Unlock the Figure Posterior Approach to the Hip
Key Takeaway
Learn more about Unlock the Figure Posterior Approach to the Hip and how to manage it. The **figure posterior approach** to the hip is a surgical technique for primary and revision hip arthroplasty. It requires placing the patient in a lateral decubitus position and involves incising the gluteus maximus fascia, splitting the muscle, and taking down short rotators to expose the posterior capsule while protecting the sciatic nerve.
Introduction and Epidemiology
The posterior approach to the hip, often referred to as the Moore or Southern approach, remains the most widely utilized surgical corridor for access to the hip joint globally. Initially popularized by Austin Moore and Alexander Gibson, this approach has undergone numerous modifications to optimize exposure while minimizing soft tissue morbidity. It provides unparalleled, extensile access to the proximal femur and acetabulum, making it the workhorse approach for both primary and revision total hip arthroplasty (THA), hemiarthroplasty for femoral neck fractures, and the surgical management of posterior acetabular and femoral head fractures.
Epidemiologically, despite the recent surge in the popularity of the direct anterior approach, the posterior approach is still employed in the majority of primary THAs worldwide. Its widespread adoption is largely driven by its straightforward learning curve, excellent visualization of the femoral shaft, and the ability to extend the incision proximally or distally for complex primary or revision scenarios. The historical criticism of the posterior approach—namely, a higher rate of posterior dislocation—has been significantly mitigated by the advent of larger femoral head sizes, optimized component positioning, and the universal adoption of enhanced posterior soft tissue repair (EPSTR) techniques.



Understanding the nuances of this approach is foundational for any orthopedic surgeon. The posterior approach does not utilize a true internervous plane; rather, it relies on a muscle-splitting technique through the gluteus maximus. Despite this, the robust proximal neurovascular supply to the gluteus maximus ensures that a carefully executed split does not result in clinically significant denervation.
Surgical Anatomy and Biomechanics
A profound understanding of the posterior hip anatomy is critical for safe and effective execution of this approach. The dissection proceeds through distinct anatomical layers, each harboring specific neurovascular structures that must be respected.
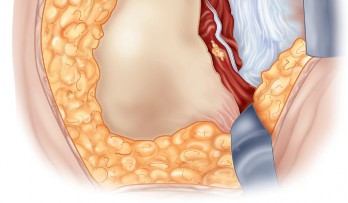
Superficial Fascial Layer and Gluteus Maximus
The superficial dissection involves incising the fascia lata distally and the gluteus maximus fascia proximally. The gluteus maximus is the largest muscle in the human body, serving as the primary extensor of the hip. It is innervated by the inferior gluteal nerve (L5, S1, S2) and receives its blood supply from the superior and inferior gluteal arteries. The surgical split is performed in line with its muscle fibers. Because the inferior gluteal nerve enters the muscle proximally and medially, splitting the muscle laterally and distally avoids denervation of the proximal muscle belly.



Deep Muscular Layer and Short External Rotators
Deep to the gluteus maximus lies the layer of the short external rotators and the posterior capsule. From cephalad to caudad, these include the piriformis, superior gemellus, obturator internus, inferior gemellus, obturator externus, and quadratus femoris.
The piriformis serves as a critical anatomical landmark. The superior gluteal neurovascular bundle exits the greater sciatic foramen superior to the piriformis, while the inferior gluteal neurovascular bundle, the sciatic nerve, and the posterior femoral cutaneous nerve exit inferior to it.
The short external rotators (piriformis, obturator internus, and the gemelli) converge to insert on the medial aspect of the greater trochanter. During the approach, these tendons are tagged and transected close to their insertion. This maneuver achieves two goals: it exposes the posterior joint capsule and creates a soft tissue sling that protects the sciatic nerve from posterior retractors.
Neurovascular Considerations
The sciatic nerve is the most critical structure at risk during the posterior approach. It typically courses anterior to the piriformis and posterior to the short external rotators. However, anatomical variations (Beaton and Anson classification) are present in approximately 15-20% of the population, where the nerve may pierce the piriformis or divide proximally, with the common peroneal division passing through or superior to the piriformis.
The medial femoral circumflex artery (MFCA) is the primary blood supply to the femoral head. Its deep branch courses between the pectineus and iliopsoas, traveling posteriorly to pass between the quadratus femoris and the inferior gemellus. When the quadratus femoris is released to enhance inferior exposure, the ascending branch of the MFCA is routinely encountered and must be meticulously coagulated to prevent postoperative hematoma.


