularity (preserving the intrinsic blood supply).
- Sufficient strength throughout the healing phase to permit the application of early active motion (EAM) stress.
Extensive biomechanical studies confirm that a four-strand core suture combined with an epitendinous repair best accomplishes these objectives, providing the necessary tensile strength for modern rehabilitation protocols.
The Healing Curve and Repair Strength
No suture material or technique can maintain a tendon repair against unlimited active movement in the early postoperative period. The biomechanical strength of a repaired tendon drops precipitously during the first 10 days as the inflammatory phase peaks and collagen softens.
Surgical Warning: The repair is at its weakest between days 5 and 10. Thereafter, fibroplasia and collagen cross-linking gradually increase the tensile strength. By 10 to 12 weeks, the repair can withstand considerable active forces.
SUTURE MATERIALS IN TENDON SURGERY
The selection of suture material is a critical determinant of repair success. The ideal suture must possess high tensile strength, minimal tissue reactivity, excellent handling characteristics, and resistance to elongation.
Core Suture Selection
- Stainless Steel: Historically, monofilament stainless steel offered the highest tensile strength. However, it is notoriously difficult to handle, tends to "cheese-wire" through the tendon substance, and leaves a bulky, prominent knot. Its use is largely restricted to the distal forearm.
- Absorbable Sutures: Catgut and polyglycolic acid derivatives (Dexon, Vicryl) undergo rapid hydrolysis and lose tensile strength far too early to be effective in primary flexor tendon repair.
- Synthetic Non-Absorbables: Nylon and caprolactam (Supramid) maintain resistance to disrupting forces longer than polypropylene (Prolene). Polydioxanone (PDS), a slowly absorbing monofilament, has demonstrated strength comparable to polypropylene. Studies comparing polyglycolide-trimethylene carbonate (Maxon) to PDS found that PDS maintained superior strength over a 28-day period.
- Braided Synthetics (The Clinical Standard): Biomechanical studies indicate that braided polyethylene and braided polyester (Ticron, Fiberwire, Mersilene) offer the best combination of mechanical strength, resistance to gap formation, and knot security. Monofilament nylon, by contrast, permits earlier gap formation under cyclic loading.
Suture Sizing:
Caliber matters significantly. A 4-0 suture is approximately 66% stronger than a 5-0 suture, and a 3-0 suture is 52% stronger than a 4-0 suture.
* 3-0 Suture: Recommended for two- or four-strand configurations in the forearm, palm, and larger digits, yielding a twofold to threefold increase in fatigue strength.
* 4-0 Suture: Preferred in smaller digits where a 3-0 knot would be too bulky for the flexor sheath.
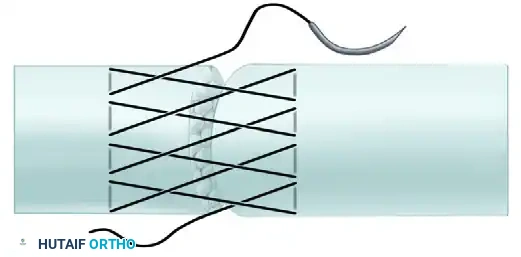
Epitendinous Suture Selection
Epitendinous repairs are typically performed with a 5-0 or 6-0 monofilament suture (e.g., Prolene or Nylon) to minimize drag and tissue reaction.
Emerging Technologies
Recent innovations aim to bypass the limitations of traditional knots:
* Teno Fix: An intratendinous, crimped, single-strand multifilament stainless steel device. In multicenter randomized trials, it demonstrated a 0% rupture rate compared to 18% in four-strand cruciate controls, with excellent DASH scores.
* Barbed Sutures: Knotless barbed sutures have shown equivalent strength to four-strand configurations for epitendinous repair, reducing operative time and knot bulk.
* Laser Welding: Experimental use of neodymium:yttrium-aluminum-garnet (Nd:YAG) lasers has not proven effective for structural tendon welding in current models.
SURGICAL TECHNIQUES AND SUTURE CONFIGURATIONS
The quest for the strongest intratendinous suture arrangement has led to the development of numerous configurations.
Classification of Tendon Anastomoses
Tendon repairs are broadly categorized into three biomechanical groups:
-
Group 1 (Simple Sutures): The suture pull is parallel to the tendon collagen bundles. This transmits stress directly to the opposing tendon ends, resulting in a weak repair prone to pull-out. Interrupted sutures fall here and are unsuitable for primary flexor repair.
