A1 Pulley Release & Flexor Digitorum Superficialis Slip Excision: An Intraoperative Masterclass

Key Takeaway
Welcome, fellows, to an immersive masterclass on A1 pulley release for trigger finger. We'll meticulously cover comprehensive anatomy, precise patient positioning, and step-by-step intraoperative execution. Learn to identify and release the A1 pulley, protect neurovascular structures, perform tenosynovectomy or FDS slip excision when indicated, and manage potential pitfalls, ensuring optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, to the operating theater. Today, we are addressing a ubiquitous yet frequently debilitating condition encountered in hand surgery: trigger finger, formally known as stenosing tenosynovitis. This pathology represents a biomechanical entrapment of the digital flexor tendon—or tendons—by the flexor tendon sheath, culminating in a critical size mismatch between the gliding tendon and its constraining pulley system. Over time, this repetitive mechanical irritation induces profound histological changes. The A1 pulley undergoes fibrocartilaginous metaplasia, characterized by an accumulation of hyaluronic acid and chondroid cells, leading to gross hypertrophy. Simultaneously, the underlying tendon develops reactive swelling, often forming a palpable mass known as the Nodule of Notta.
This pathophysiological cascade creates a vicious cycle. The initial entrapment causes localized pulley hypertrophy, and this resultant thickening exponentially exacerbates the entrapment. Clinically, this manifests as a spectrum of tenosynovial inflammation, localized volar pain, mechanical catching, locking, and a progressive, debilitating reduction in active range of motion (ROM). The fundamental issue lies in the high angular loads exerted at the A1 pulley during power grip, often compounded by systemic causes of local inflammation, rendering the inner diameter of the flexor tendon sheath insufficient to accommodate the excursion of the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons.
Trigger digits frequently develop spontaneously, though they are highly correlated with periods of unaccustomed heavy hand use, repetitive microtrauma, or specific systemic diatheses. The epidemiological profile reveals a marked predilection for females in their fifth and sixth decades of life. Furthermore, patients with endocrine and metabolic disorders—most notably diabetes mellitus, rheumatoid arthritis, hypothyroidism, and amyloidosis—exhibit a significantly higher incidence, multi-digit involvement, and a higher propensity for recalcitrant disease that fails conservative management.
While some mild, transient cases may resolve spontaneously or with behavioral modification, a substantial majority persist. These cases inexorably advance to passively correctable locking, or worse, become indefinitely locked in flexion or extension. When a digit becomes rigidly locked, the risk of secondary proximal interphalangeal (PIP) joint flexion contracture increases dramatically, necessitating prompt and definitive surgical intervention to restore the intricate biomechanics of the hand.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches the skin, an exhaustive, three-dimensional understanding of the intricate anatomy of the flexor tendon system and its intimately associated neurovascular structures is paramount. The surgical release of the A1 pulley is an exercise in precise anatomical navigation.
The Flexor Tendon Pulley System
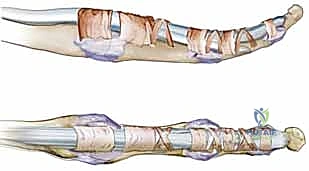
The FDP and FDS tendons (and the flexor pollicis longus, or FPL, in the thumb) course under a highly sophisticated, retinacular flexor sheath. This sheath is composed of a specialized series of annular (A) and cruciate (C) pulleys, strategically positioned to maintain the mechanical advantage of the tendons, optimize their moment arm, and prevent bowstringing across the joints during active digital flexion.
The annular pulleys (A1 through A5) are dense, rigid fibrous bands that are biomechanically crucial for maintaining the tendon's close proximity to the phalangeal bones.
