Operative Management of Trigger Finger & De Quervain Disease
Key Takeaway
Stenosing tenosynovitis, encompassing trigger finger and de Quervain disease, requires precise surgical intervention when conservative measures fail. This guide details the step-by-step operative techniques for A1 pulley release, percutaneous methods, and first dorsal compartment reconstruction. Mastery of these procedures demands a thorough understanding of hand biomechanics, neurovascular anatomy, and meticulous surgical execution to restore optimal tendon glide and prevent recurrence.
INTRODUCTION TO STENOSING TENOSYNOVITIS
Stenosing tenosynovitis is a pervasive orthopaedic pathology characterized by a size mismatch between a swollen, inflamed tendon (or its synovial sheath) and the rigid fibro-osseous tunnel through which it glides. In the hand and wrist, this phenomenon most frequently manifests as Trigger Finger (involving the A1 pulley of the flexor tendon sheath) and de Quervain Disease (involving the first dorsal extensor compartment).
When conservative modalities—such as corticosteroid injections, splinting, and nonsteroidal anti-inflammatory drugs (NSAIDs)—fail to provide durable relief, surgical intervention becomes the gold standard. This comprehensive masterclass details the evidence-based surgical techniques, biomechanical considerations, and advanced reconstructive options for both conditions, tailored for the practicing orthopaedic surgeon and hand specialist.
PART I: SURGICAL RELEASE OF TRIGGER FINGER
Trigger digit (stenosing tenosynovitis of the flexor sheath) is caused by pathological thickening of the first annular (A1) pulley and the formation of a reactive nodule (Notta nodule) within the flexor tendon. The primary surgical objective is the complete longitudinal division of the A1 pulley to restore unimpeded tendon excursion while meticulously preserving the adjacent A2 pulley to prevent tendon bowstringing.
Indications for Surgery
- Failure of conservative management (typically after 1–2 corticosteroid injections).
- Locked digit (irreducible triggering) presenting acutely or chronically.
- Severe triggering in diabetic patients, who statistically exhibit lower success rates with corticosteroid injections.
- Pediatric trigger thumb (often requiring surgical release if unresolved by age 2-3).
Clinical Anatomy & Biomechanics
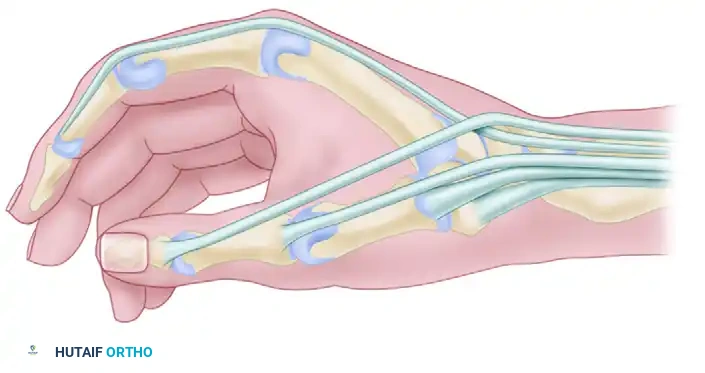
The flexor tendon pulley system consists of five annular (A1-A5) and three cruciate (C1-C3) pulleys.
* The A1 Pulley: Arises from the palmar plate of the metacarpophalangeal (MCP) joint and the base of the proximal phalanx. It is the primary site of impingement.
* The A2 Pulley: Located over the proximal phalanx, this is a critical biomechanical structure. Iatrogenic injury to the A2 pulley results in flexor tendon bowstringing, leading to a profound loss of mechanical advantage and active flexion deficit.
* Neurovascular Bundles: The digital nerves run volar and parallel to the flexor sheath. The radial digital nerve of the thumb is particularly vulnerable as it courses obliquely across the flexor sheath near the MCP flexion crease.
🚨 SURGICAL WARNING: Avoid the digital nerves, which on the thumb are more palmar and closer to the flexor sheath than might be anticipated. The thumb radial digital nerve is especially vulnerable during both open and percutaneous approaches.
Open Surgical Technique (Technique 76-6)
1. Anesthesia and Positioning
The procedure is typically performed under local anesthesia, often utilizing the Wide-Awake Local Anesthesia No Tourniquet (WALANT) technique. Local anesthetic infiltration (e.g., 1% lidocaine with 1:100,000 epinephrine) in the palm proximal to the incision site is preferred.
If a tourniquet is desired, a pneumatic arm tourniquet may be helpful, although a high forearm Esmarch wrap is usually sufficient for hemostasis.
2. Incision Planning
Precise incision placement is critical for adequate exposure and prevention of scar contracture.
* Middle, Ring, and Small Fingers: Make a transverse incision about 2 cm long, several millimeters distal to the distal palmar crease.
* Index Finger: Make a transverse incision several millimeters distal to the proximal palmar crease.
* Thumb: Alternative incisions can be made obliquely or longitudinally between the MCP and distal palmar creases, or obliquely across the thumb MCP flexion crease.
Figure: Standard transverse incision markings for open surgical treatment of trigger finger.
3. Dissection and Exposure
- Incise the skin and carefully dissect through the subcutaneous fat using blunt spreading with tenotomy scissors.
- Retract the neurovascular bundles laterally.
- Identify with a small probe the discrete proximal edge of the first annular (A1) pulley of the flexor sheath. Clear the overlying fascia to visualize the transverse fibers of the pulley.
4. Pulley Release
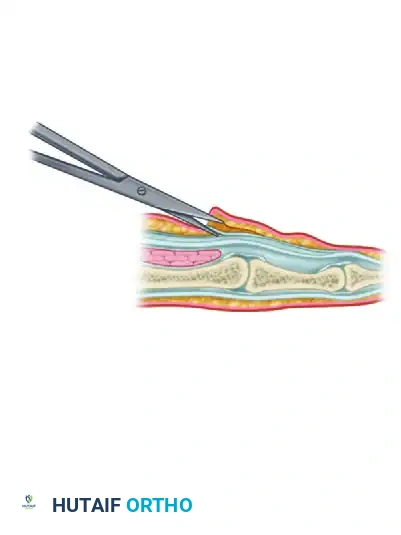
- Place a small knife blade or one blade of a pair of slightly opened blunt scissors just under the proximal edge of the sheath.
- Gently push it distally, cutting the first annular pulley in the midline.
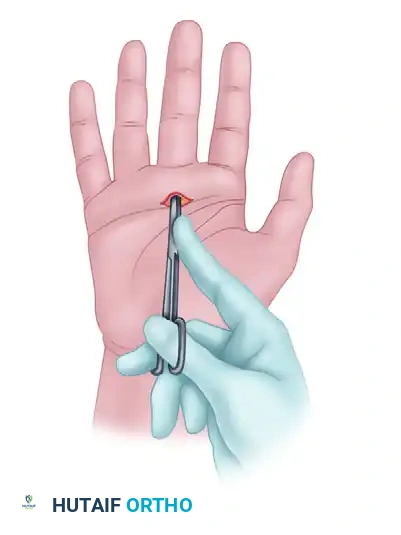
Figure: One blade of scissors has been placed beneath the proximal edge of the tendon sheath, opening the flexor sheath from proximal to distal.
- Incise the sheath from proximal to distal, approximately 1 cm.
- Crucial Step: Reassess for triggering. Ask the awake patient to actively flex and extend the digit fully. Ensure smooth gliding of the tendon without catching.
💡 CLINICAL PEARL: Avoid cutting too far distally. In the fingers, extending the release too far risks disrupting the A2 pulley. In the thumb, overzealous distal release risks disrupting the oblique pulley, which is essential for thumb kinematics.
Percutaneous Release Technique
Percutaneous release is a minimally invasive alternative, primarily indicated for the middle and ring fingers. It is generally contraindicated in the thumb and index finger due to the proximity of the digital nerves to the midline.
Technique Steps
- Hyperextend the metacarpophalangeal joint to stretch the A1 pulley and displace the neurovascular bundles dorsally.
- Insert a 19-gauge needle just distal to the flexor crease. The bevel of the needle must be oriented longitudinally, parallel with the tendon fibers.