Biomechanical Implications
The posterior approach disrupts the posterior stabilizing structures of the hip. The posterior capsule and the short external rotators act as a primary restraint against posterior subluxation during hip flexion, adduction, and internal rotation. The biomechanical integrity of the hip joint is significantly compromised if these structures are not adequately repaired. Modern EPSTR restores the resting tension of these muscles, effectively recreating the posterior soft tissue buttress and normalizing hip kinematics postoperatively.
Indications and Contraindications
The posterior approach is highly versatile, making it suitable for a wide array of orthopedic procedures. Its extensile nature allows for proximal extension into the ilium (Kocher-Langenbeck) or distal extension along the femoral shaft, providing comprehensive access for complex reconstructions.
Primary and Revision Arthroplasty
In primary THA, the posterior approach offers excellent visualization of the acetabulum and allows for straightforward preparation of the femoral canal. It is particularly advantageous in cases of severe proximal femoral deformity, where direct inline access to the femoral diaphysis is required. For revision THA, the posterior approach is considered the gold standard. It facilitates the removal of well-fixed femoral stems, allows for the execution of an extended trochanteric osteotomy (ETO), and provides adequate exposure for managing massive acetabular defects with augments or cages.




Trauma and Oncology
The approach is routinely utilized for the treatment of displaced femoral neck fractures via hemiarthroplasty or THA. In the realm of pelvic trauma, it is the foundation for the Kocher-Langenbeck approach to address posterior wall and posterior column acetabular fractures. Furthermore, it allows for the excision of benign and malignant tumors of the proximal femur and posterior acetabulum.
Summary of Indications and Contraindications
| Clinical Scenario | Operative Indication for Posterior Approach | Alternative Approach / Non-Operative Strategy |
|---|---|---|
| Primary Osteoarthritis | Standard primary THA | Direct Anterior or Anterolateral Approach |
| Revision Arthroplasty | Component extraction, ETO, massive bone loss | Direct Anterior (limited to simple revisions) |
| Femoral Neck Fracture | Displaced fractures requiring arthroplasty | Closed reduction and percutaneous pinning (CRPP) |
| Acetabular Fracture | Posterior wall / posterior column fractures | Ilioinguinal or Stoppa approach (anterior fractures) |
| Femoral Head Fracture | Pipkin I, II, IV fractures requiring fixation | Anterior approach (Smith-Petersen) for pure anterior lesions |
| Hip Infection | Irrigation and debridement, spacer placement | Suppressive antibiotics (if poor surgical candidate) |
Relative contraindications to the posterior approach include severe hip flexion contractures or ankylosing spondylitis with extensive anterior heterotopic ossification, where an anterior approach might provide more direct access to the pathology. Additionally, in patients with a history of recurrent posterior instability or severe neuromuscular disorders (e.g., cerebral palsy, Parkinson's disease), an anterolateral approach may be preferred to mitigate the risk of posterior dislocation.


Pre Operative Planning and Patient Positioning
Thorough preoperative planning is mandatory to ensure accurate restoration of hip biomechanics, including leg length, global offset, and the center of rotation.
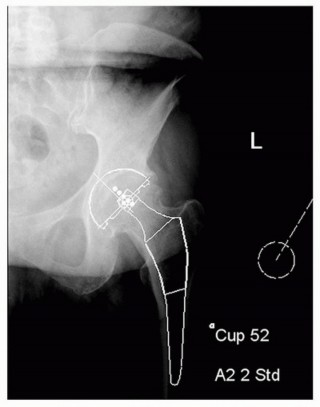
Radiographic Evaluation and Templating
Standard radiographic evaluation includes an anteroposterior (AP) view of the pelvis and an AP and cross-table lateral view of the affected hip. Digital templating is utilized to estimate the acetabular component size, assess the depth of the acetabulum, and determine the level of the femoral neck cut. The surgeon must meticulously evaluate the contralateral hip to establish the target leg length and femoral offset. High-resolution CT imaging may be indicated in cases of complex acetabular deformity, post-traumatic arthritis, or revision arthroplasty to assess bone stock and plan for augments.