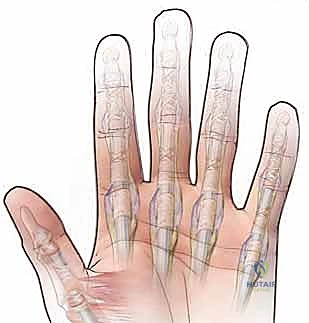
* A1 Pulley: This is our primary surgical target. Located volar to the metacarpophalangeal (MCP) joint, it arises from the palmar plate and the base of the proximal phalanx. It is almost universally the primary site of entrapment in idiopathic trigger finger.
* A2 Pulley: Located at the volar aspect of the proximal half of the proximal phalanx. It is the longest and biomechanically most critical pulley. Its integrity must be absolutely preserved during an A1 release to prevent debilitating flexor tendon bowstringing.
* A3 Pulley: A narrow band located over the PIP joint palmar plate.
* A4 Pulley: Located over the mid-portion of the middle phalanx. Like the A2 pulley, it is a major mechanical constraint and must be protected.
* A5 Pulley: A thin band located over the DIP joint palmar plate.
The cruciate pulleys (C1, C2, and C3) are thinner, highly flexible, cross-hatched bands located intervening between the rigid annular pulleys. They collapse during digital flexion, allowing the annular pulleys to approximate without restricting tendon excursion.
In the thumb, the retinacular system is distinct, comprising the A1 pulley at the MCP joint, a broad Oblique pulley coursing diagonally over the proximal phalanx, and the A2 pulley at the interphalangeal (IP) joint. The Oblique pulley in the thumb is functionally analogous to the A2 pulley in the triphalangeal digits; its inadvertent release will lead to FPL bowstringing and severe loss of terminal pinch strength.
Neurovascular Structures: Our Constant Companions
The proper digital arteries and nerves run immediately adjacent to the flexor tendon sheath, particularly at the level of the A1 pulley where they are relatively superficial. These structures are exquisitely vulnerable during our surgical approach and must be meticulously identified, protected, and gently retracted.
The digital nerves typically run volar to the digital arteries, making them the most superficial and vulnerable structures encountered after traversing the subcutaneous fat. They provide critical tactile sensation to the digits. Iatrogenic injury can lead to permanent numbness, debilitating dysesthesia, or the formation of exquisitely painful neuromas. The digital arteries run slightly deeper and more dorsally. While the hand has a robust collateral blood supply, arterial injury can compromise digital perfusion, particularly in vasculopathic patients.
Specifically for the Thumb: The radial digital nerve of the thumb is at the absolute greatest risk during an A1 pulley release. Due to the pronation of the thumb, the radial digital nerve frequently courses obliquely across the surgical field, directly overlying or immediately adjacent to the radial border of the A1 pulley. This anatomical quirk demands heightened vigilance and meticulous blunt dissection. Similarly, the ulnar digital nerve of the small finger is at elevated risk due to its superficial course near the MCP crease.
Muscular Intervals and Osteology
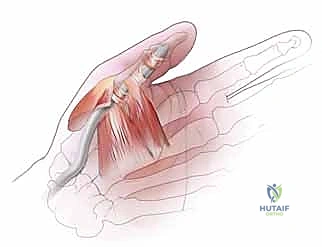
The A1 pulley lies directly volar to the metacarpal head and the base of the proximal phalanx, spanning the volar aspect of the MCP joint. Our incision is planned in the distal palm, directly overlying this pulley system. Because we are operating superficially to access the fibrous flexor sheath, deeper muscular intervals are not directly encountered during a standard A1 release.
However, a profound understanding of the superficial palmar anatomy is essential. The palmar aponeurosis sends pretendinous bands that insert distally into the skin and the flexor sheath. These bands must be longitudinally split to access the A1 pulley. Furthermore, awareness of the underlying intrinsic muscles—the lumbricals originating from the FDP tendons, and the interossei flanking the metacarpals—helps the surgeon appreciate the depth and boundaries of the dissection, ensuring instruments remain safely within the central compartment of the digit.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for stenosing tenosynovitis is predicated on a careful clinical evaluation, the duration of symptoms, and the patient's response to conservative modalities. Clinical presentation is often categorized using Green's classification of trigger digits, ranging from pre-triggering pain (Grade I) to a rigidly locked digit with secondary joint contracture (Grade IV).