Figure: Initial percutaneous needle insertion.
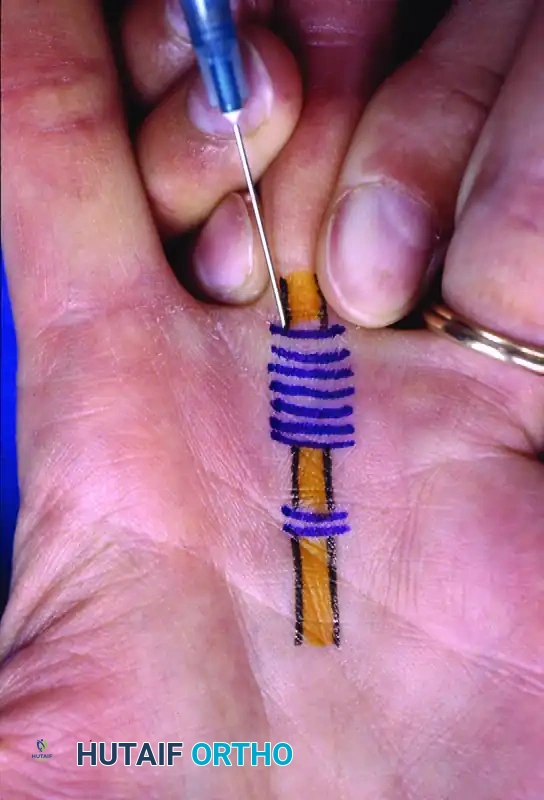
Figure: Percutaneous release of long finger A1 pulley. Metacarpophalangeal joint hyperextended and 19-gauge needle inserted just distal to the flexor crease. Skin markings indicate the path of flexor tendons.
- Stabilize the needle and use the sharp bevel to sweep and release the pulley from proximal to distal.
- A distinct loss of grating sensation as the pulley is cut indicates the completion of the release.