-
Group 2 (Grasping Sutures): Exemplified by the Bunnell suture. The longitudinal pull is converted into oblique or transverse compressive forces. The strength of the repair approaches the ultimate tensile strength of the suture material itself.
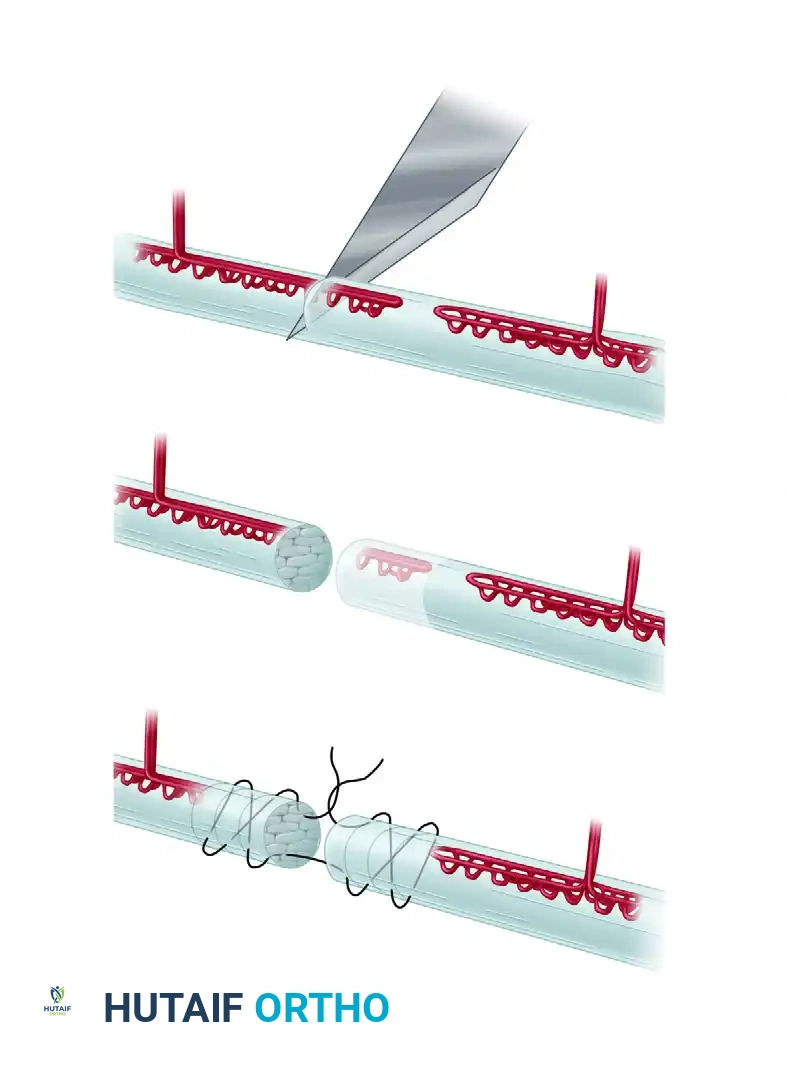
- Group 3 (Weave Repairs): Exemplified by the Pulvertaft fish-mouth weave. Sutures are placed perpendicular to the collagen bundles. This is the strongest union, ideal for tendon grafts and transfers in the forearm, but too bulky for the digital flexor sheath.
Core Suture Techniques
Research unequivocally demonstrates that increasing the number of core strands crossing the repair site (four-strand, six-strand, eight-strand) proportionally increases repair strength, reduces gap formation, and safely permits early active motion.
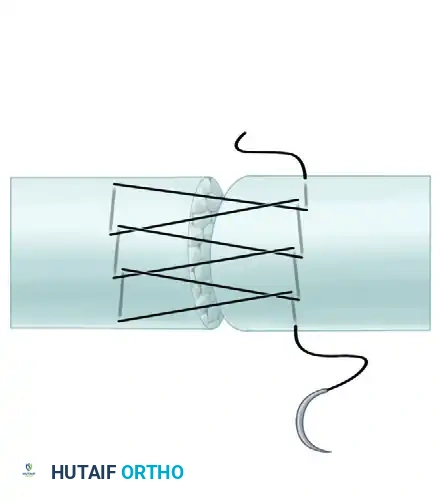
The Bunnell Crisscross:
The classic end-to-end technique. While it provides excellent grasp, it is largely obsolete for primary digital repair because the intratendinous crisscrossing severely jeopardizes the intrinsic microcirculation of the tendon.