While non-operative management—including activity modification, rigid extension splinting, and corticosteroid injections—is the first-line treatment for Grades I through III, surgical release becomes the definitive solution when these measures fail or are anatomically contraindicated.
| Category | Specific Criteria |
|---|---|
| Primary Indications | - Persistent symptoms (pain, catching, locking) failing 1-2 corticosteroid injections. - Grade IV Trigger Digit (locked in flexion or extension with passive uncorrectability). - Severe pain severely limiting activities of daily living (ADLs). - Trigger digits in pediatric patients (often presenting as locked thumbs), which rarely respond to injections. |
| Relative Indications | - Trigger digits in diabetic patients (historically exhibit a lower success rate and higher recurrence rate with corticosteroid injections). - Multiple concurrent trigger digits. - Concomitant carpal tunnel syndrome requiring surgical release in the same hand. |
| Absolute Contraindications | - Active local skin infection or cellulitis at the planned surgical site. - Medically unstable patient unfit for local or regional anesthesia. |
| Relative Contraindications | - Rheumatoid Arthritis or other inflammatory arthropathies (Isolated A1 release can exacerbate ulnar drift; these patients often require tenosynovectomy and potentially FDS slip excision instead). - Severe, long-standing PIP joint flexion contracture where A1 release alone will not restore functional extension. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning and meticulous patient positioning are the bedrock of a safe, efficient, and successful surgical outcome. The preoperative phase is where potential complications are anticipated and mitigated.
Pre-Operative Assessment and Anesthesia
Before the patient enters the operating theater, I review their clinical notes, noting the specific digits involved, the duration of locking, and the presence of any pre-existing PIP joint contractures. I discuss the planned procedure comprehensively, explicitly including the possibility of a flexor digitorum superficialis (FDS) ulnar slip resection if a simple A1 release proves insufficient to restore smooth gliding. This ensures the patient is fully informed and we have explicit consent for all potential intraoperative interventions.

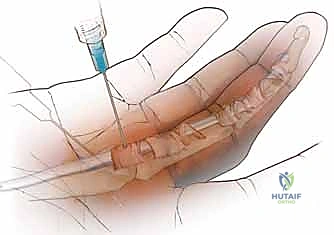
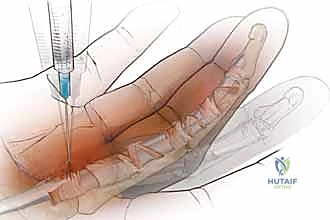
Anesthesia is a critical consideration. While traditional approaches utilized a proximal arm tourniquet with local anesthesia and intravenous sedation, the modern gold standard is the Wide Awake Local Anesthesia No Tourniquet (WALANT) technique. By injecting a mixture of 1% lidocaine with 1:100,000 epinephrine (buffered with sodium bicarbonate to minimize injection pain) directly into the subcutaneous tissues and tendon sheath 30 minutes prior to surgery, we achieve profound local anesthesia and excellent hemostasis without the ischemic pain of a tourniquet. Crucially, WALANT allows the fully awake patient to actively flex and extend their digits intraoperatively. This provides the surgeon with immediate, dynamic confirmation of a complete pulley release and highlights any residual triggering that might necessitate an FDS slip excision.
Patient Positioning and Setup
The patient is positioned supine on the operating table. The affected extremity is abducted onto a specialized, radiolucent hand table, ensuring the palm is facing directly upwards in full supination.
For the index, middle, ring, and small digits, a specialized hand holder (such as a malleable "lead hand") is invaluable. It rigidly stabilizes the hand, retracts the adjacent digits, allows for consistent exposure, and reduces the need for a surgical assistant to manually hold the limb. For thumb procedures, I often prefer to have the surgeon and assistant position the hand manually, or utilize a specialized thumb holder to maintain the thumb in extension and slight abduction, optimizing the exposure of the volar MCP crease.