Patient Positioning
The patient is placed in the lateral decubitus position on the operating table. Rigid pelvic fixation is essential; this is typically achieved using a peg board, a bean bag, or specialized pelvic positioners. The pelvis must be oriented strictly perpendicular to the floor to ensure accurate intraoperative estimation of acetabular version and inclination. The anterior superior iliac spine (ASIS) and the pubic symphysis should be aligned in the vertical plane.
The operative leg is draped free to allow for full range of motion during the procedure. Careful padding of all bony prominences, particularly the dependent peroneal nerve at the fibular head and the axilla, is imperative to prevent positioning-related neuropraxias.


Detailed Surgical Approach and Technique
The posterior approach requires meticulous surgical technique to optimize exposure while preserving the soft tissue envelope for subsequent repair.
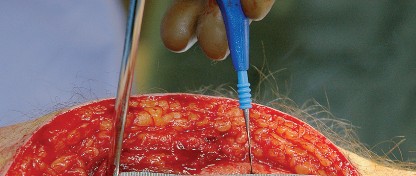
Incision and Superficial Dissection
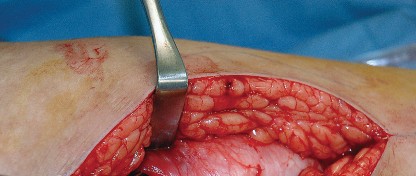
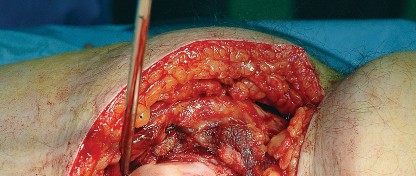
The skin incision is curvilinear, typically measuring 10 to 15 centimeters. It begins approximately 5 centimeters proximal and slightly posterior to the tip of the greater trochanter, curves distally over the posterior third of the trochanter, and extends longitudinally along the axis of the femoral shaft.
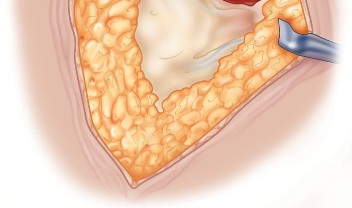
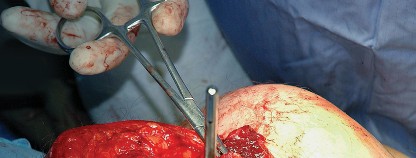
Subcutaneous tissues are divided in line with the skin incision to expose the fascia lata distally and the gluteus maximus fascia proximally. The fascia lata is incised longitudinally over the center of the greater trochanter. This fascial incision is extended proximally, splitting the fibers of the gluteus maximus bluntly. A Charnley or self-retaining retractor is placed beneath the fascial flaps to maintain exposure. A trochanteric bursa is routinely encountered and excised to clearly visualize the short external rotators.