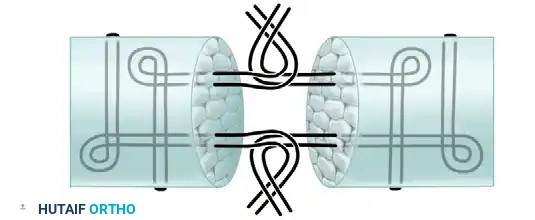
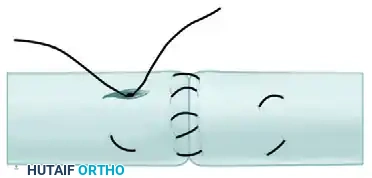
Kessler and Modified Kessler:
The Kessler grasping stitch and its modifications (e.g., Tajima) utilize locking loops that trap bundles of tendon fibers. This prevents the suture from pulling out and significantly increases resistance to gap formation.
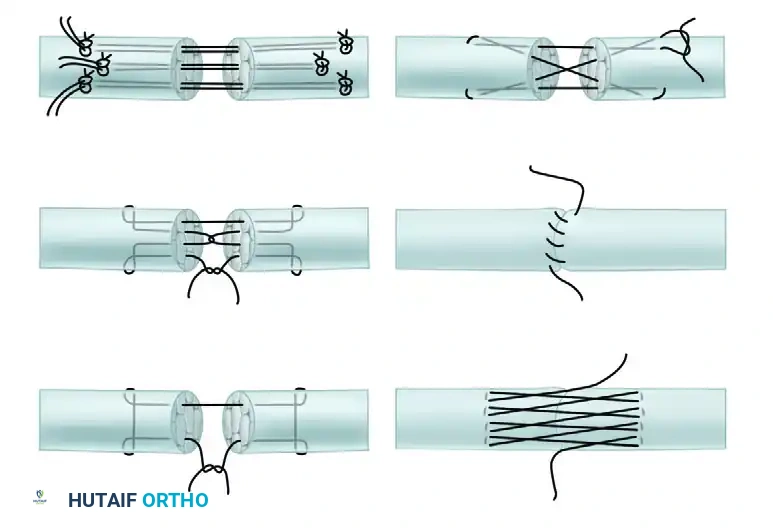
Multi-Strand Modifications:
To support early active motion, surgeons have adapted the Kessler into four-strand and six-strand variants.
* Savage Technique: A robust six-strand modification.
* Lee Technique: A four-strand configuration with two knots buried within the repair site.
* Cruciate and Tang Repairs: The four-strand cruciate technique provides superior resistance to gap formation and higher ultimate tensile strength compared to standard Kessler or Strickland techniques.
Surgical Pearl: Suture placement matters. Experimental data reveals that the mean strength of repairs sutured in the dorsal half of the tendon is 58.3% greater than those placed in the volar half. Furthermore, placing peripheral sutures 2 mm from the repair site provides a stronger construct than a 1 mm purchase.