If the WALANT technique is not utilized, a well-padded pneumatic tourniquet is placed high on the brachium. The arm is exsanguinated with an Esmarch bandage, and the tourniquet is inflated to 250 mmHg just before the incision to create a bloodless field. This is critical for identifying the delicate, translucent neurovascular structures.
Step-by-Step Surgical Approach and Fixation Technique
We are now scrubbed, the patient is prepped and draped in a standard sterile fashion, and our surgical field is optimized. The following steps detail the precise intraoperative execution of an A1 pulley release and, when necessary, an FDS slip excision.
1. Incision Planning and Execution
Our primary objective is to access the A1 pulley with minimal disruption to the surrounding palmar fascia and maximum protection of the neurovascular bundles. The choice of incision depends on the specific digit and surgeon preference.


For the central digits (index, middle, ring), I strongly advocate for a 1.5 cm longitudinal or slightly oblique incision centered directly over the palpable A1 pulley, typically originating just distal to the distal palmar crease. A longitudinal incision offers superior proximal and distal extensibility should the pathology require wider exposure. Alternatively, a transverse incision placed precisely within the distal palmar crease offers excellent cosmesis but limits longitudinal extension. For the thumb, a transverse incision placed exactly in the volar MCP flexion crease provides safe and direct access to the A1 pulley while minimizing scar contracture.
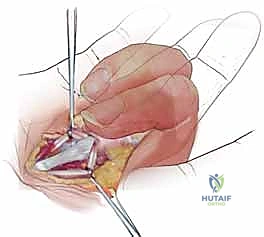
2. Dissection to the Flexor Sheath
Using a #15 blade, the skin is incised. From this point forward, dissection must be strictly blunt and longitudinal to avoid iatrogenic injury. Using delicate tenotomy scissors or a small hemostat, the subcutaneous fat is gently spread parallel to the axis of the digit.
We quickly encounter the longitudinally oriented pretendinous bands of the palmar aponeurosis. These fibers are bluntly split and retracted radially and ulnarly using small Senn or Ragnell retractors. As we retract these bands, we must actively sweep the neurovascular bundles away from the midline. The glistening, transversely oriented fibers of the A1 pulley will now come into direct view.
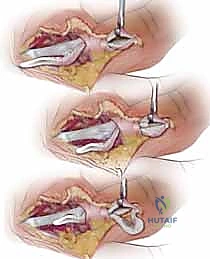
3. The A1 Pulley Release
With the A1 pulley clearly visualized and the neurovascular bundles safely protected behind our retractors, the release is performed.
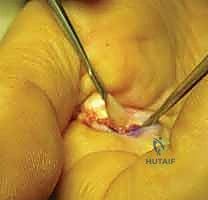
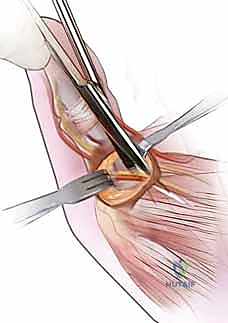

Using a #15 blade or sharp tenotomy scissors, the A1 pulley is incised longitudinally precisely in the midline. You will feel a distinct, gritty resistance as the thickened fibrocartilaginous tissue yields. The release must be carried proximally to the origin of the A1 pulley at the palmar aponeurosis, and distally to its termination.


CRITICAL STEP: The distal extent of the release must be performed under direct, magnified vision. The surgeon must positively identify the proximal edge of the A2 pulley. The A1 release stops exactly where the A2 pulley begins. Inadvertent transection of the A2 pulley is a catastrophic error that will result in immediate and irreversible flexor tendon bowstringing.
Once the release is complete, if the patient is awake under WALANT, they are instructed to actively make a full fist and fully extend the digit. The surgeon observes the tendon gliding smoothly without any catching or locking. If the patient is under general anesthesia, passive traction on the flexor tendons proximal to the wrist can simulate this motion.