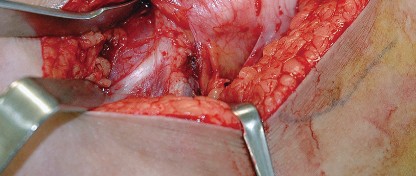

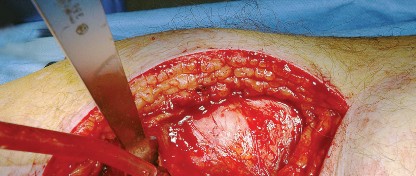
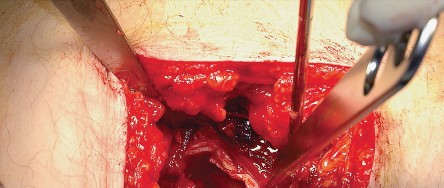
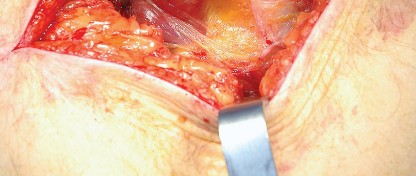
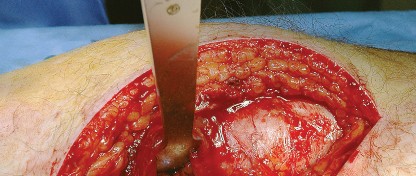
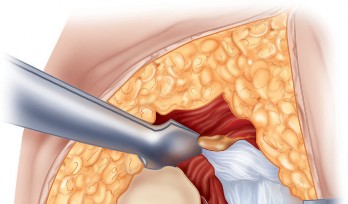
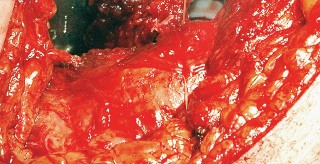
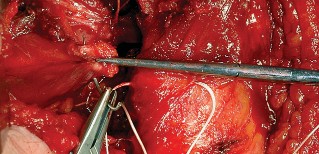
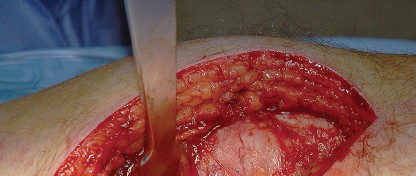
Deep Dissection and Sciatic Nerve Protection
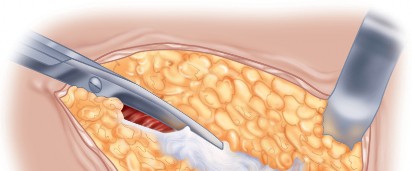
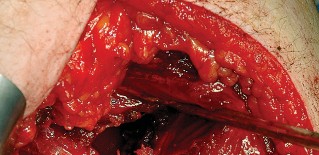
With the hip internally rotated, the short external rotators are placed under tension. The piriformis tendon is identified superiorly, and the quadratus femoris is identified inferiorly. The piriformis, superior gemellus, obturator internus, and inferior gemellus are tagged with heavy non-absorbable suture and transected approximately 1 centimeter from their insertion on the greater trochanter.
These tagged tendons are reflected posteriorly. This maneuver is critical as it creates a soft tissue barrier that shields the sciatic nerve from retractors and direct surgical trauma. The sciatic nerve itself does not routinely need to be formally exposed unless distorted anatomy or severe post-traumatic scarring is present. If additional inferior exposure is required, the proximal half of the quadratus femoris can be released, taking care to identify and ligate the ascending branch of the medial femoral circumflex artery.


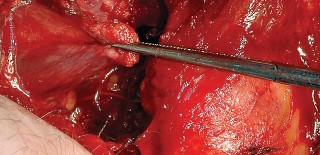
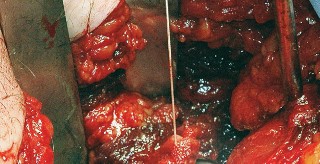
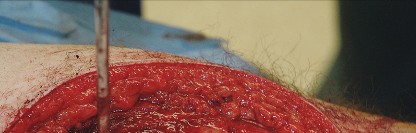
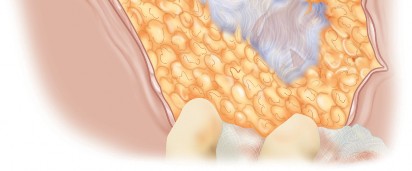
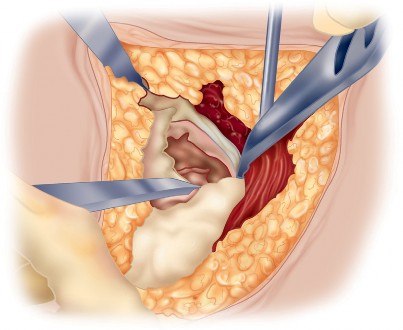
Capsulotomy and Hip Dislocation
The posterior joint capsule is now fully exposed. A capsulotomy or capsular flap is created. Many surgeons prefer a T-shaped or H-shaped capsulotomy, while others raise a continuous soft tissue flap comprising the capsule and the short external rotators. Regardless of the technique, preserving the capsular tissue is essential for later repair.
Once the capsulotomy is completed, the hip is gently dislocated through a combination of flexion, adduction, and internal rotation. Excessive force must be avoided to prevent iatrogenic fracture of the femoral shaft, particularly in osteoporotic bone.