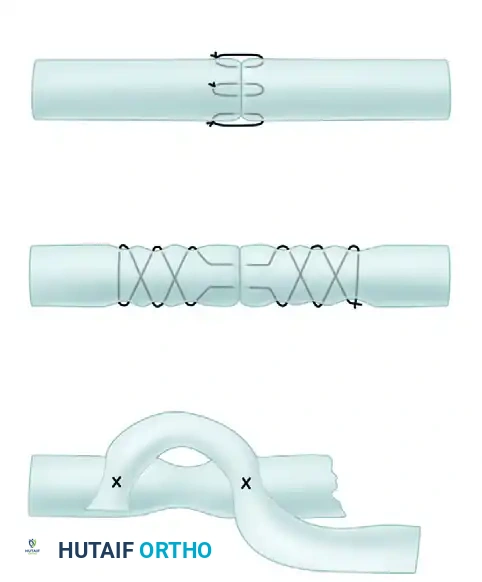
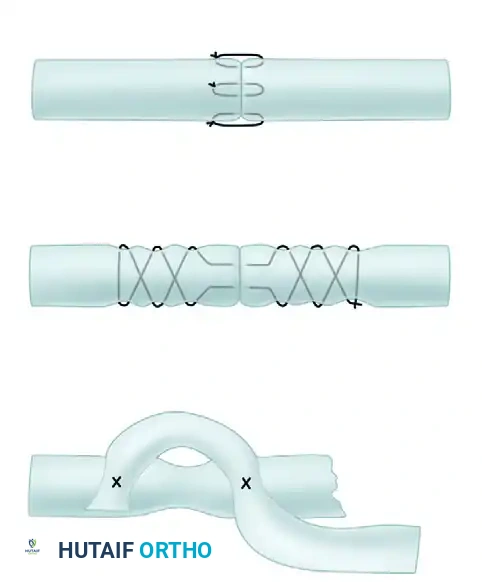
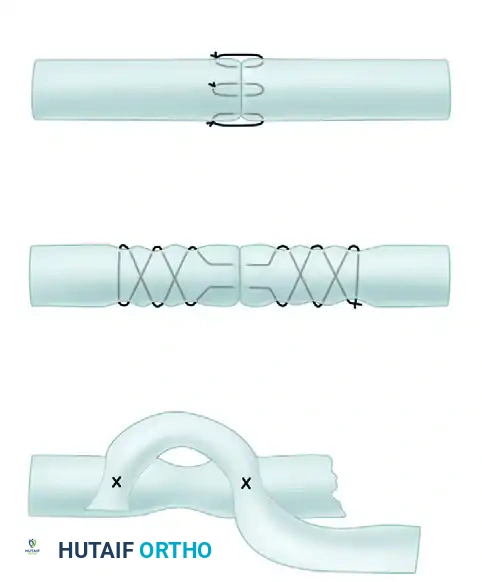
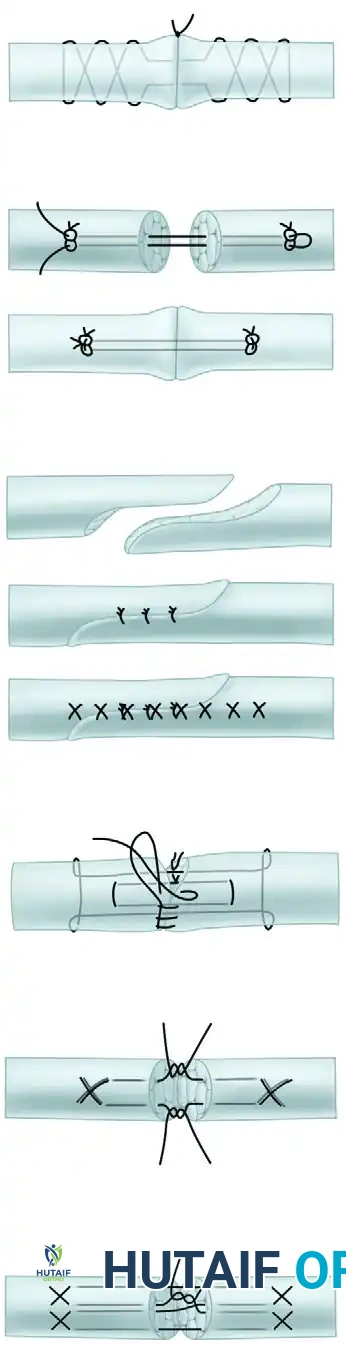
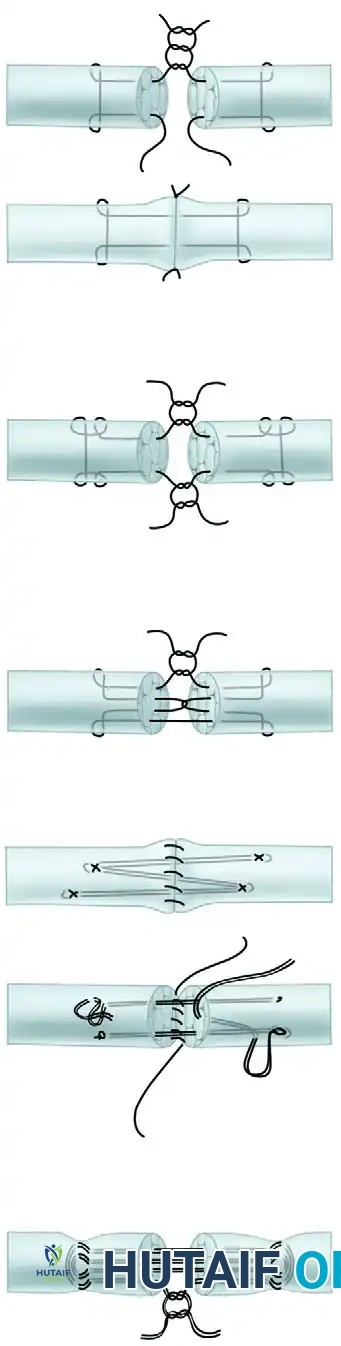
