Postoperative Management and Rehabilitation in Total Hip Arthroplasty
Key Takeaway
Effective postoperative management following total hip arthroplasty (THA) is critical for optimizing functional recovery, ensuring implant stability, and minimizing complications. This evidence-based protocol encompasses immediate postoperative positioning, tailored weight-bearing guidelines based on fixation methods, and progressive rehabilitation. By integrating targeted physical therapy with strict dislocation precautions, surgeons can accelerate patient independence, restore abductor biomechanics, and achieve excellent long-term survivorship of the arthroplasty.
INTRODUCTION TO POSTOPERATIVE REHABILITATION IN TOTAL HIP ARTHROPLASTY
While total hip arthroplasty (THA) is widely regarded as one of the most successful surgical interventions in modern medicine, the surgical procedure itself is only one component of a successful outcome. There is no universally accepted, rigid postoperative rehabilitation program; however, the principles of early mobilization, biomechanical protection of the implant, and progressive functional restoration remain absolute. Although a pain-free hip can often be achieved with minimal postoperative effort, a meticulously constructed, evidence-based rehabilitation program significantly accelerates the recovery of motion and function, diminishes postoperative limp (Trendelenburg gait), and facilitates a rapid return to independent living.
The ultimate goal of postoperative management is to guide the patient through the phases of tissue healing and implant osteointegration while restoring the complex biomechanical milieu of the hip joint.
PREOPERATIVE OPTIMIZATION AND EDUCATION
Ideally, the rehabilitation continuum should commence well before the surgical incision is made. A concept often termed "prehabilitation," preoperative education and physical optimization are paramount. A patient who is highly motivated, thoroughly informed, and equipped with appropriate functional goals becomes an active participant in their own recovery process, rather than a passive recipient of care.
A dedicated preoperative session—often coordinated with physical and occupational therapy—should be utilized to instruct the patient on several critical elements:
* Transfer Mechanics: Safe techniques for moving from supine to sitting, and sitting to standing, without violating hip precautions.
* Assistive Devices: Proper sizing and preliminary training with walkers, crutches, or canes.
* Stair Negotiation: The classic "up with the good, down with the bad" methodology for navigating steps.
* Dislocation Precautions: Specific positional restrictions based on the planned surgical approach (e.g., avoiding combined flexion, adduction, and internal rotation for the posterior approach).
* Expectation Management: A realistic anticipated schedule for recuperation, hospital discharge, and return to work or sport.
IMMEDIATE POSTOPERATIVE MANAGEMENT (DAYS 0–2)
Positioning and Biomechanical Protection
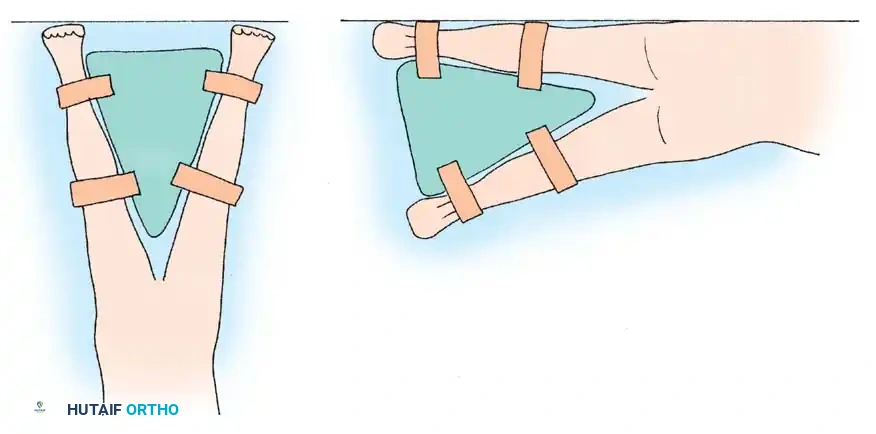
In the immediate postoperative period, particularly while the patient is recovering from anesthesia in the Post-Anesthesia Care Unit (PACU), meticulous attention must be paid to limb positioning. The operated hip should be positioned in approximately 15 degrees of abduction. This position maximizes the containment of the femoral head within the acetabular component and reduces tension on the repaired capsular and muscular structures.