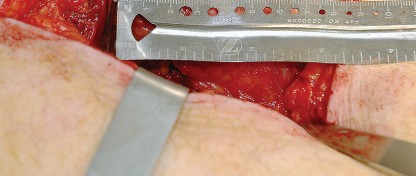
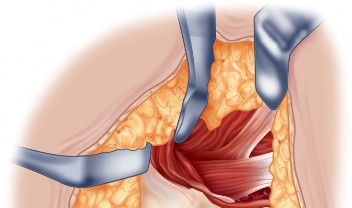
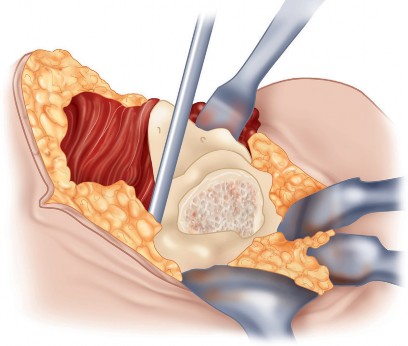
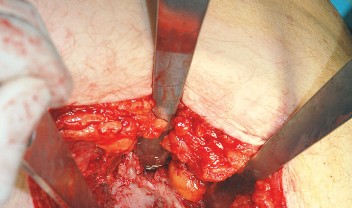
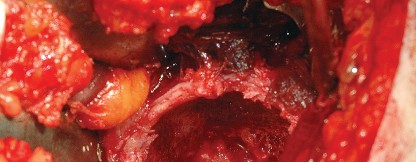
Acetabular and Femoral Preparation
Following dislocation, the femoral neck is osteotomized according to the preoperative template, and the femoral head is removed.
Acetabular exposure is achieved by placing a blunt retractor anteriorly over the anterior column, a retractor inferiorly beneath the transverse acetabular ligament, and a final retractor posteriorly to retract the capsule and femur. Complete excision of the labrum and visualization of the true acetabular floor (cotyloid fossa) are necessary to ensure proper reaming depth and component positioning.
For femoral preparation, the leg is positioned in flexion, adduction, and marked internal rotation. A retractor is placed under the proximal femur to elevate it out of the wound. The femoral canal is then sequentially broached. The posterior approach provides excellent, inline access to the femoral diaphysis, reducing the risk of varus malpositioning of the femoral stem.




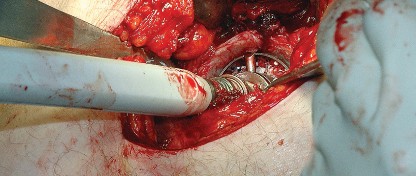
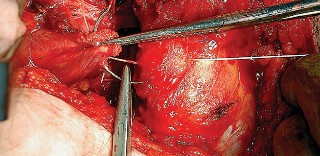
Enhanced Posterior Soft Tissue Repair
Following the insertion of the final components and reduction of the hip, meticulous closure is paramount. Enhanced posterior soft tissue repair (EPSTR) involves reattaching the posterior capsule and the short external rotators to the greater trochanter. This is typically accomplished using heavy transosseous sutures passed through drill holes in the posterior edge of the greater trochanter. This robust repair restores the posterior tension band, significantly reducing the incidence of postoperative dislocation. The fascia lata and gluteus maximus fascia are then closed tightly, followed by standard subcutaneous and skin closure.



Complications and Management
While the posterior approach is generally safe and reproducible, specific complications can arise. Recognition and appropriate management of these complications are critical for optimal patient outcomes.
Instability and Dislocation
Historically, the posterior approach was associated with a higher rate of posterior dislocation compared to the anterolateral or direct anterior approaches. However, the routine implementation of EPSTR, combined with the use of larger femoral heads (32mm, 36mm, or dual mobility constructs) and precise component positioning, has reduced the dislocation rate to less than 1%, comparable to other surgical approaches. Management of a posterior dislocation initially involves closed reduction under conscious sedation or general anesthesia. Recurrent instability may necessitate revision surgery to correct component malposition, increase femoral head size, or utilize constrained liners.



Sciatic Nerve Palsy
Sciatic nerve injury is a devastating complication, occurring in approximately 0.5% to 2% of primary THAs and up to 5% of revision cases. The common peroneal division is most susceptible to injury due to its lateral position and relative tethering. Mechanisms of injury include excessive retractor tension, direct laceration, thermal injury from cement, or postoperative hematoma. Intraoperative monitoring (SSEP/MEP) may be utilized in high-risk cases. If a postoperative palsy
Clinical & Radiographic Imaging






You Might Also Like