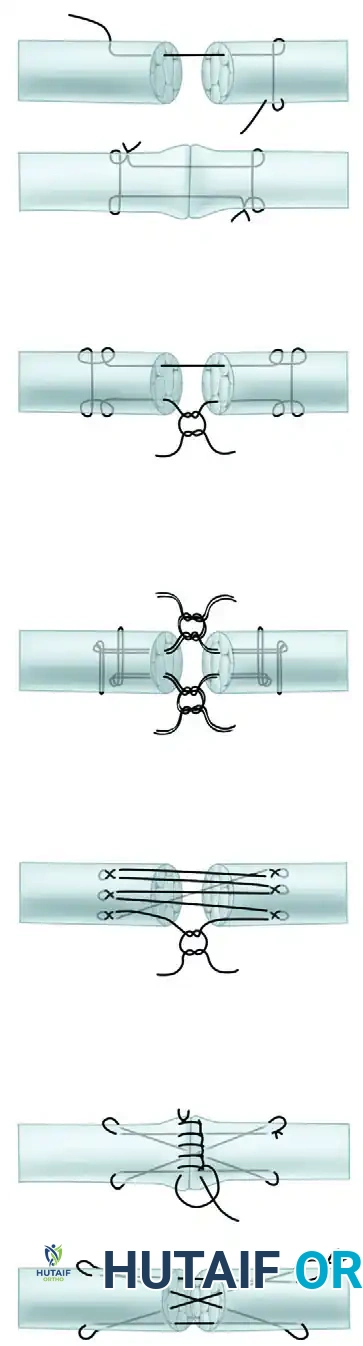
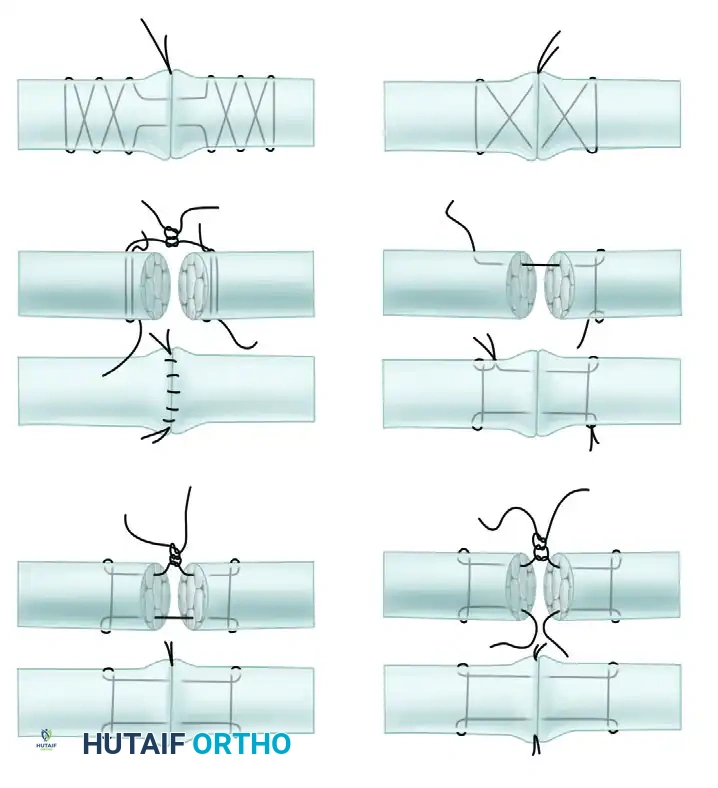
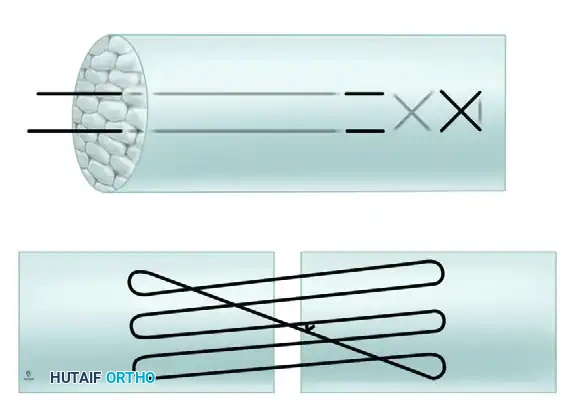
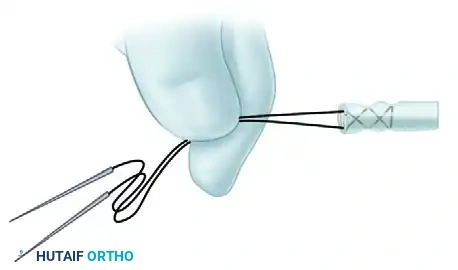
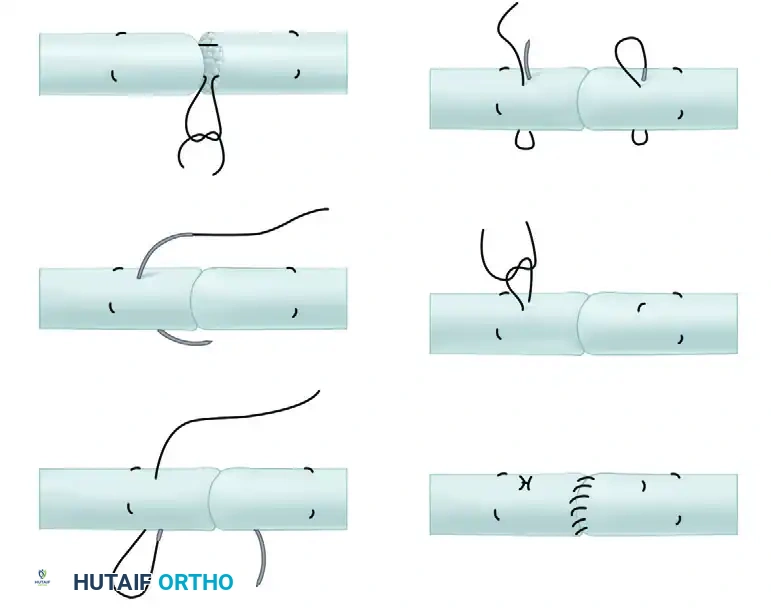
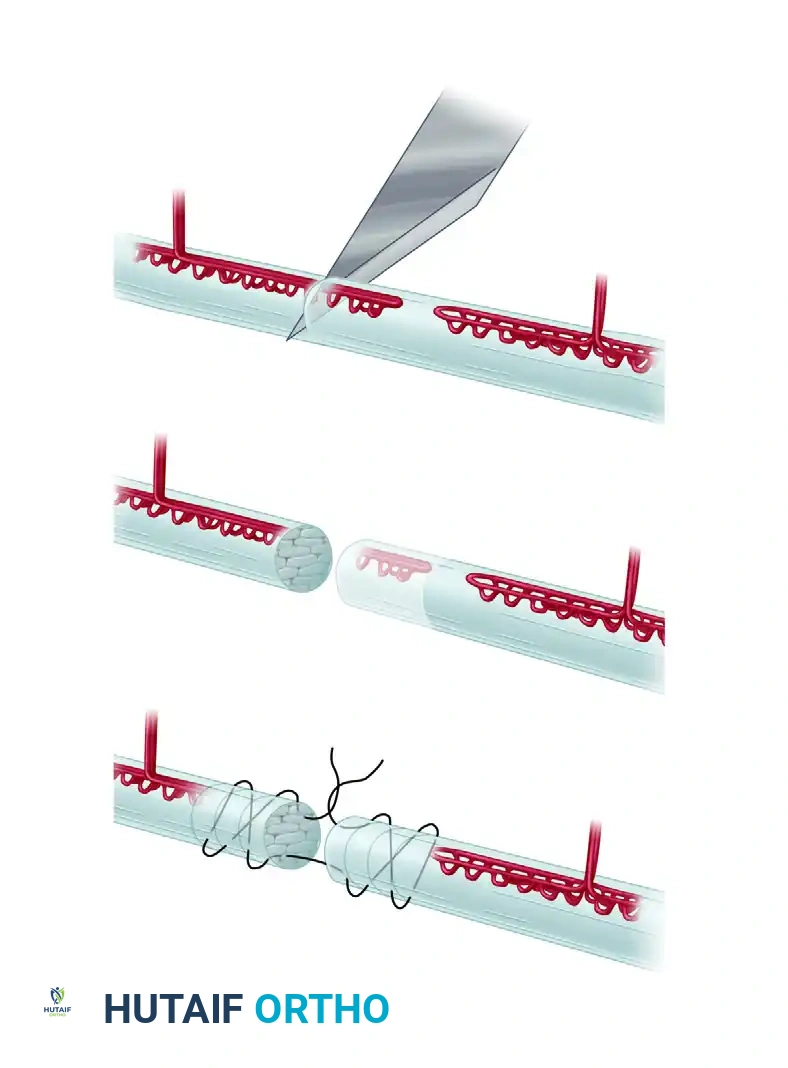