To maintain this optimal alignment, a triangular abduction pillow is frequently utilized. This splint maintains abduction and prevents extremes of flexion, adduction, and internal rotation—the primary vectors for posterior dislocation.
Surgical Warning: While the triangular abduction pillow aids in safely rolling the patient onto the contralateral side in the early postoperative period, it must be applied with caution. The straps used to secure the device to the lower limbs must be positioned carefully to avoid undue compression over the fibular neck. Iatrogenic peroneal nerve palsy is a devastating and preventable complication caused by excessive strap pressure.
Early Mobilization and Bed Exercises
Most patients are sufficiently alert and comfortable to commence bed exercises and limited mobilization on the first postoperative day. Early intervention is critical for deep vein thrombosis (DVT) prophylaxis and the prevention of pulmonary complications.
Initial exercises include:
* Deep Breathing and Incentive Spirometry: To prevent basal atelectasis.
* Ankle Pumps: To enhance venous return and mitigate thromboembolic risk.
* Isometric Contractions: Quadriceps and gluteal sets to maintain muscle tone without loading the joint.
* Gentle Rotation Exercises: Within the safe, pain-free arc of motion.
Clinical Pearl: Straight leg raising (SLR), although highly beneficial after total knee arthroplasty, is strictly contraindicated in the early postoperative phase following total hip arthroplasty. SLR generates massive joint reaction forces (often exceeding 2.5 times body weight) due to the forceful contraction of the iliopsoas. This places unnecessary rotational and compressive stress on the femoral component, potentially compromising initial press-fit stability, and frequently results in severe anterior groin pain.
Patients should be instructed to perform these safe exercises for a few minutes every hour they are awake. Surgical drains, if utilized, are typically removed 24 to 48 hours after surgery, depending on output.
Sitting Protocols
On the first or second postoperative day, the patient is assisted to sit on the edge of the bed or in a chair in a semirecumbent position. Proper seating ergonomics are vital:
* One or two firm pillows should be placed in the seat of the chair to elevate the hips above the knees, thereby preventing excessive hip flexion (greater than 90 degrees).
* An additional pillow placed between the thighs limits adduction and internal rotation.
Because extended periods of sitting can be uncomfortable and promote anterior capsular tightness and hip flexion contractures, sitting sessions should be strictly limited to half-hour increments in the early recovery phase.
WEIGHT-BEARING PROTOCOLS AND IMPLANT FIXATION
Gait training usually begins on the first postoperative day. Most elderly patients require a standard or rolling walker for balance and stability, whereas younger, more agile patients may transition to crutches within a few days.
The amount of weight-bearing permitted on the operated limb is a critical decision that depends entirely on the biomechanical stability of the construct. Factors influencing this include the method of component fixation, the presence of structural bone grafts, intraoperative stress risers (e.g., cortical perforations or fractures), and the use of a trochanteric osteotomy.
Cemented Fixation
If the components are fully cemented, the polymethylmethacrylate (PMMA) mantle provides immediate mechanical interlock. Therefore, early weight-bearing to tolerance (WBAT) is universally permitted and encouraged.
Cementless (Porous Ingrowth) Fixation
The protocol for cementless implants has historically been a subject of debate. Biological fixation requires osteointegration—the direct ingrowth of bone into the porous coating of the implant. Excessive micromotion (greater than 150 micrometers) at the bone-implant interface can lead to fibrous encapsulation rather than true bone ingrowth.
- Conservative Approach: Many authors historically recommended limited weight-bearing (toe-touch or partial) for 6 to 8 weeks to protect the interface.
- Modern Evidence-Based Approach: With modern, fully porous-coated or highly porous metal implants achieving excellent initial press-fit stability, many surgeons now encourage immediate weight-bearing as tolerated. In a landmark study involving fully porous-coated cementless implants, Woolson and Adler demonstrated no difference in reliable bone ingrowth between patients allowed immediate weight-bearing as tolerated and a historical control group restricted to partial weight-bearing.
Ultimately, not all implants or host bone qualities are identical. The weight-bearing prescription must be individualized according to the specific implant design, the bone quality encountered intraoperatively, and the clinical judgment of the operating surgeon.