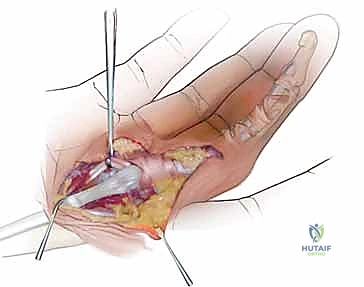
4. Flexor Digitorum Superficialis (FDS) Slip Excision
In approximately 5-10% of cases—particularly in patients with severe, chronic triggering, rheumatoid arthritis, or profound diabetic tenosynovitis—a complete A1 pulley release is insufficient. The patient will continue to exhibit triggering, or the PIP joint will remain stubbornly stiff. This occurs because the FDS tendon itself has become so grossly hypertrophied that it impinges at the level of Camper's chiasm or against the proximal edge of the intact A2 pulley.


In these complex scenarios, an FDS ulnar slip excision is indicated to decompress the flexor sheath volume.
1. Using a blunt hook, the flexor tendons are gently elevated from the sheath.
2. The FDS tendon is identified superficial to the FDP.
3. The FDS bifurcates into radial and ulnar slips just distal to the A1 pulley. The ulnar slip of the FDS is carefully isolated using a right-angle clamp.


- Traction is applied to the ulnar slip, and a 1.5 to 2.0 cm segment of the slip is sharply resected.
- Following resection, the patient is again asked to actively flex and extend. The reduction in tendon volume almost universally resolves the residual impingement, restoring fluid, unimpeded motion.
5. Hemostasis and Closure
Following confirmation of a complete release and smooth tendon glide, the tourniquet (if used) is deflated. Meticulous hemostasis is achieved using bipolar electrocautery, taking extreme care to avoid thermal injury to the adjacent digital nerves.
The flexor sheath itself is left open; it is never repaired. The wound is copiously irrigated with sterile saline.

The skin is closed using interrupted 4-0 or 5-0 non-absorbable monofilament sutures (e.g., nylon). A bulky, soft sterile compressive dressing is applied, leaving the interphalangeal joints free to allow for immediate postoperative mobilization.
Complications, Incidence Rates, and Salvage Management
While A1 pulley release is generally considered a highly successful, routine outpatient procedure with excellent outcomes, complications can and do occur. A masterful surgeon must be prepared to recognize and manage these adverse events.
| Complication | Incidence Rate | Pathoanatomy / Cause | Salvage Management / Treatment |
|---|---|---|---|
| Digital Nerve Injury | < 1% | Direct laceration or thermal injury. The radial digital nerve of the thumb is at highest risk. | Immediate microsurgical primary epineural repair if recognized intraoperatively. Late presentation requires neuroma excision and nerve grafting or capping. |
| Tendon Bowstringing | Rare (< 0.5%) | Iatrogenic transection of the A2 (fingers) or Oblique (thumb) pulley. | Conservative: Extension block splinting. Surgical: Pulley reconstruction using palmaris longus autograft or extensor retinaculum. |
| Incomplete Release / Recurrence | 1 - 3% | Failure to release the proximal or distal-most fibers of the A1 pulley, or failure to recognize FDS hypertrophy requiring slip excision. | Re-exploration, completion of the A1 release under direct vision, and likely execution of an FDS ulnar slip excision. |
| Post-operative Stiffness / Flare | 5 - 10% | Tenosynovial flare, inadequate early mobilization, or pre-existing PIP joint contracture. | Aggressive hand therapy, dynamic extension splinting, short course of oral NSAIDs or oral corticosteroids. |
| Superficial Infection | 1 - 2% | Normal skin flora colonization of the surgical site. | Oral antibiotics (e.g., Cephalexin) covering staphylococcal and streptococcal species. Suture removal if localized abscess forms. |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of an A1 pulley release hinges not only on precise surgical execution but also on a rigorous, phased postoperative rehabilitation protocol. The primary goal is to prevent