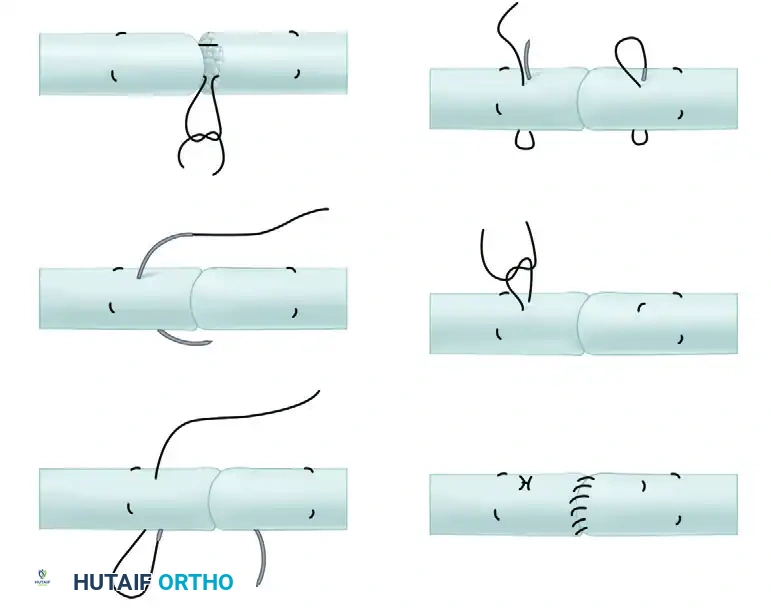
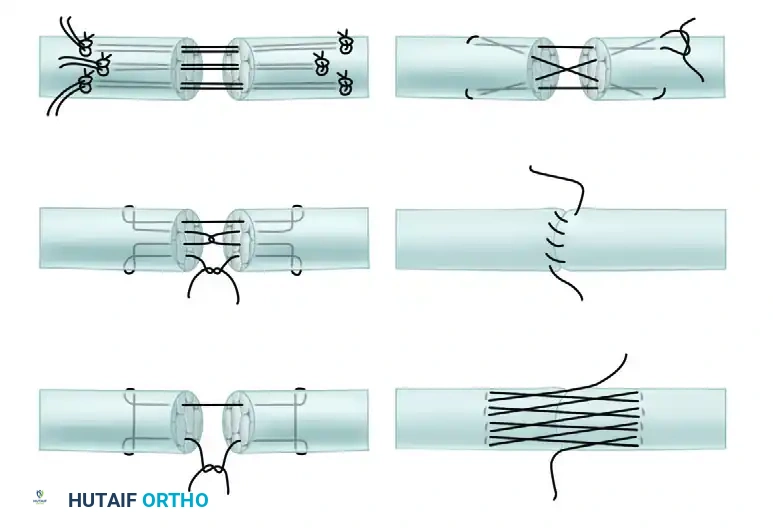
Visual Atlas of Advanced Core and Epitendinous Configurations
The following diagrams illustrate the evolution and biomechanical diversity of modern tendon repair strategies, highlighting locking mechanisms, cross-stitches, and multi-strand distributions designed to optimize the strength-to-bulk ratio.









You Might Also Like