PROGRESSIVE PHYSICAL AND OCCUPATIONAL THERAPY
Ward-Based Gait Training
Gait training is preferably conducted directly on the hospital ward. Transporting postoperative patients to a distant physical therapy department in a wheelchair often leaves them fatigued, stiff, and uncomfortable before the therapeutic session even begins. Once the patient demonstrates the ability to walk far enough to reach the bathroom with supervision, bathroom privileges utilizing an elevated toilet seat are granted.
Stretching and Contracture Prevention
Hip extension exercises are strongly encouraged, particularly if the patient presented with a preexisting flexion deformity secondary to advanced osteoarthritis.
* Supine Positioning: The patient should spend dedicated time in the supine position each day. Pillows beneath the operative knee are strictly discouraged, as they promote hip and knee flexion contractures.
* The Thomas Test Stretch: The hip flexors can be stretched early by having the patient flex the contralateral (unoperated) hip to the chest while actively maintaining the operated limb flat against the bed.
* Prone Lying: After a few days, prone exercises can be initiated to provide a sustained, passive stretch to the anterior capsule and hip flexors. The patient should roll over their unoperated side with a pillow maintained between the legs to prevent adduction.
Occupational Therapy and ADLs
A few periods of targeted instruction by an occupational therapist are invaluable. Patients, particularly those who live alone, can return to independent living much sooner if they master safe techniques for Activities of Daily Living (ADLs). This includes dressing, donning shoes and socks, picking up objects from the floor, and personal hygiene. Numerous simple assistive appliances (e.g., reachers, sock aids, long-handled shoehorns) are available to facilitate these activities without violating hip precautions.
DISCHARGE CRITERIA AND TRANSITION OF CARE
Initiatives to optimize recovery and control the economic burden of THA have led to significantly shortened hospital stays. While traditional stays averaged 3 to 4 days, many modern enhanced recovery after surgery (ERAS) protocols allow for discharge within 24 to 48 hours, or even same-day discharge for highly selected candidates.
Standard criteria for hospital discharge include the patient's ability to:
1. Get in and out of bed independently.
2. Walk safely over level surfaces with an appropriate assistive device.
3. Climb and descend a few steps safely.
4. Understand and verbalize their home exercise program and dislocation precautions.
Printed instructions reviewing these protocols are essential. These must be supplemented with specific, individualized instructions from the surgeon regarding any particular positions of instability noted during the intraoperative trial reduction.
Patients with multiple joint involvement (e.g., severe polyarticular rheumatoid arthritis), preexisting neurological weakness, or other significant medical comorbidities may require an additional period of inpatient care at a subacute rehabilitation center. Carefully constructed transfer protocols detailing the exercise regimen, specific dislocation precautions, medical management, and DVT prophylaxis/anticoagulation make the transition of care seamless and safe.
THE SUBACUTE PHASE (WEEKS 1–6)
During the first 6 weeks post-surgery, the soft tissues (capsule, short external rotators, abductors) are actively healing. Patients must strictly adhere to the following guidelines:
* Seating: Continuous use of an elevated toilet seat and firm, high chairs.
* Sleeping: Use of one or two ordinary pillows between the knees when lying on the unoperated side to prevent the operative leg from falling into adduction and internal rotation.
* Hygiene: Showering is permitted once wound healing is deemed satisfactory (typically after suture/staple removal at 10-14 days, or immediately if waterproof dressings and absorbable sutures are used). A tub bath is permissible only if a dedicated shower stool is placed in the tub; a rubber mat and secure handrails are mandatory to prevent catastrophic falls.
* Sexual Activity: Can generally be resumed safely in the supine position, avoiding extreme flexion or rotation of the operative hip.
THE 6-WEEK MILESTONE AND OUTPATIENT FOLLOW-UP
The patient is typically evaluated in the outpatient clinic approximately 6 weeks after surgery. Routine orthogonal radiographs (AP pelvis and cross-table lateral) are obtained to assess component position, rule out subsidence, and evaluate early osteointegration.
Transitioning Assistive Devices
If the procedure was an uncomplicated primary arthroplasty and radiographic evaluation is satisfactory, crutches or the walker can be discontinued. The patient is then instructed in the use of a cane, held in the hand contralateral to the operated hip.