Figure: Needle stabilized and pulley released from proximal to distal.
PART II: SURGICAL MANAGEMENT OF DE QUERVAIN DISEASE
De Quervain tenosynovitis involves the entrapment of the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons within the first dorsal extensor compartment of the wrist.
Anatomical Pitfalls
The most common cause of surgical failure in de Quervain disease is the failure to recognize and release a separate subcompartment housing the EPB tendon.
* The APL typically has multiple tendon slips (often 2 to 4).
* The EPB is usually a single slip.
* An intracompartmental septum separates the APL and EPB in up to 60% of patients.

Figure: Cross-sectional anatomy demonstrating the first dorsal compartment. Note the distinct septation separating the APL and EPB tendons, a frequent site of missed pathology.
Primary Release and Compartment Reconstruction (Littler, Freedman, and Malerich Technique)
Simple division of the retinaculum can sometimes lead to volar subluxation of the tendons upon wrist flexion. To prevent this, reconstruction of the first extensor compartment is highly recommended.
1. Incision and Nerve Protection
- Make a transverse incision at the level of the margin of the first extensor compartment, in line with the extensor creases.
- Meticulously identify and protect the superficial branch of the radial nerve (SBRN). Neuroma of the SBRN is a devastating complication that can cause severe, chronic pain.
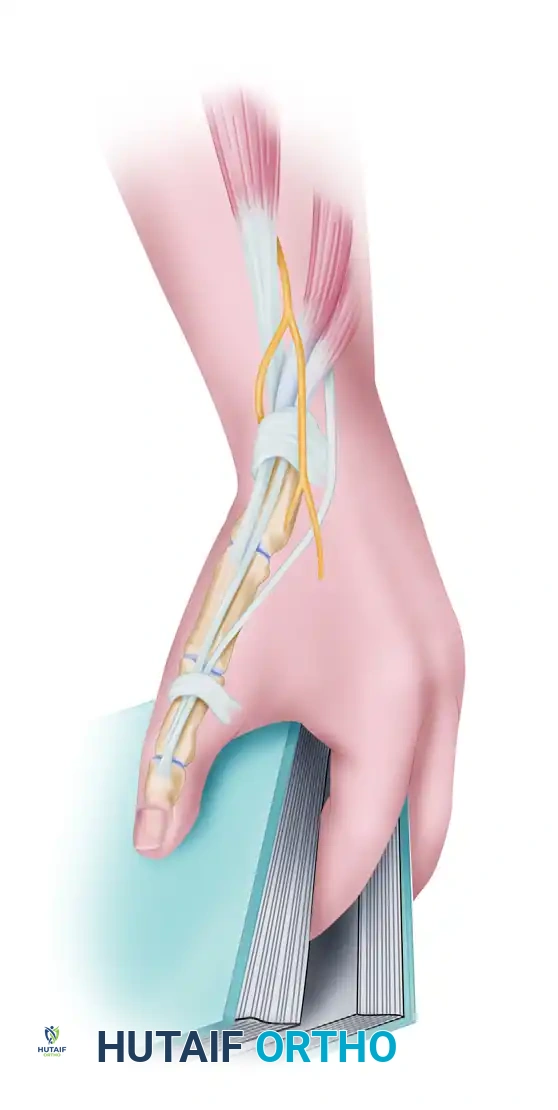
Figure: Transverse incision at the level of the first extensor compartment. The superficial radial nerve is identified and rigorously protected.
2. Retinacular Incision and Exploration
- Incise the retinacular sheath along its dorsoulnar margin. This specific placement leaves a volar flap of retinaculum to prevent anterior tendon subluxation.
- Explore the sheath and definitively identify both the APL (multiple slips) and the EPB tendon.

Figure: The retinacular sheath is incised. The Extensor pollicis brevis (b) is retracted from the first dorsal compartment. Note the abductor pollicis longus (a).
3. Septum Excision
- If an intracompartmental septum is present, it must be completely excised to ensure full decompression of the EPB.