Biomechanical Pearl: Using a cane in the contralateral hand significantly reduces the joint reaction forces across the operated hip. By providing a long lever arm, the cane decreases the force required by the abductor musculature to maintain a level pelvis during the stance phase of gait, thereby minimizing implant stress and eliminating the Trendelenburg limp.
We encourage the continued use of a cane until all pain and limp have completely resolved.
If structural bone grafting was required (e.g., for acetabular dysplasia or revision surgery), or if the procedure was a complex revision, crutch use with protected weight-bearing may be continued for 3 months or longer, depending on the radiographic evidence of graft incorporation. In patients who have undergone multiple revision procedures with compromised abductor musculature, the permanent use of a cane may be advisable.
Advanced Rehabilitation
Strengthening exercises specifically targeting the abductor muscles (gluteus medius and minimus) are intensified to eliminate any residual limp. Stretching exercises are continued until the patient achieves sufficient functional range of motion to reach their foot for dressing and nail care. A safe method for foot dressing is to place the ankle of the operated limb resting on the opposite knee (a modified figure-of-four position), provided this does not violate specific anterior approach precautions if applicable.
Return to Driving
Patients who have undergone a left THA can usually resume driving an automatic vehicle at approximately 6 to 8 weeks, provided they are off narcotic analgesics. When the right hip has been operated on, the decision must be highly individualized. Return to driving depends on the objective return of muscular strength, precise leg control, and normalization of braking reaction time.
LONG-TERM RECOVERY AND FUNCTIONAL EXPECTATIONS (MONTHS 3–24)
Muscle Strength Kinetics
Surgeons and patients must recognize that recovery is a marathon, not a sprint. Gait analysis and force-plate data demonstrate that the recovery of strength in the periarticular musculature is a prolonged process. At 3 to 6 months post-surgery, abductor muscle strength is often still only 50% of normal. Long et al. reported persistent objective weakness in all patients at 2 years postoperatively, underscoring the absolute necessity for a prolonged, supervised, and dedicated home exercise regimen.
Return to Work
Many patients with sedentary, desk-based occupations can safely return to work after 6 to 8 weeks. At 3 months, patients can generally return to occupations requiring limited, controlled lifting and bending. However, we strongly discourage patients from returning to heavy manual labor after total hip arthroplasty, as repetitive heavy loading exponentially increases the risk of accelerated polyethylene wear and early aseptic loosening.
Athletic Participation
The resumption of athletic activity must be carefully counseled.
* Permitted Activities: Low-impact, cyclic activities such as swimming, stationary or level cycling, and golfing are highly acceptable and beneficial.
* Discouraged Activities: Jogging, singles tennis, racquetball, basketball, and other activities requiring repetitive impact loading, sudden cutting maneuvers, or extremes of hip positioning are unwise. Patients must be explicitly warned that such activities drastically increase the risk of accelerated bearing wear, osteolysis, and catastrophic failure of the arthroplasty.
Cardiovascular Benefits
Despite the restrictions on high-impact sports, overall cardiovascular fitness usually improves significantly following THA due to the restoration of pain-free mobility. Ries et al. found significant improvements in exercise duration, maximal workload, and peak oxygen consumption (VO2 max) in hip arthroplasty patients compared with matched controls treated non-operatively.
LONG-TERM SURVEILLANCE
Total hip arthroplasty requires lifelong surveillance. Standard follow-up visits are typically scheduled at 3 months, 6 months, and 1 year postoperatively, and periodically (every 1 to 2 years) thereafter.
Routine radiographs must be obtained at these intervals and meticulously compared with previous films. The surgeon must actively look for subtle signs of:
* Radiolucent lines indicating aseptic loosening.
* Component subsidence or migration.
* Eccentric positioning of the femoral head indicating polyethylene wear.
* Focal bone loss indicative of particle-induced osteolysis.
Regular, asymptomatic follow-up is essential because polyethylene wear and aggressive osteolysis frequently occur in the complete absence of clinical symptoms. If intervention is delayed until the patient experiences pain or catastrophic failure occurs, the subsequent revision arthroplasty becomes exponentially more difficult, with higher complication rates and inferior functional outcomes. Early detection of silent wear allows for simpler interventions, such as isolated modular bearing exchange, preserving the well-fixed components and the patient's bone stock.
===```
You Might Also Like