Figure: Excision of the intracompartmental septum separating the APL and EPB tendons.
4. Retinacular Repair
- To prevent tendon subluxation while maintaining decompression, the retinacular sheath is repaired over the abductor pollicis longus tendon using 5-0 absorbable sutures, effectively creating a widened, reconstructed compartment.

Figure: The retinacular sheath is repaired over the abductor pollicis longus tendon with 5-0 absorbable sutures. The wrist is subsequently immobilized in a splint for 2 weeks.
Management of Recurrent De Quervain Disease (Wilson et al. Technique)
In cases of severe recurrence, extensive scarring, or iatrogenic tendon subluxation from previous over-release, a vascularized fascial flap may be required to provide a smooth gliding surface and reconstruct the pulley.
Distally Based Radial Forearm Fascia-Fat Flap
This advanced technique utilizes a local fasciosubcutaneous flap based on the radial artery perforators.
- Flap Harvest: A radial fasciosubcutaneous flap (approximately 4 cm x 12 cm) is harvested from the volar forearm. The superficial branch of the radial nerve and the lateral antebrachial cutaneous nerve are retracted and protected. The flap is turned over 180 degrees distally.

Figure: The distally based radial forearm fascia-fat flap is harvested, protecting the radial artery and local cutaneous nerves.
- Tendon Wrapping: The vascularized fascial flap is wrapped around the scarred APL and EPB tendons to provide a healthy, vascularized gliding bed.
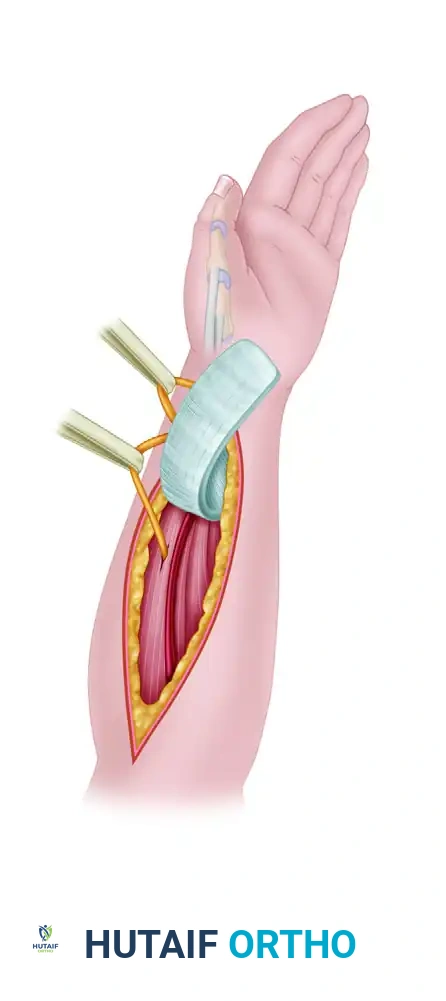
Figure: The fascial flap is wrapped around the APL and EPB tendons.
- Tube Construction: A vascularized fascial tube is created and anchored distally with tacking sutures to reconstruct the extensor retinaculum and prevent subluxation.

Figure: Fascial tube construction is completed, anchoring the flap distally with tacking sutures to restore biomechanical stability.
POSTOPERATIVE PROTOCOL & COMPLICATION MANAGEMENT
Rehabilitation
- Trigger Finger: Immediate active range of motion (AROM) of the digits is encouraged on postoperative day 1 to prevent flexor tendon adhesions. Heavy lifting and forceful gripping are restricted for 3–4 weeks.
- De Quervain Disease: Following primary release or reconstruction, the wrist and thumb are typically immobilized in a thumb spica splint for 1 to 2 weeks to allow the retinacular repair to heal, followed by progressive AROM and strengthening.
Complications
- Nerve Injury: The most severe complication. Injury to the radial digital nerve of the thumb (in trigger release) or the superficial radial nerve (in de Quervain release) can lead to debilitating neuromas. Meticulous blunt dissection and retraction are mandatory.
- Incomplete Release: Results in persistent triggering or pain. In de Quervain's, this is almost exclusively due to a missed EPB subcompartment.
- Tendon Bowstringing: Caused by iatrogenic division of the A2 pulley (fingers), oblique pulley (thumb), or excessive release of the extensor retinaculum without reconstruction.
- Infection and Stiffness: Mitigated by strict sterile technique, appropriate prophylactic antibiotics (if indicated), and early, aggressive hand therapy.
💡 CLINICAL PEARL: The success of stenosing tenosynovitis surgery lies not just in the release of the constriction, but in the meticulous preservation of the surrounding biomechanical stabilizers and neurovascular structures. Always verify full, unimpeded tendon excursion intraoperatively before skin closure.
You Might Also Like